Article Text

Abstract
Objectives To monitor progression to inflammatory arthritis (IA) in individuals with non-specific musculoskeletal (MSK) symptoms and positive anticyclic citrullinated peptide (anti-CCP) antibodies. To develop a pragmatic model to predict development of IA in this patient group.
Methods In this prospective observational cohort, patients with new non-specific MSK symptoms and positive anti-CCP were recruited from regional primary care and secondary care referrals. Clinical, imaging and serological parameters were assessed at baseline. Cox regression analysis was performed to identify predictors of progression to IA and develop a risk score to stratify patients at presentation.
Findings 100 consecutive patients (73 women, mean age 51 years) were followed up for median 19.8 months (range 0.1–69.0); 50 developed IA after a median 7.9 months (range 0.1–52.4), 34 within 12 months. The majority (43/50) fulfilled the 2010 American College of Rheumatology/European League Against Rheumatism criteria for rheumatoid arthritis. A model for progression to IA was devised using four variables: tenderness of hand or foot joints, early morning stiffness ≥30 min, high-positive autoantibodies, and positive ultrasonographic power Doppler signal. None of the five individuals at low risk (score 0) progressed to IA, compared with 31% of 29 at moderate risk (1–2) and 62% of 66 at high risk (≥3). Adding shared epitope increased the number at low risk (score 0–1; 0/11 progressed).
Conclusions In patients presenting with non-specific MSK symptoms and anti-CCP, the risk of progression to IA could be quantified using data available in clinical practice. The proposed risk score may be used to stratify patients for early therapeutic intervention.
Trial registration number NCT02012764 at ClinicalTrials.gov.
- Ant-CCP
- Autoantibodies
- Early Rheumatoid Arthritis
- Rheumatoid Arthritis
- Ultrasonography
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic autoimmune disease with a substantial socio-economic burden in terms of direct costs to healthcare providers and indirect costs related to lost productivity, increased morbidity and premature mortality.1 Early diagnosis and intervention with disease modifying antirheumatic drugs (DMARDs) have been established as the best strategy to prevent joint destruction and preserve function.2–4
Several studies have identified a preclinical phase of seropositive RA characterised by increased levels of circulating autoantibodies including rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPAs).5–10 In clinical practice, ACPA positivity is defined by measuring antibodies against synthetic cyclic citrullinated peptide (CCP). Anti-CCP antibodies are more specific markers for RA than RF and have been detected in the sera of asymptomatic blood donors up to 14 years prior to disease onset.5 ,6 However, the 5-year risk of developing RA in the general population with positive anti-CCP was found to be only 5%.5 This long transition from asymptomatic anti-CCP status to inflammatory arthritis (IA) means screening for autoantibodies is unlikely to be cost-effective unless predictive factors can be identified. Certain factors have been associated with a more rapid transition to RA including smoking, obesity, prolonged early morning stiffness (EMS), raised inflammatory cytokines and the presence of human leucocyte antigen (HLA)-DRB1.7 ,11–15 Sensitive imaging, proven to be superior to clinical examination in the detection of low level joint inflammation,16 has produced inconsistent results in preclinical populations with low progression rates.
Our understanding of the period in anti-CCP positive individuals prior to development of RA has improved in recent years. Notably, a phase of imminent RA has been demonstrated to occur within 2 years of RA onset,17 characterised by rising ACPA titres and expansion of the number of citrullinated epitopes recognised by ACPAs (epitope spreading).18 ,19 In addition, from our personal observation, this phase is characterised by more frequent primary care attendance with non-specific musculoskeletal (MSK) symptoms. This observation is supported by recent findings that patients with RA visited their general practitioner (GP) on average four times before being referred to a specialist for diagnosis, and 18% of patients visited their GP more than eight times in the period preceding diagnosis.20 It was our hypothesis that anti-CCP testing in patients who present with new non-specific MSK presentations would select a population enriched for imminent RA. Identifying patients at this early phase should produce the best clinical outcome by early diagnosis and treatment, and may also permit the possibility of preventive therapy.
The first aim of this study was to investigate the rate and timing of progression to IA in anti-CCP positive individuals presenting with new onset non-specific MSK symptoms. Our second aim was to develop a scoring system to predict progression to IA in this group using clinical, serological and imaging parameters.
