Article Text

Abstract
Objectives Combination therapy with methotrexate (MTX) and tumour necrosis factor (TNF) blockade has increased remission rates in patients with rheumatoid arthritis. However, there are no guidelines regarding cessation of therapy. There is a need for markers predictive of sustained remission following cessation of TNF blocker therapy.
Methods Patients in remission (DAS28 <2.6) treated with a TNF blocker and MTX as initial or delayed therapy were recruited. Joints were assessed for grey scale synovitis and power Doppler (PD) activity. Immunological assessment involved advanced six-colour flow cytometry.
Results Of the 47 patients recruited, 27 had received initial treatment and 20 delayed treatment with TNF blocking drugs. Two years after stopping TNF blocker therapy, the main predictor of successful cessation was timing of treatment; 59% of patients in the initial treatment group sustained remission compared with 15% in the delayed treatment group (p=0.003). Within the initial treatment group, secondary analysis showed that the only clinical predictor of successful cessation of treatment was shorter symptom duration before receiving treatment (median 5.5 months vs 9 months; p=0.008). No other clinical features were associated with successful cessation of therapy. Thirty-five per cent of patients had low PD activity but levels were not informative. Several immunological parameters were significantly associated with sustained remission including abnormal differentiation subset of T cells and regulatory T cells. Similar non-significant trends were observed in the delayed treatment group.
Conclusion In patients in remission with low levels of imaging synovitis receiving combination treatment with a TNF blocker and MTX, immunological parameters and short duration of untreated symptoms were associated with successful cessation of TNF blocker therapy.
Statistics from Altmetric.com
For patients with rheumatoid arthritis (RA), remission is the goal of treatment. The therapeutic agent and timing of treatment both have crucial roles in achieving remission.1 In patients with early RA treated with combination therapy (tumour necrosis factor (TNF) blocker and methotrexate (MTX)), clinical remission rates of 40–50% have been reported with considerable reduction in radiographic damage.2 3 Furthermore, there is evidence that sustainable remission can be achieved after withdrawal of treatment with a TNF blocker or, in some cases, disease-modifying antirheumatic drugs (DMARDs) in patients with early RA.3 4 In contrast, in patients with established RA, cessation of TNF blocker has led to high flare rates.5 Furthermore, the majority of patients with established RA in DMARD-induced remission are known to have synovitis detectable by imaging.6
Studies have shown superior radiographic and functional outcomes with higher rates of remission if DMARD treatment is commenced within 3 months of diagnosis.7 8 The place of imaging-detected synovitis in predicting sustained remission after cessation of TNF blocker therapy has not been examined.
Immunological assessment of the remission state may also be valuable in predicting successful cessation of TNF blocker therapy. Inflammation has a direct effect on T cell differentiation in RA9 and drives the differentiation and proliferation of naïve CD4+ T cells towards an abnormal phenotype. These cells, known as inflammation-related cells (IRC), predicted relapse in a cohort of patients with RA in DMARD-induced remission.10 The value of IRC in predicting successful cessation of TNF blocker is still unknown. Another marker of immune-mediated disease, the frequency of naturally occurring regulatory T cells (Tregs), is reduced in patients with RA.11 12 Using more sensitive Treg markers, it is hypothesised that Tregs may also provide predictive value.13,–,15
The ability to predict successful cessation of TNF blockade would have significant health economic implications. Using clinical, imaging and immunological assessments, this study aimed to determine markers of successful cessation of TNF blockade.
Methods
Patients
Forty-seven patients with RA (American College of Rheumatology diagnostic criteria, >18 years) in remission according to the European League Against Rheumatism definition of remission (DAS28 <2.6) following treatment with MTX and TNF blocker therapy with no change in therapy or disease activity for at least 6 months (range 6–17 months) were recruited to this prospective controlled study.16 All patients stopped the TNF blocking drug and continued with MTX for 24 months' follow-up. The primary outcome was flare of disease as defined by an increase of DAS28 >2.6 or an increase of 1.2 if DAS remained <2.6. Clinical and ultrasound assessment are described in the online supplement.
