Article Text

Abstract
Objectives Disease Activity Score in 28 joints calculated with C-reactive protein (DAS28-CRP) is used instead of erythrocyte sedimentation rate (DAS28-ESR) to assess rheumatoid arthritis disease activity; however, values for remission and low disease activity (LDA) for DAS28-CRP have not been validated. American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) guidelines suggest remission should be calculated by Simplified Disease Activity Index (SDAI) rather than DAS28-ESR. We examined values of remission and LDA of DAS28-CRP that correspond to the respective cut-off points for DAS28-ESR and SDAI from five clinical trials.
Methods DAS28-CRP cut-offs that best correspond to DAS28-ESR remission <2.6 and LDA ≤3.2 were obtained by cumulative distribution plots, receiver operating curves and maximum concordance and averaged for each approach, treatment group and study. Level of agreement between DAS28-CRP and DAS28-ESR remission and LDA cut-offs was compared against each other and versus SDAI remission ≤3.3 and LDA ≤11.
Results Percentage of patients who achieved remission and LDA by DAS28-ESR cut-offs was greater for DAS28-CRP versus DAS28-ESR regardless of patient population or treatment group. Discordance between CRP and ESR cut-offs ranged from 4%–26% and 8%–23% for remission and LDA, respectively, and 19%–40% and 6%–11% for DAS28-CRP versus SDAI, respectively. Estimated (range) remission and LDA thresholds were 2.4 (2.2–2.6) and 2.9 (2.6–3.3), 1.9 (1.6–2.2) and 3.1 (3.1–3.3) and 2.2 (1.1–2.9) and 3.6 (3.4–4.0) for DAS28-CRP versus DAS28-ESR, DAS28-CRP versus SDAI and DAS28-ESR versus SDAI, respectively.
Conclusions DAS28-CRP underestimates disease activity when using cut-off points validated for DAS28-ESR; therefore, DAS28-ESR cut-off values should not be applied to DAS28-CRP. Although DAS28-CRP and DAS28-ESR cut-offs for LDA ≤3.2 correspond to SDAI LDA, neither corresponds well to SDAI remission.
- DAS28
- Rheumatoid Arthritis
- Anti-TNF
- Disease Activity
- TNF-alpha
Statistics from Altmetric.com
Introduction
Use of the Disease Activity Score (DAS) using erythrocyte sedimentation rate (ESR) has been a valuable addition in the measurement of rheumatoid arthritis (RA) disease activity since its validation and subsequent modification to use 28 joint counts (DAS28).1 ,2 In 2004, Fransen et al3 predicted that DAS28 calculated with C-reactive protein (CRP) could replace DAS28-ESR in spite of the fact that cut-offs for remission and low disease activity (LDA) have not been validated for DAS28-CRP. Since then, it has been common for DAS28-CRP to be used in clinical practice and clinical trials applying the validated cut-offs of remission and LDA determined for DAS28-ESR.3 The American College of Rheumatology (ACR) 2012 revised criteria and European Medicines Agency (EMA) 2013 updated recommendations for treatment of RA include the DAS28-CRP calculation as an alternative to DAS28-ESR and do not make any distinction between the two measures in spite of the lack of validated cut-offs.4 ,5
The ACR suggests that the cut-offs for remission and LDA determined for DAS28-ESR can be used for both measures in spite of noting the discrepancies in applying DAS28-ESR cut-off points to DAS28-CRP calculations, which overestimates remission and LDA.6 Multiple clinical studies corroborate that within the same population, DAS28-CRP values are much lower as a whole when compared with DAS28-ESR and thus would overestimate the proportion of patients achieving LDA or remission.7–11 In a previous report, analysis of these two measures showed mean DAS28-CRP and ESR was 5.8 and 6.2 in early RA and 6.1 and 6.4 in established RA at baseline, respectively, with as many as 30% of patients categorised into a different disease activity level depending upon which measure was used.8
Analyses from several studies have provided data that suggested a significant correlation between the two measures. However, correlations between the unique components (0.70×ln[ESR] vs 0.36×ln[CRP+1]+0.96) between the two measures have not been analysed. In addition, thresholds for remission and LDA for DAS28-CRP have not been validated.5 ,8 ,11–13 This results in misclassification if thresholds for DAS28-ESR are applied to DAS28-CRP. A validated set of cut-off points for DAS28-CRP remission, LDA and moderate and high disease activity is needed to be able to use the DAS28-CRP correctly and appropriately in interpretation of clinical results both in clinical trials and in practice.