Patients and methods
Patients were recruited from primary care services in Yorkshire, UK. We also recruited patients from the rheumatology early arthritis clinic in Leeds if they were found to have no clinical evidence of inflammatory joint swelling (deemed IA). The primary care recruitment was adopted by the UK Primary Care Clinical Research Network21 and the study was approved by the local ethics committee. Patients aged >18 years presenting to their GPs or other health professionals (eg, physiotherapy or podiatry) with new onset MSK symptoms were invited to participate. All participants signed an informed consent form before taking part. For patients referred from primary care, the anti-CCP test was performed centrally at the Rheumatology Department in Leeds using a standard commercially available anti-CCP2 (immunocap method; Phadia, Sweden, Germany). Those with a positive test were invited to a dedicated research clinic at Chapel Allerton Hospital, Leeds. The following exclusion criteria were applied: history of IA diagnosed by a rheumatologist; presence at baseline of clinically detected IA confirmed by a rheumatologist; and use of DMARDs.
Assessment
Patients were assessed at baseline, at 3-monthly intervals for the first year, and then as clinically indicated or until they developed IA defined by the presence of at least one tender and swollen joint confirmed by a rheumatologist. Patients could also be seen between these visits if they developed new joint symptoms. The clinical assessments were carried out by a group of rheumatologists who completed the eligibility criteria, clinical examinations and fulfilment of IA.
Clinical and demographic assessment
The following clinical and demographic parameters were recorded at baseline: age, gender, body mass index (BMI), smoking history, alcohol intake, history of first degree relative(s) with RA, duration of EMS in minutes, 44 tender joint count and the Ritchie articular index (scores 0–78), tenderness of the small joints of the hands and feet (wrists, metacarpophalangeal (MCP), proximal interphalangeal (PIP), midtarsal and/or metatarsophalangeal joints) defined by the physician on examination, joint symptoms in the upper and lower extremities, pain visual analogue scale (VAS), and the presence of intermittent symptoms.
Biomarkers
A number of biomarkers were measured at baseline. HLA-DRB1 shared epitope status was considered positive with the presence of one or two copies of the following alleles: HLA- DRB1*01, DRB1*04 and DRB1*10 in the HLA-DRB1 locus.22 ,23 For antibody tests, reference ranges in the laboratory changed partway through recruitment. Immunoglobulin M RF levels were measured and the cut-off for positive test was initially 40 IU/mL, and later 20 IU/mL. Anti-CCP antibody levels (anti-CCP2; immunocap assay, Phadia) were also measured with a cut-off of 7 IU/mL initially, and later 2.99 IU/mL. The status of high-level RF or anti-CCP was defined according to the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) 2010 criteria by a cut-off level of >3 times the upper limit of normal.24 High sensitivity C reactive protein was performed and levels ≥2 mg/dL, which have been associated with disease activity in RA, were considered positive.25 Ultrasound examination of the wrists, MCPs and PIPs was performed by a rheumatologist experienced in MSK ultrasound, using a commercially available machine (ATL HDI 5000, Philips) with 12–5 MHz and 15–8 MHz transducers. Power Doppler (PD) was reported as positive with the presence of intra-articular Doppler signal (total PD ≥1) using a standard method.26 ,27 Intrareader reliability for the assessor performing the ultrasound scanning has been reported to be excellent, with 100% agreement between two repeated assessments of the presence of PD signal in 33 joints.28
For sample size, we opted to assess the potential predictive utility of the variables collected in the first 100 patients, based on an estimate that 40%–50% of patients would progress. This would allow us to estimate the unadjusted HRs for the full set of potential predictors and to trial a clinically relevant simplified four-variable model. Published rules of thumb for Cox regression recommend 10 events per variable.29
Statistical analysis
Baseline variables were assessed for their association with time to progression to IA using univariable Cox regression analyses to obtain unadjusted HR. Clinically relevant cut-offs were used to dichotomise continuous variables. In addition to those listed above, cut-offs of ≥25 for BMI, ≥12 months for symptom duration, ≥50 mm for pain VAS and ≥30 min for EMS were used. Further details of the cut-offs used for continuous predictors can be found in the online supplementary material. Variables were coded so that the HR was positive in each case; HR≥1.5 was considered substantive when selecting variables to include in the multivariable model. Cases were treated as censored after their last follow-up if they had not progressed to IA.
Multivariable Cox regression
To develop a risk stratification score, variables were considered for inclusion in a multivariable model of time to progression if they were (a) potentially available in clinical practice and (b) related to the outcome to a substantive degree (HR≥1.5). After fitting the model, each variable was given a score derived from its regression coefficient, rounded to the nearest 0.5 interval and then multiplied by 2. A patient's total score depended on which risk factors were present at baseline. Risk categories were then defined according to the proportions of patients progressing at each score level.