Immunological assessment
Flow cytometry analysis was performed to quantify naïve CD4+ T cells (CD3+CD4+CD45RBbright CD45RA+CD62L+), IRC (CD3+CD4+CD45RBbright CD45RA+Cd62L−) and Tregs (CD4+CD25bright FOXP3+) (experimental details are given in the online supplement). Further phenotyping of Tregs included CD127 and CD62L.
Statistical analysis
Statistical software SPSS Version 16 was used. Non-parametric statistics were used throughout. Continuous measures were compared between groups using Mann–Whitney U tests and nominal measures with χ2 tests. Before obtaining odds ratios, all continuous measures were trichotomised at the tertiles of distribution. Patients with missing values were given an intermediate score to preserve the number of patients entered into the analysis, allowing us to test whether missing data were associated with higher or lower than expected odds of achieving sustained remission. Exact logistic regression was used to assess whether clinical and immunological measures were individually related to the odds of achieving sustained remission. Only univariate associations were examined owing to the low patient numbers.
Results
Characteristics of the remission group
Forty-seven patients in DAS28 remission treated with combination therapy were recruited (table 1). None of the patients was receiving regular corticosteroids. Twenty-seven patients received combination therapy as first-line treatment for 12 months (initial treatment group, median disease duration 19 months), then stopped the TNF blocker drug. Twenty patients received combination therapy after fulfilling the NICE prescribing guidelines for biological therapy (delayed treatment group) with median disease duration of 120 months. Patients in the second group had failed at least two DMARDs (including MTX) and 10 (50%) had also failed a previous TNF-blocking drug due to secondary non-response.17 Apart from longer duration of remission at recruitment in the delayed treatment group, only parameters associated with disease duration and accumulation of damage were significantly different between the two groups.
Clinical characteristics of the initial and delayed treatment groups
Imaging assessment
Ultrasound data were available on 40 patients (20 in each group). Comparing the initial treatment group with the delayed treatment group, 85% and 90% of patients had grey scale (GS) synovial hypertrophy, respectively (GS >0). However, patients in the initial treatment group had significantly lower GS synovial hypertrophy scores (median 5 vs 12, p=0.02); 35% and 45% of patients, respectively, also had power Doppler (PD) activity (PD >0) but no differences in scores were noted, all patients having low levels of PD activity.