Rather than DAS28 (calculated by either CRP or ESR), Simplified Disease Activity Index (SDAI) is recommended by the ACR and the European League Against Rheumatism (EULAR) for use in clinical trials and routine clinical practice to assess disease activity in RA.6 ,14 SDAI and DAS28 are similar disease activity measures in that they both use tender and swollen joint counts, Patient Global Assessment and a laboratory value (either ESR or CRP) in their mathematical formulas with the addition of Physician Global Assessment in the SDAI calculation. However, SDAI and DAS28 calculations differ in how they weigh their individual components, and in that SDAI uses CRP while DAS28 cut-off values are established for ESR.1 ,15 SDAI defines remission as a value ≤3.3 and LDA as a value of >3.3 to ≤11.0; DAS28-ESR values for remission and LDA are <2.6 and 2.6 to ≤3.2, respectively.6 ,15 As SDAI is now the standard to define remission and LDA, when establishing cut-offs for DAS28-CRP, comparisons to the SDAI values should be made.
When establishing and analysing new and established cut-offs, it is essential to examine and analyse differences in DAS28-CRP, DAS28-ESR and SDAI values across large and diverse RA patient populations. The aim of this analysis is to examine the value of DAS28-CRP that corresponds to the value of DAS28-ESR for cut-off points for remission and LDA as well as DAS28-CRP and DAS28-ESR cut-offs that correspond to SDAI LDA and remission, using three different patient populations (moderate, early moderate-to-severe and established moderate-to-severe) across five randomised clinical controlled trials using three different statistical approaches.
Methods
Randomised patients with moderate RA (PRESERVE), early moderate-to-severe RA (COMET) and established, moderate-to-severe RA (TEMPO, APPEAL and LARA) who received either etanercept (ETN) 50 mg weekly plus methotrexate (MTX), MTX alone or disease-modifying antirheumatic drugs (DMARDs) plus MTX and had at least one postbaseline observation were analysed from five clinical trials. The five clinical trials are summarised in table 1; study schema, baseline population demographics, efficacy and safety details were previously published elsewhere.9 ,16–19
Summary of clinical trials
DAS28-CRP, DAS28-ESR and SDAI response rates were calculated separately for each study and treatment group at their respective study endpoints carrying last observation forward for patients who were missing the final study endpoint. Based on the validated DAS28-ESR thresholds (remission <2.6; LDA 2.6 to ≤3.2), corresponding thresholds for DAS28-CRP were determined for each study and treatment group using three different statistical approaches: cumulative distribution plots, receiver operating curves (ROC) and maximum concordance. The same approach was used to determine DAS28-CRP values as well as DAS28-ESR values that correspond to the established SDAI thresholds (remission, ≤3.3; LDA, ≤11). DAS28-CRP and DAS28-ESR were then compared based on the validated DAS28-ESR cut-off points for remission <2.6 and LDA ≤3.2, using sensitivity, specificity, κ coefficients and proportion of discordance statistics. The same comparison was done between DAS28-CRP and SDAI and between DAS28-ESR and SDAI cut-offs of remission (≤3.3) and LDA (3.3 to ≤11).