Results
Baseline clinical and demographic characteristics are presented in table 1. A total of 100 patients were included—71 from early arthritis clinic referrals and 29 from primary care referrals. A flow chart of participants is presented in figure 1. Individuals who met inclusion criteria at the point of referral but were found to have IA at the baseline assessment were excluded (n=21). The 100 individuals included in the analysis were followed up for a median of 19.8 months (1st quartile=7.6, 3rd quartile=34.4; range 0.1–69.0). Fifteen were lost to follow-up from the research clinic; however, we were able to confirm from their clinical records or with their GPs that they had not developed IA. Using point of last consultation or GP contact to determine the duration of follow-up in these patients, all but one had been followed for at least 12 months.
Baseline demographic, clinical and imaging characteristics of 100 anti-CCP positive patients with non-specific MSK symptoms
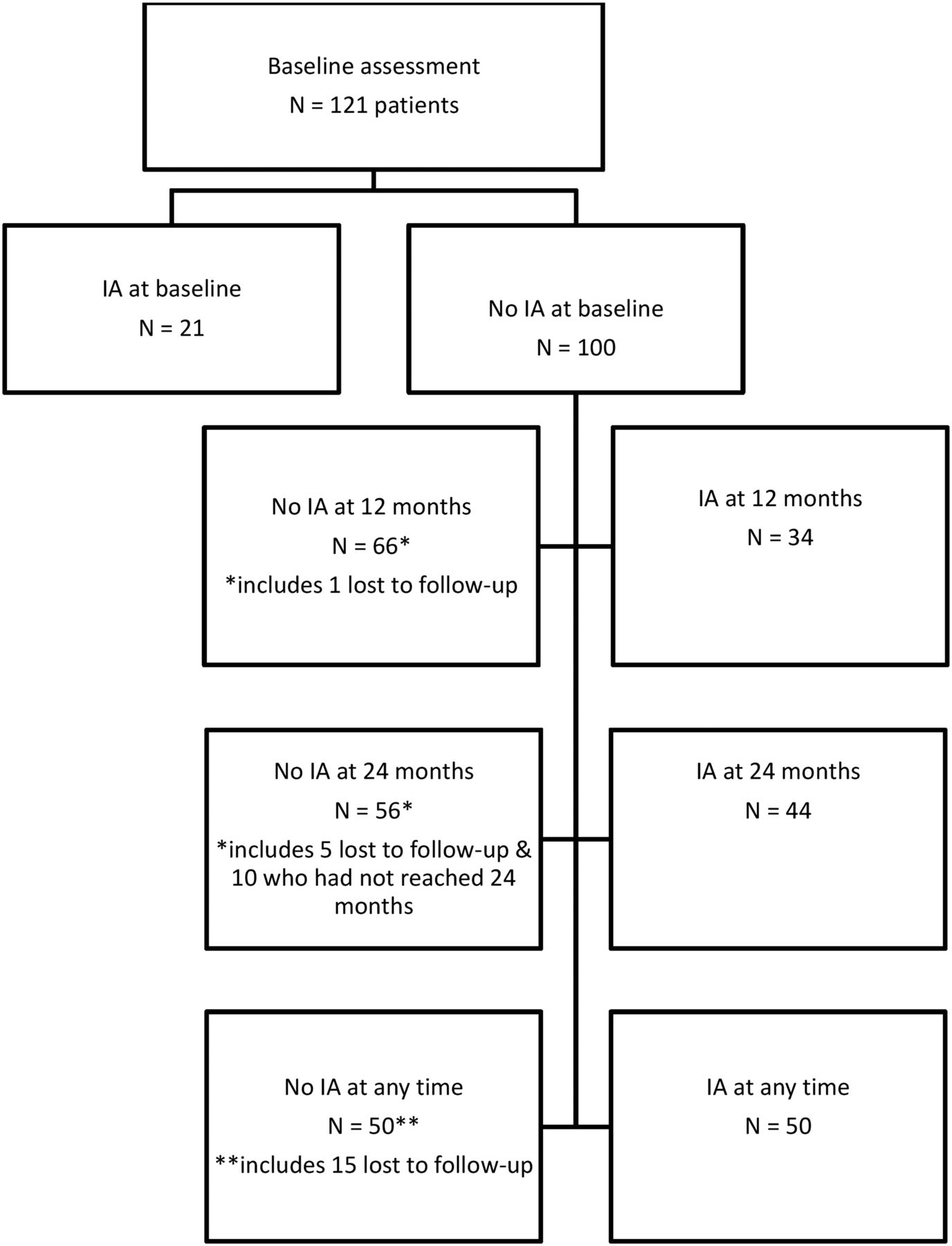
Flowchart of the study patients. IA, inflammatory arthritis; **details of the 15 patients lost to follow-up from the research clinic, obtained from their clinical records or with their general practitioners showed that none had developed IA at their last clinic appointments.