Immunological assessment
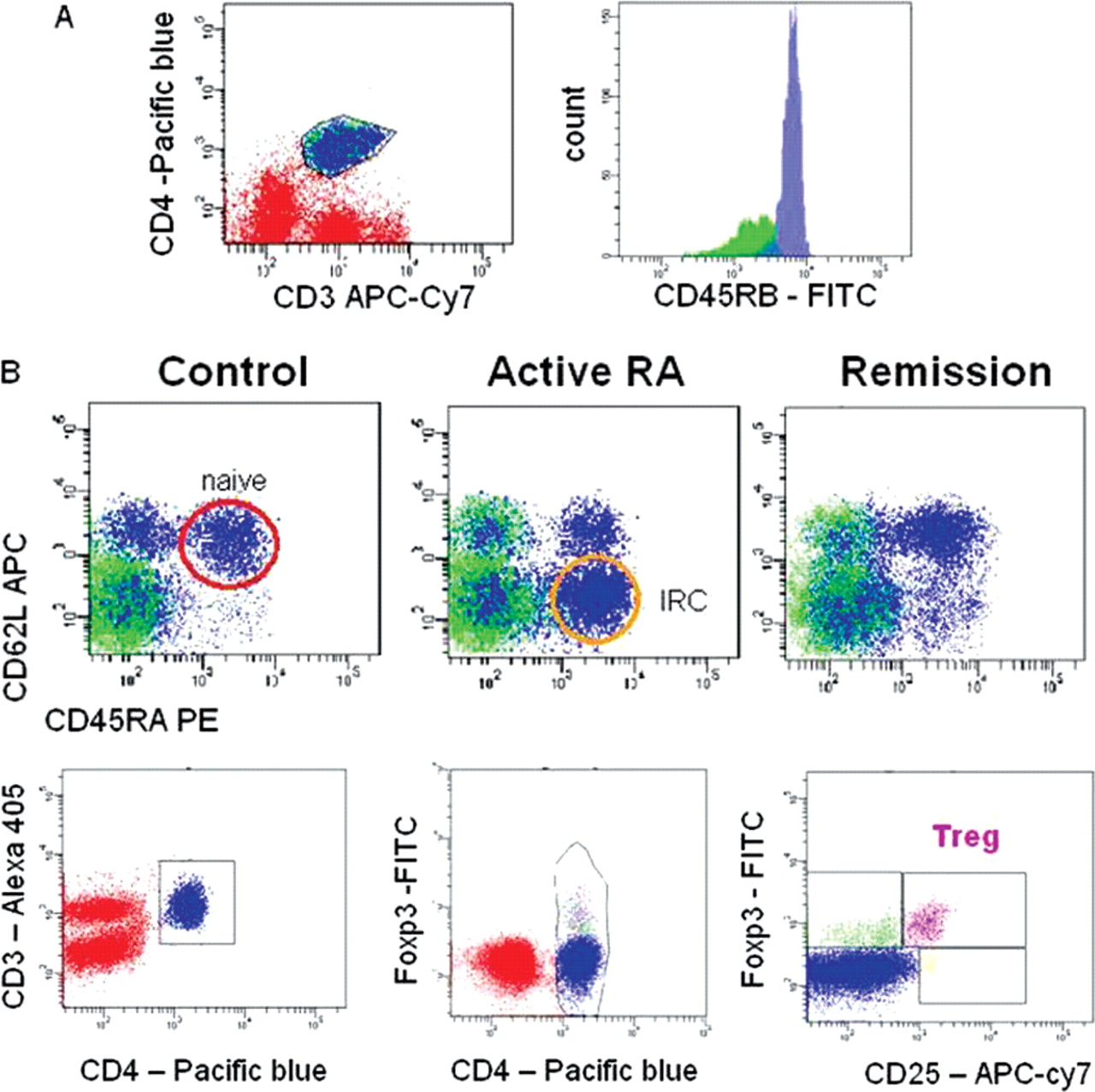
The frequency of IRC and naïve CD4+ T cells was determined by flow cytometry using a successive gating strategy (see figure 1A). A double CD25high/FOXP3+ gate was used to define Tregs (figure 1B). Comparing the immunological characteristics of patients in the initial treatment group with those in the delayed treatment group, no differences in IRC frequency or naïve T cell frequency were observed. Surprisingly, the frequency of Tregs (CD25high/FOXP3+) was higher in the delayed treatment group than in the group receiving initial TNF blocker therapy (3.95% vs 1.57%, p=0.001).

Gating strategies for the quantification of inflammation-related cells (IRC) and naive CD4+ T cells and T regulatory cells (Tregs) using flow cytometry. (A) Representative flow cytometry plots for a healthy control, patient with active rheumatoid arthritis (RA) and patient with RA in remission. Naïve CD4+ T cells were gated first on the basis of their expression of CD3+ and CD4+ double expression followed by a high expression of CD45RB, CD45RA+ and CD62L+ (red circle). IRC were CD3+CD4+ T cells expressing high levels of CD45RB, CD45RA+ but no CD62L (orange circle). (B) Representative plot for gating Tregs as CD3+CD4+ T cells, with a FOXP3+and CD25high phenotype (purple gate). Of note, subsets with a FOXP3+CD25− (green gate) or FOXP3−CD25+ (orange gate) were also identified.
Parameters associated with successful cessation of TNF blocker drugs
Nineteen patients (40%) sustained remission for 24 months, associated with shorter duration of disease (table 2; p<0.0001), lower Health Assessment Questionnaire (HAQ) scores (p=0.012) and lower RA Quality of Life Questionnaire (RAQoL) scores (p=0.039), but no difference was seen in the duration of remission compared with patients who flared. Significantly more patients in the initial treatment group than in the late treatment group were able to sustain remission (59% vs 15%; p=0.003). The median time to any flare in the initial treatment group was 14 months (range 9–24 months) after stopping treatment compared with 4 weeks (range 2–10 weeks) in the late treatment group. Ultrasound assessment was available on 40 patients (14 with sustained remission and 26 with flare). The percentage of patients with PD >0 and GS synovial hypertrophy (GS >0) was similar in the remission group (36% and 93%, respectively) and the flare group (42% and 85%, respectively).
