Article Text

Abstract
Objectives To investigate whether bortezomib, a proteasome inhibitor approved for treatment of multiple myeloma, induces clinically relevant plasma cell (PC) depletion in patients with active, refractory systemic lupus erythematosus (SLE).
Methods Twelve patients received a median of two (range 1–4) 21-day cycles of intravenous bortezomib (1.3 mg/m2) with the coadministration of dexamethasone (20 mg) for active SLE. Disease activity was assessed using the SLEDAI-2K score. Serum concentrations of anti–double-stranded DNA (anti-dsDNA) and vaccine-induced protective antibodies were monitored. Flow cytometry was performed to analyse peripheral blood B-cells, PCs and Siglec-1 expression on monocytes as surrogate marker for type-I interferon (IFN) activity.
Results Upon proteasome inhibition, disease activity significantly declined and remained stable for 6 months on maintenance therapies. Nineteen treatment-emergent adverse events occurred and, although mostly mild to moderate, resulted in treatment discontinuation in seven patients. Serum antibody levels significantly declined, with greater reductions in anti-dsDNA (∼60%) than vaccine-induced protective antibody titres (∼30%). Bortezomib significantly reduced the numbers of peripheral blood and bone marrow PCs (∼50%), but their numbers increased between cycles. Siglec-1 expression on monocytes significantly declined.
Conclusions These findings identify proteasome inhibitors as a putative therapeutic option for patients with refractory SLE by targeting PCs and type-I IFN activity, but our results must be confirmed in controlled trials.
- Systemic Lupus Erythematosus
- Autoimmune Diseases
- B cells
- Treatment
- Autoimmunity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The resistance of long-lived plasma cells (PCs) to conventional and B-cell-depleting therapies constitutes a therapeutic challenge in antibody-mediated autoimmune diseases, such as systemic lupus erythematosus (SLE).1 ,2
Proteasome inhibition is one of the most promising therapeutic approaches to target PCs, since this strategy has been shown to efficiently eliminate multiple myeloma cells, that is, transformed PCs.3–5 Proteasome inhibition blocks antiapoptotic nuclear factor kappa B (NF-κB) activation and causes accumulation of misfolded proteins within the endoplasmic reticulum thereby activating the terminal unfolded protein response leading to apoptosis.3 ,4 Due to their extremely high rate of antibody synthesis, PCs are particularly sensitive to proteasome inhibition. Bortezomib, a proteasome inhibitor approved for the treatment of multiple myeloma, reversibly binds to the 26S proteasome and inhibits its chymotrypsin-like activity. Proteasome inhibition has been demonstrated to deplete short-lived and long-lived PCs in lupus-prone mice, resulting in reduced nephritis and markedly prolonged survival.6 More recently, next-generation proteasome inhibitors delanzomib and carfilzomib were also shown to effectively reduce autoantibody levels and inhibit type-I interferon (IFN) production in lupus-prone mice.7 ,8 Given the promising results of experimental lupus models and first experiences with proteasome inhibition for allograft rejection in kidney transplantation,9 ,10 patients with SLE with persistent disease activity and autoantibody production despite immunosuppressive treatment received bortezomib according to the approved protocol for multiple myeloma.3 Here, we describe the clinical features of 12 patients treated with bortezomib, in correlation to serological responses and flow cytometric findings.
Patients and methods
Patients and methods and any associated references are available in the online supplement.