Cumulative distribution approach
For each study and each treatment group, two cumulative distribution plots, one for DAS28-CRP and another for DAS28-ESR, were plotted, illustrating the cumulative percentage of patients up to and including each DAS28-CRP or DAS28-ESR value. A vertical line was drawn from remission or LDA thresholds of the DAS28-ESR plot down to the DAS28-CRP plot. The intersection of the vertical line on the DAS28-CRP plot indicated the corresponding DAS28-CRP threshold. This same cumulative distribution approach was done between DAS28-CRP and SDAI and between DAS28-ESR and SDAI.
Receiver operating curves
DAS28-CRP thresholds that best correspond to the established ESR thresholds were obtained by maximising sensitivity plus specificity in ROC analyses. Sensitivity was defined as the true proportion of positive results and specificity as the true proportion of negative results. This also was completed between DAS28-CRP and SDAI and between DAS28-ESR and SDAI.
Maximum concordance
DAS28-CRP thresholds were selected that best correspond to DAS28-ESR thresholds using maximum concordance; in other words, the largest sum of the number of patients who were above the threshold for both measures plus the number of patients who are below the threshold for both measures. This also was completed between DAS28-CRP and SDAI and between DAS28-ESR and SDAI.
Statistical analyses
The calculated DAS28-CRP thresholds from each of the three statistical approaches were then averaged by remission and LDA for each study and treatment group. Subsequently, the calculated thresholds were then pooled among all studies and averaged to create a mean threshold for each treatment group and further averaged once again to obtain the overall new cut-offs that best correspond to either DAS28-ESR or SDAI cut-offs for remission and LDA.
Level of agreement between the calculated DAS28-CRP and established DAS28-ESR thresholds was determined by κ coefficient, sensitivity and specificity. Level of agreement also was determined between the calculated DAS28-CRP thresholds and established SDAI thresholds and between the established DAS28-ESR thresholds and established SDAI thresholds. DAS28-CRP and DAS28-ESR, along with their unique components (0.70×ln[ESR] and 0.36×ln[CRP+1]+0.96), were analysed as continuous parameters using Spearman's correlation. Relationships between DAS28-CRP and SDAI and between DAS28-ESR and SDAI also were analysed using Spearman's correlation.
Results
A total of 2534 patients were included in this analysis. The percentage of patients who achieved remission and LDA by the DAS28-ESR cut-offs of <2.6 and ≤3.2 was generally higher for DAS28-CRP than DAS28-ESR and SDAI calculations regardless of study population or treatment group (table 2). In general, the proportions of patients achieving LDA and remission were higher if the cut-offs used for DAS28-ESR or SDAI were applied to DAS28-CRP, thus overestimating improvement in disease activity if DAS28-CRP was used.
Statistical measures of agreement between DAS28-CRP, DAS28-ESR and SDAI (remission <2.6 and LDA ≤3.2)
As the proportions of patients who achieved the DAS28 threshold levels by CRP and ESR calculations do not correspond in a one-to-one ratio (eg, one patient may achieve remission via DAS28-CRP but not via DAS28-ESR and vice versa), differences in response between these two measures were determined by discordance. The proportion of discordance between the DAS28-CRP and ESR composite measures ranged from 8% to 23% for LDA and 4% to 26% for remission for the different studies and treatment groups (table 2). Comparatively, the proportion of discordance between DAS28-CRP and SDAI ranged from 2% to 11% for LDA and 2% to 40% for remission, and between DAS28-ESR and SDAI ranged from 6% to 24% for LDA and 4% and 43% for remission (table 2). Overall, the percentage of patients achieving remission or LDA was lower for DAS28-ESR than DAS28-CRP when using values of <2.6 and 2.6 to ≤3.2 as cut-offs for both measures. A higher discordance was observed between DAS28-CRP versus SDAI compared with DAS28-ESR versus SDAI; thus DAS28-CRP overestimates remission even more than DAS28-ESR if <2.6 is the cut-off for both. The calculated DAS28-CRP cut-off based on SDAI remission is even lower than the DAS28-ESR established cut-offs.