Progression to IA
In total, 50 participants progressed to IA detected clinically after a median of 7.9 months (IQR 3.2, 14.5; range 0.1–52.4); 34 did so within the first 12 months of follow-up, and 44 within the first 24 months (figure 1). Overall, 43 of those who progressed to IA fulfilled the 2010 ACR/EULAR RA classification criteria; the remaining had undifferentiated IA. Those who did not progress were followed up for a median of 30.3 months (IQR 22.5, 45.1; range 7.7–69.0).
Univariable Cox regression analysis
Two clinical parameters were substantively associated with increased risk of progression to IA: tenderness of small joints and EMS lasting ≥30 min (table 2). We considered 30 and 60 min as cut-off points for EMS and both showed similar predictive values. Therefore, we opted for the 30 min which is more sensitive and may detect patients at an earlier stage of the disease.30
Associations among baseline demographic, clinical and imaging characteristics and time to development of IA in 100 anti-CCP positive patients with non-specific MSK symptoms
All of the following biomarkers were associated with increased risk of progression: presence of shared epitope, positive RF, high positive anti-CCP or RF, and positive PD on ultrasound.
Multivariable Cox regression
Of the variables found to be substantively associated with progression in univariable analysis (HR ≥1.5), only those possibly available in clinical practice were considered for inclusion in the multivariable models of progression. Ultrasound was initially chosen over the shared epitope due to its wider availability and lower cost in the UK; however, we explored whether shared epitope would also be predictive, with or without PD, to allow for differences in the availability of each test.
The first model of progression to IA up to 69 months of follow-up (PD model, tables 3 and 4) included 100 patients, 50 of whom progressed. The independent variables were presence/absence of small joint tenderness, EMS ≥30 min, high level RF and/or anti-CCP, and PD. The proportional hazards assumption was tested by adding time-varying covariates to each model 31 and found to be satisfied. We used Harrell's C to assess the predictive strength of the model.32 This statistic assesses whether the ordering of the predicted progression times is in agreement (concordant) with the observed data; values >0.5 indicate predictive ability better than random chance and 1 represents perfect concordance. For this model Harrell's C was 0.67 (0.59, 0.74). All four variables were substantively associated with the risk of progression