Results
Bortezomib is clinically effective in refractory SLE
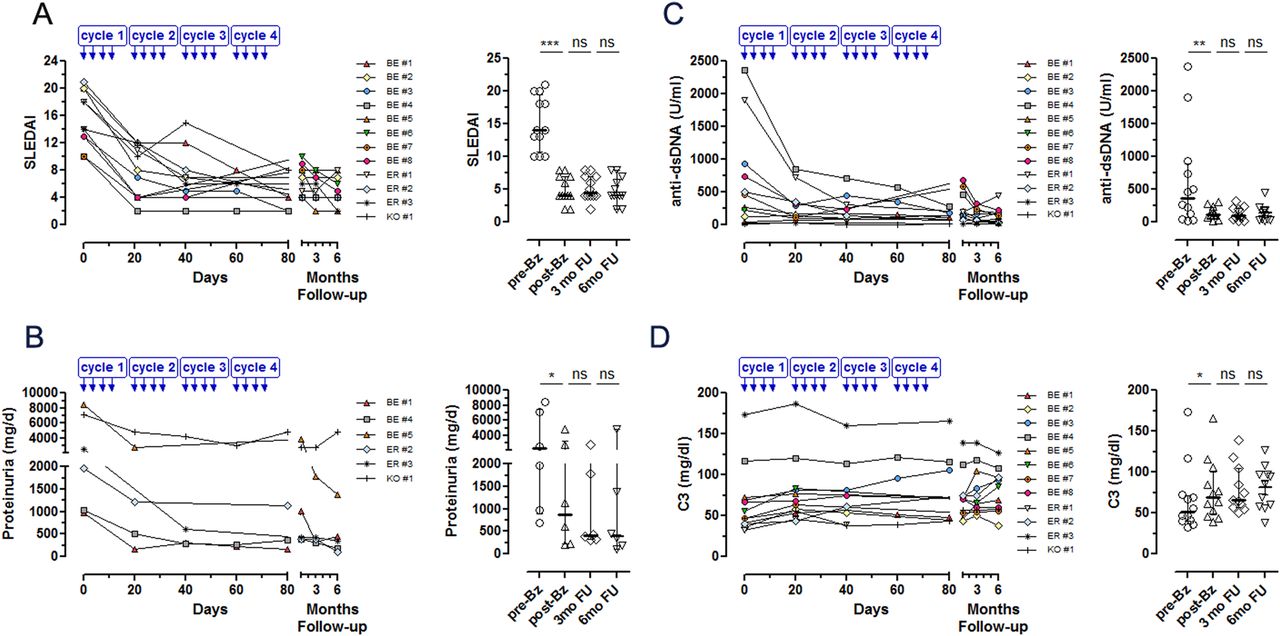
Patients received one to four (median: two) cycles of bortezomib, depending on their individual tolerance and treatment response. Upon proteasome inhibition, all patients showed significant clinical improvement, as reflected by a significant reduction of Systemic Lupus Erythematosus Disease Activity (SLEDAI) score from a median 14 at baseline to 4 after the last bortezomib cycle (p<0.001, figure 1A). In all affected patients musculoskeletal and mucocutaneous manifestations improved, pericardial effusions regressed (see online supplementary figure S1), and proteinuria levels decreased from a median of 2221 to 867 mg/day (p=0.012, figure 1B). Detailed responses of clinical manifestations are shown in online supplementary figure S2. A significant change-point in SLEDAI reduction was detected after the first 21 days of proteasome inhibition (p<0.001), suggesting that most of the clinical improvement was achieved during the first bortezomib cycle.

Proteasome inhibition with bortezomib is clinically effective in refractory systemic lupus erythematosus (SLE) patients. (A) SLE Disease Activity Index (SLEDAI-2K), (B) proteinuria (mg/day) in nephritis patients, (C) serum anti-dsDNA antibody concentrations and (D) serum complement C3 concentrations in patients with SLE before and after each cycle of bortezomib treatment. Median/IQR values are shown for each category at baseline before bortezomib treatment (pre-Bz), after the last bortezomib cycle (post-Bz) and 3 months (3 months follow-up, FU) and 6 months (6 months follow-up, FU) following the last bortezomib cycle.
When maintenance therapy was reintroduced after a median of 41 days (range, 1–61 days), disease activity remained stable for 6 months following the last bortezomib cycle despite prednisolone tapering from a median dose of 20 mg/day at baseline to 7.5 mg/day (figure 1A). Notably, seven patients became responsive to immunosuppressive therapies that had initially failed to control disease activity (see online supplementary table S1). In patients receiving bortezomib without coadministration of dexamethasone (n=4), disease activity also markedly decreased, as reflected by SLEDAI score reduction from a median of 15.5 at baseline to 10 after the last bortezomib cycle (see online supplementary table S2).