Although DAS28-CRP and ESR measures were highly correlated (Spearman's correlation, range 0.80–0.96; p<0.001) for each study and treatment group, their unique components (0.70×ln[ESR] vs 0.36×ln[CRP+1]+0.96) were not highly correlated (range 0.35–0.50; p<0.001; data not shown). Overall, the κ coefficients of agreement between DAS28-CRP and DAS28-ESR calculations for remission and LDA ranged between 0.40 and 0.79 and were statistically significant between the two measures (table 2). For DAS28-CRP and DAS28-ESR analysis, the sensitivity in detecting a true rate of response (where a patient has a positive response for both the test and comparator thresholds) and the specificity of detecting a true rate of non-response (where a patient has a negative response (non-responder) for both the test and comparator thresholds) was high, with most per cent sensitivity ranging in the 80–90 s, and in the 70–80 s for per cent specificity. Overall, the κ coefficients of agreement between DAS28-CRP <2.6 and SDAI ≤3.3 ranged between 0.20 and 0.76 and were statistically significant between the two measures, whereas κ coefficients between DAS28-CRP ≤3.2 and SDAI LDA ≤11 ranged between 0.77 and 0.91 (table 2). Similar observations were made between DAS28-ESR <2.6 and SDAI ≤3.3 with the κ coefficients of agreement ranging between 0.26 and 0.51, which was statistically significant, whereas κ coefficients between DAS28-ESR ≤3.2 and SDAI ≤11 ranged between 0.47 and 0.75 (table 2).
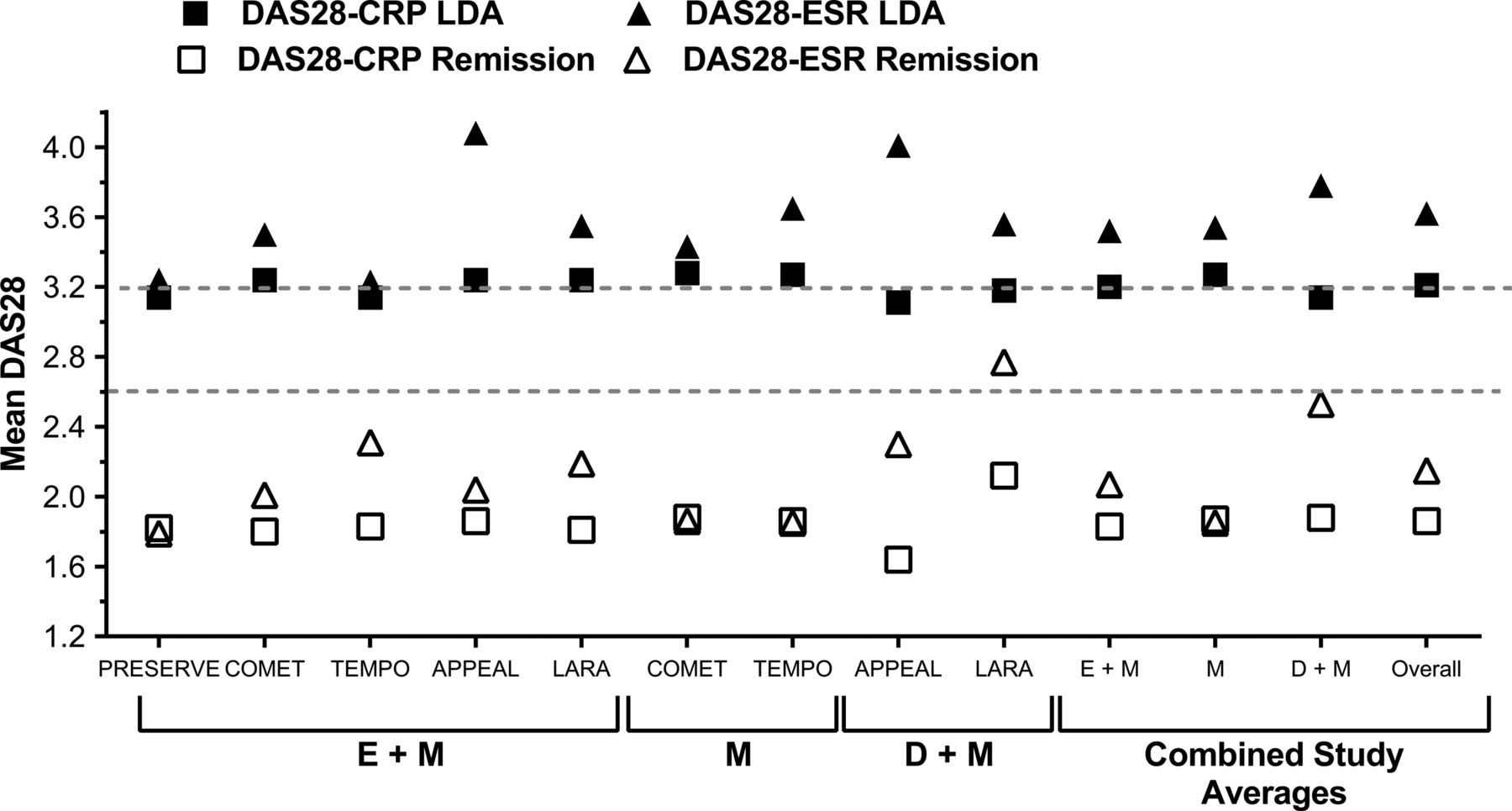