Clinical and immunological characteristics for patients in sustained remission and patients who flared
Sustained remission was associated with a significantly lower IRC frequency (p<0.001) and higher naïve T cell frequency (p<0.001). Treg frequency was, however, higher in the flare group (p=0.001; figure 2B). Further analysis to refine the phenotype of the CD25high/FOXP3+ Tregs using CD127 and CD62L showed that CD62L+ Tregs were more frequent in the sustained remission group than in the flare group (p<0.001; figure 2B).

{kind=link}
{kind=link}
Extended phenotype of T regulatory cells (Tregs) and difference in Treg phenotype in sustained remission and flare. (A) Representative plot from a healthy individual for gating Tregs as CD4+ T cells (blue gate) with a FOXP3+ and CD25high phenotype (green gate, top row of secondary plots). Subsets with a FOXP3+CD25− were identified as an orange gate (bottom row) and cells FOXP3−CD25+ with a pink gate (middle row). Expression of CD127 and CD62L was analysed using these three gates. Tregs were CD127low and CD62L+, FOXP3+CD25− were mostly CD127high and CD62L− as opposed to FOXP3−CD25+ cells which were mostly CD127high but CD62L+. (B) Top panels: quantification of Tregs (CD4+CD25highFOXP3+) in a representative healthy control and two patients in remission. Of note, the Tregs were more frequent in the patients destined to flare. Bottom panels: CD62L expression on Tregs (CD4+CD25highFOXP3+) in a representative healthy control and two patients in remission. Most of the Tregs are CD62L+ in the patients with sustained remission (like in the healthy control) but CD62L− in the patients destined to flare.
Initial treatment group
Markers of sustained remission in patients treated with initial TNF blocker therapy
Sixteen patients (60%) in the initial treatment group sustained remission following cessation of treatment with a TNF blocker. The 11 patients who flared did so within 24 months of stopping the drug (median 14 months, range 9–24 months). More women than men tended to flare (p=0.079).
Baseline pretreatment clinical characteristics
All patients had active RA with a similar median DAS28 of 5.8 before receiving treatment. Nearly one-third of patients in both groups had erosive changes on the plain x-ray (see table 1 in online supplement). There were no differences in HAQ or RAQoL before treatment to account for the outcome following cessation of TNF blockade therapy. Approximately 50% of patients in both groups were antiCCP2 antibody- and RF-positive with no predictive value for flare. However, a trend for a higher level of C-reactive protein at baseline was seen in the group that sustained remission. Sustained remission was, however, clearly associated with shorter symptom duration before starting treatment (median 5.5 vs 9.0 months, p=0.008), and only one patient with a short duration of symptoms (5 months) experienced a flare after stopping treatment.
Clinical and imaging characteristics
There was no significant difference in the clinical features of patients in the two groups (table 3). Neither duration of remission before stopping TNF blocker therapy nor time to achieving remission on treatment was associated with sustained remission.
Early treatment group: clinical, imaging and immunological characteristics
Imaging data were available on 20 patients (table 3). No imaging features were associated with sustained remission, with a similar ratio of patients having PD activity.
Immunological assessment
RF titres were reduced in remission (three patients became seronegative), but they were not associated with sustained remission (see table 1 in the online supplement). Forty-five per cent of patients were also antiCCP2-positive. Similarly, antiCCP2 titres were reduced in remission (data not shown), but higher titres were not associated with flare. When only RF-positive or CCP2-posistive patients were analysed, RF or antiCCP2 titres remained not associated with remission.
Sustained remission showed a significant association with higher naïve T cell frequency (table 3, p=0.001) and lower IRC (p=0.003). Treg frequency was higher in patients who flared (p<0.0001). Analysis of CD62L expression on Tregs showed a significantly lower percentage of CD62L+ Tregs in patients who flared (p=0.033).