Reductions in pathogenic and vaccine-induced protective antibody concentrations upon proteasome inhibition
The beneficial clinical effects of proteasome inhibition were accompanied by an increase in serum complement levels for C3 (p=0.030) and a significant reduction of anti-dsDNA antibodies, which decreased from a median 366.5 U/mL at baseline to 112.5 U/mL after the last bortezomib cycle (median reduction: 62.2%, p=0.005, figure 1C). In addition, autoantibodies directed against extractable nuclear antigens, such as anti-Sm, anti-RNP/Sm and anti-Ro/SSA, which are believed to be secreted by long-lived PCs, declined in patients displaying those specificities (see online supplementary figure S3). But, pathogenic and vaccine-induced protective antibody titres against measles (32.5%, p<0.001), mumps (24.5%, p=0.003) and tetanus toxoid (29.2%, p=0.012) decreased upon bortezomib treatment (figure 2A–C). Overall, proteasome inhibition was associated with a significant reduction of total immunoglobulins with greater effects on IgM (34.0%) and IgA (34.2%) than on IgG (15.5%, figure 2D–F). Although significantly reduced, immunoglobulin concentrations remained within the reference range and vaccine titres within the protective range in the majority of patients.

Reduction of serum immunoglobulin (Ig) levels and vaccine-induced protective antibody levels by bortezomib. Vaccine titres in serum specific for (A) measles, (B) mumps and (C) tetanus toxoid (TT), and serum concentrations of (D) IgG, (E) IgA and (F) IgM in patients with systemic lupus erythematosus (SLE) (n=8) before and after each cycle of bortezomib. Median/IQR values are shown for each category at baseline before bortezomib treatment (pre-Bz) and after the last bortezomib cycle (post-Bz). The protective levels of vaccine titres and normal range of immunoglobulin levels in serum (dashed lines) are as follows: anti-measles titres >1000 IE/mL, antimumps titres >500 IE/mL, anti-TT titres >0.1 IE/mL, IgG 700–1600 mg/dL, IgA 70–400 mg/dL and IgM 40–230 mg/dL.
Bortezomib depletes peripheral blood and bone-marrow PCs
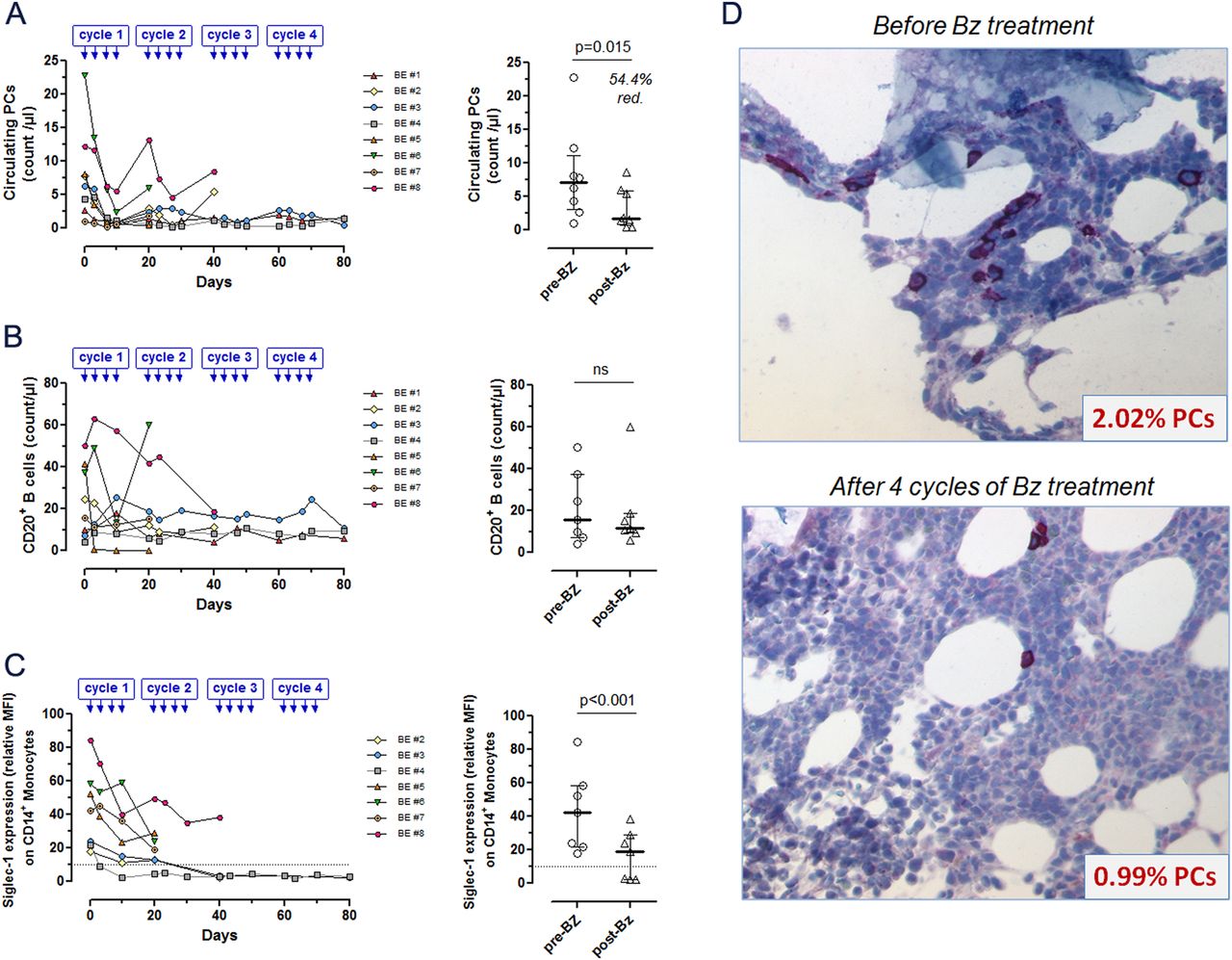