Estimated DAS28-CRP thresholds for remission as they correspond to DAS28-ESR averaged among the three statistical approaches by study and treatment arm ranged between 2.2 and 2.6, with an overall 2.4 average among all studies and treatments (figure 1 and online supplementary table S1A). Estimated DAS28-CRP thresholds for LDA ranged between 2.6 and 3.3, with an overall average of 2.9 among all studies and treatment groups. The newly calculated cut-offs of 2.4 for remission and 2.9 for LDA were similar among studies (with the exception of APPEAL) and treatments with only minor differences between ETN plus MTX or MTX alone versus DMARD plus MTX treatment groups.

Estimated DAS28-CRP thresholds that correspond to DAS28-ESR thresholds, the average of three statistical approaches. DAS28-CRP, Disease Activity Score in 28 joints calculated with C-reactive protein; DAS28-ESR, Disease Activity Score in 28 joints calculated with erythrocyte sedimentation rate; D+M, disease-modifying antirheumatic drugs plus methotrexate; E+M, etanercept plus methotrexate; LDA, low disease activity; M, methotrexate.
Importantly, the estimated DAS28-CRP thresholds for remission and LDA as they correspond to SDAI were 1.9 and 3.2, respectively, whereas the corresponding DAS28-ESR thresholds to SDAI were slightly higher with an overall average of 2.2 and 3.6, respectively (figure 2 and online supplementary tables S1B and S1C). These corresponding cut-offs were similar among statistical approaches, studies and treatments within each DAS28 versus SDAI comparison.

{kind=link}
{kind=link}
Estimated DAS28-CRP and DAS28-ESR thresholds that correspond to SDAI, the average of three statistical approaches. DAS28-CRP, Disease Activity Score in 28 joints calculated with C-reactive protein; DAS28-ESR, Disease Activity Score in 28 joints calculated with erythrocyte sedimentation rate; D+M, disease-modifying antirheumatic drugs plus methotrexate; E+M, etanercept plus methotrexate; LDA, low disease activity; M, methotrexate; SDAI, Simplified Disease Activity Index.