Univariate analysis
Univariate exact logistic regression was used to identify which of the following variables was associated with the odds of sustained remission: gender, duration of symptoms before treatment, GS synovial hypertrophy score <2 in all metacarpophalangeal/proximal interphalangeal and wrist joints, subset frequencies for IRC, naïve T cells, Tregs and CD62L+ Tregs. For a number of patients the data were incomplete (imaging data were obtained in 20 patients and not all patients could be further analysed for CD62L Treg phenotype).
Examination of the OR for the categories defined by ‘patients with missing values’ indicated that they were either unrelated to the outcome (table 4) or that patients with missing data were more likely than expected to achieve sustained remission. Such potential bias was identified for ultrasound, IRC and Tregs but, for the immunological variables, so few patients had missing values (n=3 and n=1, respectively) that this effect is likely to have been relatively small. Assuming a worst case scenario and assigning all missing cases to the reference category resulted in a loss of significance for IRC (4/11 (36.4%) patients in the reference category achieved remission; OR for both remaining categories were 4.77 (95% CI 0.51 to 71.41), p=0.300)). Tregs retained significance for the highest category (3/11 (27.3%) patients in the reference category achieved remission; Treg 1.5–2.2%, OR 4.85 (95% CI 0.58 to 54.82), p=0.190; Treg >2.2%, OR 17.66 (95% CI 2.00 to infinity), p=0.008)). GS <2 remained non-significant (8/13 (61.5%) with synovitis >2 achieved remission; OR 0.84 (95% CI 0.14 to 4.98), p=1.000)).
Univariate analysis of predictors of sustained remission: exact OR and CI
The odds of sustained remission were significantly increased in patients with short symptom duration (table 4; OR 13.25, p=0.050), low IRC frequency (OR 16.20, p=0.041), low Treg frequency (OR 23.26, p=0.004) and high proportions of naïve T cells (OR 14.29, p=0.021). The CD62L+ phenotype of Tregs was not informative.
Ninety-one per cent (10/11) of the patients who flared had symptoms for >6 months before receiving combination therapy. All of these patients had low naïve T cell frequencies (≤6%) and 60% had high IRC frequencies (>44%).
Delayed treatment group
Markers of sustained remission in patients treated with delayed TNF blocker therapy
Only three patients were able to sustain remission in this group of 20 patients so no statistical analysis was performed, although these patients had shorter disease duration and better HAQ and RAQoL scores. Immunological parameters showed similar trends to those of the initial treatment group with higher proportions of naïve T cells, lower IRC frequency and more CD62+ Tregs in these three patients.
Discussion
This study addressed the question of when and in whom TNF blocker drugs can be stopped. Guidelines are available on when to start TNF blocker therapy and how to induce remission,18 but there is little information regarding patient management once remission is achieved. For most patients, current practice is to continue treatment indefinitely and to stop only for adverse events or secondary non-response. This study assessed clinical, imaging and immunological measures to establish what happens when successful cessation of TNF blockade therapy is achieved. Importantly, our data are the first to show that successful cessation of TNF blocker therapy is more likely if combination therapy is used as first-line treatment. The low levels of inflammation on ultrasound in these patients provided insufficient variance to be associated with outcome. Immunological findings strongly suggest that a state of immunological suppression of inflammation could be associated with sustained remission when patients were treated early. Commencement of combination therapy within 6 months of symptoms may be associated with an increased likelihood of successful cessation of TNF blocker therapy once remission is achieved.
Initial treatment with combination therapy not only increases remission rates and reduces radiographic progression19 20 but, as suggested by our data, also increases the probability of long-term TNF blocker-free remission. Indeed, these results suggest that, while patients with long-standing RA can achieve remission, these patients will probably require long-term treatment with a TNF blocker to maintain this status as most patients flared (and did so rapidly) after stopping the drug. In contrast, 59% of patients treated with initial combination therapy sustained remission. In these patients, treatment within 6 months of symptoms was most significantly associated with successful cessation. Time to initiate treatment was notably more significant than time to achieve remission after commencing treatment. It has been suggested that women are less likely than men to achieve remission.21 Our data did not address the remission rate according to sex, but we observed that women flared more often than men. It is important to note that no other differences in clinical parameters (such as RF, antiCCP2 antibody, erosions on x-ray) were observed in our patients, which suggests that the patients' clinical ‘phenotype’ did not predict outcome.