to IA (HR ≥1.5; table 3), although none to a statistically significant degree. However, the model residuals revealed two unduly ‘influential’ individuals (dfbeta >2/√N), both of whom were low positive for anti-CCP and had no PD signal present but progressed to IA. When these two individuals were excluded, the HRs increased to the extent that EMS, antibody level and PD were all independently associated with time to progression.
Results of multivariable Cox regression models of time to progression to inflammatory arthritis during up to 69 months of follow-up; scores for each predictor were derived from the regression coefficients, rounded to nearest 0.5 then multiplied by 2, to give a total risk score ranging from 0 to 5
Proportions of patients progressing to inflammatory arthritis (IA) within 12 or 24 months of referral, or at any time during follow-up, according to their risk score at baseline
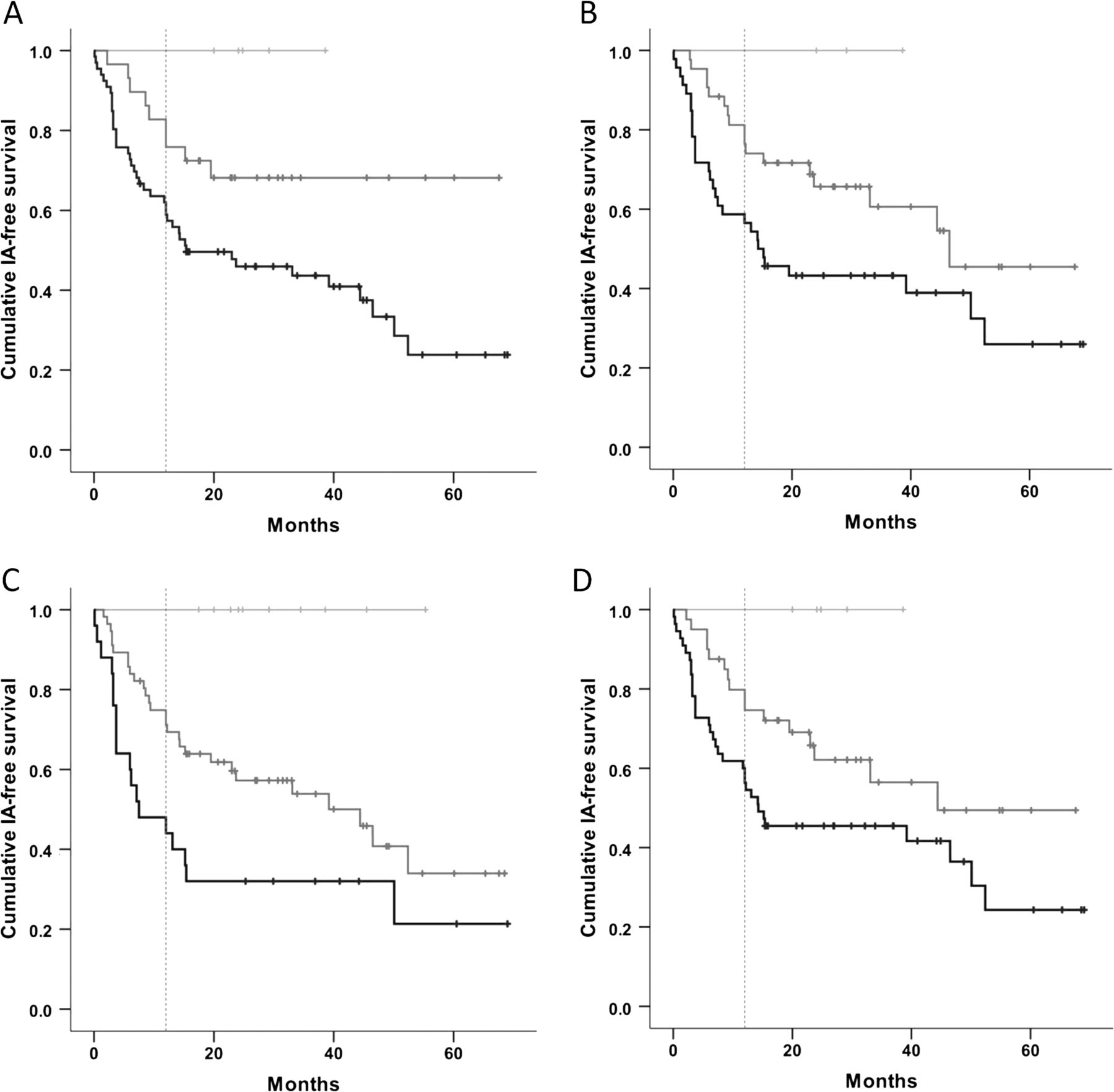
The resulting risk score ranged from 0 to 5 (table 3). The proportions progressing to IA, according to risk score (table 4), suggested that three risk groups could be defined. Anti-CCP antibody positive individuals exhibiting none of the four risk factors at baseline could be considered at low risk of progression (0/5 progressed), while those scoring 1–2 points could be pooled into a moderate risk group (31% of 29 subjects progressed), and those scoring 3 or above could be pooled into a high risk group (62% of 66 subjects progressed). The majority of those who progressed did so within the first 12 months (table 4). Figure 2A illustrates the three different risk groups and their Kaplan–Meier IA-free survival curves over up to 69 months of follow-up.
{kind=link}
{kind=link}
Conditional probability of inflammatory arthritis (IA)-free survival over up to 69 months of follow-up, according to categories of risk derived from exploratory risk scores for progression to IA; crosses indicate censoring due to loss to follow-up (n=15) or duration of follow-up <69 months without progression to IA (n=35). The majority of those who progressed did so within the first 12 months (dotted line). Four different models are presented ((A) power Doppler; (B) shared epitope; (C) power Doppler and shared epitope; (D) neither power Doppler nor shared epitope). Black line=high risk of progression to IA; mid-grey=moderate risk; light grey=low risk.
Alternative models including shared epitope were constructed and found to have similar predictive ability (tables 3 and 4; figure 2B–D; see online supplementary material for further details of these models).