To investigate the effect of bortezomib on peripheral blood PCs, their numbers were analysed by flow cytometry. PC counts (CD19+C20−CD27high) decreased significantly upon proteasome inhibition from a median 7.07/µL at baseline to 1.65/µL 10 days after the last bortezomib cycle (54.4% reduction, p=0.015, figure 3A). Nevertheless, although efficiently depleted by proteasome inhibition, PCs quickly regenerated. Within 10 days of the last bortezomib injection, PC numbers increased, almost returning to pretreatment levels (β=2.1; 95% CI 0.5 to 3.7; p=0.012). In contrast to PCs, peripheral blood B cell (CD19+CD20+) numbers did not significantly decrease upon bortezomib treatment (figure 3B).
{kind=link}
{kind=link}
{kind=link}
Bortezomib depletes peripheral blood and bone marrow plasma cells (PCs) and inhibits type I interferon activity in systemic lupus erythematosus (SLE). Peripheral blood mononuclear cells of patients with SLE (n=8) were analysed by flow cytometry. Absolute numbers of (A) peripheral blood CD3−CD14−DAPI−CD19+CD20−CD27high PCs, (B) CD3−CD14−DAPI−CD19+CD20+ B cells and (C) Siglec-1 expression levels on DAPI−CD14+ monocytes (mean fluorescence intensity, relative to isotype control; normal range, established in 25 age-matched healthy controls, 1.9–10.2) before and after bortezomib treatment. Median/IQR values are shown for each category at baseline before bortezomib treatment (pre-Bz) and after the last bortezomib cycle (post-Bz). (D) Bone marrow samples in one patient (BE #1) were analysed before and after four cycles of bortezomib treatment. The analysis of CD138+ PCs using immunohistology with quantification in 10 high-power fields relative to total cell counts in the bone marrow. Original magnification ×400.
The reduction of pathogenic and protective antibody levels point to a marked depletion of long-lived PCs from bone marrow in response to proteasome inhibition. Indeed, quantification of CD138+ PCs by immunohistology in bone marrow samples from one patient before and after four cycles of bortezomib revealed a 51% reduction of PCs from 2.02% to 0.99% relative to total cell counts in the bone marrow (figure 3D).