Patients successfully ceasing therapy did not have a significant difference in imaging abnormalities, defined by GS synovial hypertrophy and PD activity. In a long-term study of patients with established RA in DMARD-induced remission on stable therapy (ie, did not stop therapy), PD activity predicted future joint damage.22 Our patients in the initial treatment group had persistent GS synovial hypertrophy (80%) and low levels of PD activity (40%). The level of PD activity between these studies was comparable (median PD score 0.5 vs 0); however, only long-term follow-up of these patients will determine the importance of persistent low levels of PD in terms of continued remission and radiographic deterioration. The concern would be that a PD-positive patient in remission could continue to erode radiographically once the protective effect of TNF blocking therapy is ceased.
Sustained remission was associated with low levels of immunological abnormalities, defined by a lower frequency of IRC and a higher frequency of naïve T cells and CD62L+ thymic-derived Tregs. These data therefore support the theory that initial treatment is associated with normalisation of the immune system and/or that successful cessation of treatment can only be achieved when immunological abnormalities are not yet observed. The recapitulation of thymic activity was, however, not observed in DMARD-induced remission in established disease where only a high frequency of IRC predicted flare.10 Tregs, defined as CD4+CD25high only, were also not predictive of flare in patients in DMARD-induced remission.23 It could therefore be postulated that combination therapy is able to ‘switch off’ the inflammatory drive and allow immunological homeostatasis, as suggested previously.24 As TNF is both a major inhibitor of T cell progenitor development in the bone marrow25 and a direct inhibitor of thymic activity,26 recapitulation of thymic activity after TNF blocker therapy can be explained. However, our data suggest that, during the course of RA, the thymus loses the ability to recover from this adverse effect either as a consequence of inflammation or indirectly as a marker of another unknown event. This argues for an early ‘event’ occurring probably within 6 months of continuous inflammation that profoundly affects the immune system. The immunological status of the patients may then switch from reversible to controllable.
In the delayed treatment group, statistical evaluation was limited. However, the very similar data suggest that, for selected patients in remission, successful cessation of TNF blocker may be possible with careful monitoring.
The concept of early treatment for patients with RA is not new as it is recognises that radiographic damage, loss of bone mineral density and loss of function occur early.27 Moreover, there is evidence that very early RA may be an immunopathologically distinct state of disease compared with later disease.28 29 Treatment provided during this so-called ‘window of opportunity’ has allowed improved outcomes (clinical and radiographic), suggesting that the disease can be modified or reversed.4 There is already accumulating evidence that earlier treatment with DMARDs produces better outcomes30,–,32 and that further improvement can be achieved with combination therapies.2 19 33 Our study provides further rationale as to why early treatment is important.
There are several limitations to this study. Missing data may have affected the interpretation of the results, but this has been appropriately dealt with in the statistical analysis. The inclusion of patients in the delayed treatment group who had previously failed a TNF blocking drug may have biased the results in this group. However, at the time of recruitment the outcome of stopping a drug in these patients was not known and further research in this area will determine if this is, indeed, a poor predictor of successful cessation of TNF blocking therapy. The most obvious limitation was the small numbers which made multivariate analysis and hence predictive conclusions difficult. However, the results are emphatic and significant; further work in this area will provide crucial information on which to base decisions regarding the management of patients in remission, with implications for the cost effectiveness of biological therapy.
In conclusion, these preliminary data suggest that successful cessation of TNF blocker therapy is achievable if treatment is commenced early, allowing adequate suppression of inflammation before immunological abnormalities become irreversible.
Acknowledgments
This work has been partly supported by the European Union-funded FP7-integrated project Masterswitch No. 223404 and by a NIHR-RISK grant RC-PC 407-10054.
References
Supplementary materials
Web Only Data ard.2009.117341
Files in this Data Supplement:
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Leeds Teaching Hospital Trust.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous
- Miscellaneous