Discussion
With the wider availability of anti-CCP testing, the management of individuals with disease specific antibodies and non-specific symptoms is an increasingly common problem. A major hindrance to developing satisfactory guidelines for such individuals has been the inability to predict transition to clinical disease. For RA, early identification and treatment are crucial since joint damage occurs early,33 and therapy is most effective at this stage resulting in less radiographic progression over time.3 ,34–36
In this cohort, half of the anti-CCP positive individuals developed IA, most of them within 12 months of presentation with a median time of 7.9 months corresponding to what has been labelled imminent RA. Those who progressed to IA had distinctive clinical features and biomarker profiles at presentation. Clinically, they were more likely to report EMS≥30 min and to have tenderness of small joints at baseline. They were more likely to have high positive RF and/or anti-CCP, shared epitope, and positive PD on ultrasound scan.
The current study has its limitations. Although it is one of the larger prospective cohorts of individuals at risk followed up from an early phase of anti-CCP positivity and non-specific symptoms to the development of IA, the number of patients is still relatively small to allow for full multivariable analyses. Nonetheless, for the first time in individuals at risk of RA, this study derived a risk score model incorporating clinical, serological and imaging parameters. The predictive value of ultrasound highlights a potential role of this imaging modality in the assessment and stratification of individuals at risk. Ultrasound PD signal has been shown to detect subclinical inflammation and in one study predicted RA flares in patients in apparent clinical remission.37
Our results support previous research findings in which anti-CCP antibodies have been associated with a significantly increased risk of developing IA.7 ,12 ,38 ,39 The rate of progression in our cohort (50%) is higher than that reported in another recent study of individuals at risk (35%).12 This may be explained by different inclusion criteria between the studies; in particular, only 83% of patients in the previous study were anti-CCP positive.12 A comparison of predictors between the two cohorts showed similar predictive abilities of a number of variables—small joint involvement, prolonged EMS and antibody status. However, the presence of a first degree relative with RA, symptom duration of <12 months and no alcohol intake were only reported to be predictors of transition to IA in the study by van de Stadt et al.12 Findings of imaging biomarkers to predict the development of IA in previous studies have been inconsistent. In one study of individuals with anti-CCP and/or RF antibodies without evidence of arthritis, MRI of the knee joint was not predictive of progression compared with controls.40 In another study, ultrasound of painful joints and/or the joints of hands and feet was only predictive of arthritis development at the joint but not the patient level.41
The present study highlights the role of biomarkers in individuals at risk of RA. Furthermore, a simplified risk score has been developed using variables potentially available in clinical practice. This scoring system is easy to use and may aid in screening individual patients presenting with non-specific MSK presentations and a positive anti-CCP. Physician-defined tenderness of small joints of the hands and feet, prolonged EMS and positive RF and anti-CCP antibodies have face validity as they have previously been demonstrated to be predictors of both persistent and erosive arthritis42 as well as the transition from undifferentiated IA to RA.43 While not available within all rheumatology services, MSK ultrasound is becoming increasingly accessible in clinical practice.
In addition, to allow for differences in availability, we performed risk scores with/without shared epitope and PD. The results demonstrated similar predictive performance of the four derived models with regard to low risk (0% in all models) and high risk (62%–72% progression) categories. However, the model with both shared epitope and PD allowed more patients to be classified at low risk. These results would suggest that individuals may be screened at presentation with a simplified model using clinical data and antibodies and those with moderate risk could be referred for further advanced testing.
In summary, this study confirms that patients with anti-CCP antibodies and MSK symptoms are at risk of developing RA. The risk score derived from this cohort is a step towards achieving a personalised medicine approach to identify those patients at an early stage. This is particularly true for those with a moderate risk score who, once identified through a basic screen, could have their risk estimate refined by further targeted testing. This risk score model will need to be confirmed in a larger cohort with a wider and universally applied set of predictors.
Acknowledgments
We would like to thank the GPs, health professionals and UK Primary Care Research Network (UK PCRN) for their help with recruitment of the study, and Ged Connolly-Thompson, Andrea Paterson and Jonathan Thompson for their IT support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
CR and JLN are joint first authors.
Contributors All authors actively participated in conducting the study, contributed to the critical revisions to the manuscript and approved the article for publication.
Funding This study presents independent research supported by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. This study was supported by AbbVie who provided funding for anti-CCP testing.
Competing interests EMAH is supported by institution-level grants from Arthritis Research UK and the National Institute of Health Research.
Patient consent Obtained.
Ethics approval Leeds Research Ethics Committee, UK.
Provenance and peer review Not commissioned; externally peer reviewed.