Reduction of type-I IFN activity by bortezomib
Data from preclinical models suggested that the TLR-induced IFN-α production was completely abrogated by proteasome inhibiton.8 To evaluate the effect of bortezomib on type-I IFN activity in SLE, flow cytometric expression analysis of Siglec-1 on peripheral blood CD14+ monocytes, as a biomarker for type-I IFN activity,11 ,12 was performed. Siglec-1 expression on monocytes was elevated in all investigated patients at baseline (median relative mean fluorescence intensity (MFI) 42.3, range 17.7–84.6) and declined to a median of 18.8 (relative MFI, range 2.1–38.2, p<0.001, figure 3C) after bortezomib treatment, indicating an inhibition of type-I IFN activity.
Safety
Of 12 patients receiving bortezomib, 11 patients (91.7%) experienced one or more adverse events (AEs), and four (33.3%) experienced one severe adverse event (SAE) during the treatment period (see online supplementary table S3). In total, 19 AEs were reported during the treatment period. The most commonly observed AEs were infections (3/19), nausea (3/19), headache (3/19), polyneuropathy (2/19), fever (2/19) and allergic skin reactions (2/19). Most of these AEs, including polyneuropathy (grade 1), were mild or moderate and resolved completely. Four SAEs occurred, resulting in hospitalisation for fever (n=2) and infection (n=2). Both cases of fever resolved without evidence of infection and management of infections was uncomplicated. Overall, bortezomib was discontinued in seven patients (58%) due to suspected adverse reactions.
Discussion
This study aimed to determine whether the proteasome inhibitor bortezomib induces clinically relevant PC depletion in patients with active, refractory SLE. Bortezomib, approved for the treatment of multiple myeloma, has been demonstrated to deplete PCs in murine models of lupus resulting in amelioration of nephritis and prolonged survival.6 ,8 The therapeutic potential of proteasome inhibition in humans with SLE has not been investigated so far. Our detailed flow-cytometric analyses and monitoring of serological changes presented here demonstrate that bortezomib treatment for SLE is associated with a significant depletion of autoantibody-producing PCs as well as an inhibition of type-I IFN activity and accompanied by a significant improvement of disease manifestations.
Autoreactive memory PCs contribute to the maintenance of autoimmunity in antibody-mediated autoimmune diseases by the persistent secretion of autoantibodies; this is reflected by the induction of immune complex nephritis in immunodeficient RAG−/− mice after adoptive transfer of memory PCs from lupus prone NZB/W mice.13 The fact that the patients included in this study had persistent anti-dsDNA antibody production despite chronic immunosuppression, suggests that the majority of PCs secreting such antibodies were terminally differentiated, non-dividing memory PCs, harboured in dedicated survival niches in the bone marrow or inflamed tissues.1 ,14 Bortezomib induced a strong decrease in anti-dsDNA antibodies and reduced vaccine-induced serum antibodies as well as total immunoglobulin concentrations, suggesting that the drug effectively depletes the memory PCs secreting such antibodies. Indeed, analysis of bone marrow aspirates from one patient before and after four cycles of bortezomib revealed a marked decrease in bone marrow memory PC numbers. However, although efficiently depleted upon proteasome inhibition, peripheral blood PCs regenerated quickly, indicating that bortezomib did not affect their precursors. Similar results had been obtained in murine lupus models, where newly generated PCs were detected as early as 3 days after bortezomib injection and anti-dsDNA antibodies started to increase within 2 weeks after bortezomib treatment.6 These data emphasise the need for combinatorial therapeutic strategies to eliminate PCs and inhibit their regeneration. Given the continuous PC development in active SLE and the short half-life of bortezomib, proteasome inhibition may be given on background immunosuppression, as already performed in patients with antibody-mediated rejection following kidney transplantation9 ,10 or in combination with B-cell-directed therapies.