It was noted that cut-offs determined from the APPEAL (Asia-Pacific region) trial were lower compared with the other enrolled trials, which were global and Latin American studies (table 2). To explore this further, the same three statistical analyses approach was conducted on the pooled study population between the Asian and non-Asian populations in the ETN plus MTX treatment arm (the other treatment arms had too few Asian patients for meaningful analysis). The Asian population had noticeably lower thresholds for DAS28-CRP based on DAS28-ESR but not for DAS28-CRP based on SDAI or for DAS28-ESR based on SDAI compared with the non-Asian population in this analysis (see online supplementary tables S2A,B).
The same statistical analyses were completed using Clinical Disease Activity Index LDA and remission in relationship to DAS28-CRP and DAS28-ESR, which demonstrated very similar results to SDAI (see online supplementary tables S3A,B).
Discussion
Many clinicians use DAS28-CRP over DAS28-ESR to assess RA disease activity owing to the presumed consistency of CRP and that it removes some of the potential variability related to user-dependent factors associated with ESR (eg, time to conduct test, temperature, angle of test tube). DAS28-CRP also is frequently used in clinical trials because CRP can be determined by a central laboratory using consistent methodology. All clinical trials that have employed the DAS28-CRP as a primary measure have inaccurately used the DAS28-ESR cut-off points, validated for DAS28-ESR but not DAS28-CRP, which will inflate the numbers of patients achieving LDA or remission. Previous comparisons of the two measures and this analysis have been consistent and have demonstrated that the established ESR cut-offs of <2.6 and ≤3.2 provide fair agreement between DAS28-CRP and ESR based on modest κ coefficients when using the CRP calculation. However, overall the κ coefficients were higher with LDA than remission thresholds, indicating a stronger agreement for LDA across measures and therefore little difference between the test and established cut-offs. Comparatively, the κ coefficients for remission are lower, indicating less of an agreement and more discrepancy between the test and established remission cut-offs. In addition, the proportion of discordance between the two DAS28 measures was wide and variable—between 4% to 26% for remission and 8% to 23% for LDA. Differences between the two measures were not consistent, further emphasising the need for independent validated DAS28-CRP remission and LDA cut-off points.
If SDAI is now the standard to define remission, as recommended by both ACR and EULAR, both DAS28-CRP and DAS28-ESR grossly overestimate the proportion of patients achieving remission, with DAS28-CRP performing inferiorly to DAS28-ESR. With respect to LDA, the proportion of patients achieving this threshold is relatively similar whether using SDAI ≤11, DAS28-ESR or DAS28-CRP ≤3.2.
Estimated DAS28-CRP disease activity cut-off points for remission of 2.4 and for LDA of 2.9, which we calculated from this dataset, compare favourably to those estimated elsewhere.7–11 One report estimated thresholds of remission/LDA of 2.4 and low/moderate disease activity of 3.0 conducted by ROC analysis alone, while another report obtained a similar conclusion (ROC analysis only) of a remission threshold of 2.3, with a slightly lower estimate of an LDA threshold of 2.7.12 ,20
Interestingly, currently published articles regarding establishing DAS28-CRP-specific thresholds only focus on ROC analysis. Pros and cons to every statistical approach make it difficult to find one best method. For example, statistical parameters within an ROC analysis can produce different results depending on the criteria used. In our approach, we required that sensitivity and specificity be maximised; however, different criteria may have resulted in different cut-offs. In our analysis, the minor differences in cut-offs among the three approaches indicated that the results are consistent and corroborative. Additional analysis will need to be conducted to determine the best statistical approach in determining DAS28-CRP thresholds.
This analysis was conducted in treated patients at their last time point and therefore there were too few patients for analyses in the moderate and high disease activity categories to determine the corresponding DAS28-ESR and CRP thresholds. Although this analysis would be of interest, the EULAR guidelines stress treatment to a target of remission in early disease, and LDA is acceptable for patients with established disease. Therefore, a correct determination of remission and LDA is more important to the practising physician when deciding whether to continue or escalate therapy. In order to determine the corresponding DAS28-CRP cut-offs for the moderate and high disease activity categories, additional analysis should be conducted at baseline before patients receive treatment.