Beyond PC depletion, data from preclinical models had suggested that proteasome inhibition abrogated type-I IFN activity.8 Consistent with this, type-I IFN activity in patients with SLE was significantly reduced by bortezomib, reflected by decreased Siglec-1 expression levels on monocytes, a signature biomarker for type-I IFN activity.11 ,12 This effect may be due to a suppressed function and/or survival of plasmacytoid dendritic cells, induced by bortezomib, as recently suggested by preclinical studies of proteasome inhibition.8 ,15
The clinical efficacy of bortezomib is remarkable considering that all patients had been refractory to immunosuppression before. Proteasome inhibition may thus serve as a salvage therapy in patients with refractory SLE, in particular as induction therapy in serologically active patients presenting with severe and potential life-threatening organ manifestations. Since most of the clinical effects were achieved within the first 21 days of bortezomib treatment, few cycles of bortezomib induction therapy may be sufficient to ameliorate disease manifestations, and even restore responsiveness to conventional immunosuppression. The observed effects of proteasome inhibition may be partially attributable to the coadministration of dexamethasone with bortezomib on each day of injection. However, similar clinical effects were obtained in patients receiving bortezomib without dexamethasone who were analysed in as separate cohort (see online supplementary table S2) suggesting that mainly bortezomib mediated the clinical response. Nevertheless, given recent data indicating the potential benefit of bortezomib-dexamethasone compared with single-agent bortezomib in myeloma, such combination therapy might also be superior in SLE,16 but this needs further to be investigated in controlled trials.
The possible benefits of bortezomib must be weighed against its adverse effects. Although mild to moderate, AEs occurred in 92% of patients and resulted in premature discontinuation in 58% of patients. Among the AEs were infections, but occurrence of infections did not correlate to the reduction of overall immunoglobulin levels or vaccine-specific antibodies. A reduction of AEs, such as polyneuropathy, with similar levels of efficacy, had been observed upon subcutaneous administration of bortezomib,17 ,18 and might further be reduced by replacing bortezomib with next-generation proteasome inhibitors such as carfilzomib19 ,20 or the orally delivered MLN9708 and oprozomib.
In conclusion, the proteasome inhibitor bortezomib shows therapeutically relevant targeting of autoreactive PCs and inhibition of type-I IFN activity in patients with refractory SLE. This identifies proteasome inhibitors as a promising therapeutic option for patients who respond poorly to conventional therapies. For sustained efficacy, bortezomib has to be combined with therapeutic approaches that prevent the regeneration of autoreactive PCs from their precursor B cells, but this needs to be confirmed in randomised controlled trials.
Acknowledgments
We thank Cornelia Dähnrich from EUROIMMUN AG (Lübeck, Germany) for analysing serum samples for autoantibody concentrations. We thank Torsten Diekhoff, Charité—University Medicine Berlin, Department of Radiology, for providing CT images, Christoph Loddenkemper formerly Charité, Department of Pathology, for contributing to immunohistology analysis of bone marrow plasma cells, and Robert Spranger, Institute of Virology, Tobias Braun and Stephanie Finzel, Department of Internal Medicine 3, University of Erlangen-Nuremberg, for assistance in data collection and analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
- Data supplement 3 - Online tables
Footnotes
Handling editor Tore K Kvien
FH and REV are senior authors and contributed equally.
Contributors TA, FH, REV and AR conceived the study. TA, RS, AR-R, H-ML, G-RB, JR, MW and GS made substantial contributions to clinical data acquisition. TA, AAK, QC, BFH, AT and AW performed experiments. TA, JK, AAK, FH, RS and REV analysed the data. TA, FH and REV wrote the manuscript. G-RB and AR critically revised the manuscript. FH and REV contributed equally.
Funding This work was supported by grants from the German Research Foundation (DFG, grants SFB650 TP12 and 17, FOR 831 TP 8 [VO673/3-2] and Transregio SFB TRR 130, TP12 and TP15).
Competing interests None.
Patient consent Obtained.
Ethics approval All patients provided written informed consent after being informed about the nature of the “off-label” therapy and the potential risks of the treatment. The local Institutional Review Board (IRB) was notified in each individual patient and approved the analysis of samples for research (EA1/124/09).
Provenance and peer review Not commissioned; externally peer reviewed.