Limitations to this analysis include possible variability in assays used to measure the inflammatory markers, for example, central, regional and local laboratory differences with possible differing sensitivities among the trials included in this analysis. All five clinical trials in this analysis were conducted independent of each other, encompassing a variety of patient populations, geographic regions, enrolment criteria, clinical trial designs, time frames and study time points, which should be considered when assessing calculated DAS28-CRP thresholds. As with all composite measures that use laboratory components such as ESR and CRP, physicians should keep in mind patients’ concomitant conditions and medications that may possibly influence those components. Although a limitation to this analysis is that it was conducted within the parameters of homogeneous clinical trial populations, the utility of the cut-offs would be expected to be the same whether in a clinical trial or clinical practice noting that these results may not accurately reflect patients with conditions other than RA. However, in clinical practice, many other variables need to be considered in the interpretation of the clinical significance of the values of DAS28-CRP, DAS28-ESR and SDAI. It would be of interest to explore concomitant conditions and therapies/medications that directly inhibit the production of CRP (such as interleukin-6 inhibitors) to determine their possible influence on the reporting of disease activity, these composite measures and comparative LDA/remission cut-off values between measures.
Noticeable differences within the Asian population on the overall estimated CRP thresholds have been documented.12 This observation was corroborated in our analysis between Asian and non-Asian populations with estimated DAS28-CRP thresholds based on DAS28-ESR for remission of 2.2 vs 2.4, respectively, and for LDA of 2.6 vs 3.1, respectively.
To our knowledge, this is the largest comparative analysis of DAS28-CRP, DAS28-ESR and SDAI across multiple geographic regions, disease activity and RA patient populations. In general, DAS28-CRP underestimates disease activity and overestimates remission and LDA when using cut-off points validated for DAS28-ESR. The estimated DAS28-CRP thresholds calculated from three different patient populations across five randomised clinical controlled trials of 2.4 for remission and 2.9 for LDA are consistent with previously published DAS28-CRP threshold estimates.7–11 Interestingly, the DAS28 LDA value of ≤3.2 corresponds well with SDAI LDA ≤11.0 but overestimates remission ≤2.6 when compared with SDAI remission ≤3.3. Additional studies are needed to further validate these proposed DAS28-CRP disease activity thresholds and the relationships between the proposed and established thresholds with SDAI disease activity thresholds. If the remission is the goal, we should consider using SDAI as the standard to determine disease activity as both DAS28-ESR and DAS28-CRP overestimate the proportion of patients achieving remission, with DAS28-CRP performing inferiorly to DAS28-ESR.
Acknowledgments
The authors wish to thank all patients who participated in the trials and all investigators and medical staff of the participating centres.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
Handling editor Tore K Kvien
Contributors All authors have fulfilled the ICMJE 2013 authorship criteria and approve the final content of this concise report for submission.
Funding All clinical trials used in this analysis (PRESERVE, COMET, TEMPO, APPEAL and LARA) were sponsored by Pfizer Inc. Pfizer Inc was involved in the study design, collection, analysis and interpretation of the data, writing of the report and in the decision to submit the paper for publication. Medical writing support was provided by Stephanie Eide of Engage Scientific Solutions and was funded by Pfizer Inc.
Competing interests RF was a principal investigator for clinical trials used in this analysis and has received consulting fees unrelated to the development of this article. DvdH has received consulting fees from Pfizer Inc unrelated to the development of this article. AS is an employee of Inventiv Health Inc who is a paid contractor to Pfizer Inc in the development of this article. ASK, RP, LM and EB are employees of Pfizer Inc.
Ethics approval Multiple clinical trial sites, local and regional ethics committees used.
Provenance and peer review Not commissioned; externally peer reviewed.