Article Text

Abstract
Objective To contrast the effect of the burden of vasculitis activity with the burden of adverse events on 1-year mortality of patients with antineutrophil cytoplasmic antibody-associated vasculitis (AAV).
Methods This study assessed the outcome and adverse events in patients prospectively recruited to four European AAV clinical trials. Data on 524 patients with newly diagnosed AAV were included. The burden of adverse events was quantified using a severity score for leucopenia, infection and other adverse events, with an additional weighting for follow-up duration. A ‘combined burden of events’ (CBOE) score was generated for each patient by summing the individual scores. Vasculitis severity was quantified using the Birmingham vasculitis activity score and glomerular filtration rate (GFR).
Results 1-year mortality probability was 11.1%; 59% and 14% of deaths were caused by therapy-associated adverse events and active vasculitis, respectively. Using Cox regression analysis, infection score (p<0.001), adverse event score (p<0.001), leucopenia score (p<0.001) and GFR (p=0.002) were independently associated with mortality. The risk of 1-year mortality remained low (5%) with CBOE scores less than 7, but increased dramatically with scores above this. Hazard ratio for death with a CBOE greater than 7 was 14.4 (95% CI 8.4 to 24.8). Age and GFR were independent predictors of CBOE score.
Conclusions The greatest threat to patients with AAV in the first year of therapy is from adverse events rather than active vasculitis. The accumulation of adverse events, monitored using this scoring method, should prompt increased awareness that the patient is at high risk of death.
Statistics from Altmetric.com
Small vessel vasculitic syndromes (eg, Wegener's granulomatosis and microscopic polyangiitis) are frequently grouped together as antineutrophil cytoplasmic antibody-associated vasculitis (AAV).1,–,6 The introduction of treatment regimens comprising cyclophosphamide and corticosteroids have improved survival.7 However, studies suggest that early mortality remains high, particularly in those patients with renal disease.8
The European Vasculitis Study Group (EUVAS) has undertaken several large prospective trials9,–,12 that have provided the foundation for current AAV therapy. These trials have aimed to reduce the total amount of cyclophosphamide given compared with traditional National Institutes of Health-based regimes, thereby reducing treatment-associated toxicity. Older cyclophosphamide-based regimes were associated with significant morbidity, including opportunistic infections and bladder malignancy.13 14 The current trials provide an ideal opportunity to study treatment and disease-associated morbidity in a very large cohort of well-characterised patients with AAV. These trials represent the spectrum of disease activity in AAV and current therapeutic regimens, which includes non-cyclophosphamide-based regimes for patients with milder disease.
In this study we sought to quantify morbidity associated with disease and treatment and to investigate how it impacts on mortality in the first year after trial enrolment in patients recruited to the four completed EUVAS studies. We aimed to develop a score, based on the accumulation of adverse events, which would alert the physician to patients' risk of mortality.
Patients and methods
Study population
Individual data records from four EUVAS studies performed between 1995 and 2005 were analysed. These trials recruited 544 newly diagnosed patients from 42 hospitals in 11 European countries and Mexico (the list of contributors is included in appendix A, available online only). The protocols (www.vasculitis.org/comptrials.htm) and study outcomes have previously been published in detail (see supplemental table 1, available online only, for summary).9,–,12 All trials were performed according to the Declaration of Helsinki.
Cause of death within the first 12 months following trial entry
Data collection
Data were collected prospectively. Assessments were performed after 0, 1.5, 3, 6, 9 and 12 months, and at the time of relapse. Details of adverse events were recorded by the physician at each visit. To ensure the equivalence of adverse event data quality in those who died compared with those who did not we examined a random selection of data returns. Determinations of cause of death, relapse and adverse events were made by the local investigator and validated retrospectively by an independent observer.
Assessment of AAV severity
Definitions of vasculitis were adapted from the Chapel Hill Consensus Conference on nomenclature of systemic vasculitis.15 Vasculitis activity at presentation was recorded using the Birmingham vasculitis activity score (BVAS).16 Accumulated morbidity was assessed using the vasculitis damage index (VDI).17 Renal impairment at presentation was caused by glomerulonephritis in the context of active vasculitis. The estimated glomerular filtration rate (eGFR) was estimated using the modified modification of diet in renal disease (MDRD) formula.18 For the purposes of analysis in this study, we used the eGFR at study entry. We quantified relapse rate as the number of relapses per patient-year of follow-up.
Assessment of therapy-related adverse event severity
To facilitate the development of a representative summary variable to describe adverse events we developed a ‘combined burden of events’ (CBOE) score. This comprised the sum of three components: infection; leucopenia and other adverse events. We took this approach rather than using a life table analysis incorporating the ‘time to event’ because, first, many patients experienced more than one event during follow-up and, second, adverse events were of varying severity. Each adverse event was scored 1–4 dependent on severity, as defined by the National Cancer Institute terminology criteria for adverse events (http://www.fda.gov/cder/cancer/toxicityframe.htm). For each patient, the burden of events scores (1–4) arising from each event over the first year from trial entry were added together. The cumulative score for all adverse events was weighted for the duration of follow-up (see supplemental table 2 (available online only) and figure 1). Therefore, with no adverse events, the CBOE score would be zero, and if the individual experienced numerous leucopenic, infective and other adverse events, the score may be 30 or higher.

Estimation of weighting factors for each of the three combined burden of event scores. Histograms depict the number of patients developing an event at each time point during the first year of follow-up. There was a strong skew towards events occurring within the first 3 months, thereby precluding the weighting of events in those with incomplete follow-up by simply using the duration of follow-up (see also supplemental table 2, available online only).
Factors associated with mortality within the first year after trial entry on univariable analysis based on Kaplan–Meier and Cox regression proportional hazards approaches
Statistical analysis
Statistical analyses were conducted using SPSS 13 and Graphpad Prism 4.0. For univariable analysis, χ2 and Fisher's exact tests, t test or analysis of variance were used as appropriate. The primary outcome variable was mortality during the 12-month period of follow up, assessed using Kaplan–Meier analysis and compared using the log-rank test. Survival time was calculated from the date of trial entry to the date of censoring (for trial withdrawal or completion of 12 months of follow-up) or death. Parameters associated with a given outcome at a p value of less than 0.1 on Kaplan–Meier analysis were entered into a multivariable Cox proportional hazards model (forward conditional) to quantify independent predictors of mortality (verified using a backward conditional model). In an effort to include the cumulative cyclophosphamide dose in the multivariable model, we designed a time-dependent covariate term that accounted for the fact that the dose changed over time (the majority being given in the first 3–6 months). The syntax for this term is included in appendix B (available online only).
We also calculated the 100-day probability of death directly attributable to an adverse event occurring after each CBOE score increment using Kaplan–Meier analysis. This survival analysis used the date of the score increment as the start date. There is a risk when combining the results of several trials that inhomogeneity across the trials would bias the results. Therefore, we performed further Cox regression analysis including the interaction of trial×CBOE score as an additional variable.
Results
Demographics
A total of 524 newly diagnosed patients was included in this study (see supplemental table 3, available online only). Eighteen patients from the original trials were excluded because of a lack of complete data (nine from MEPEX and nine from NORAM).
Factors associated with developing a CBOE score greater than 7 on multivariable analysis using logistic regression
12-Month patient outcome
Univariable an.alysis
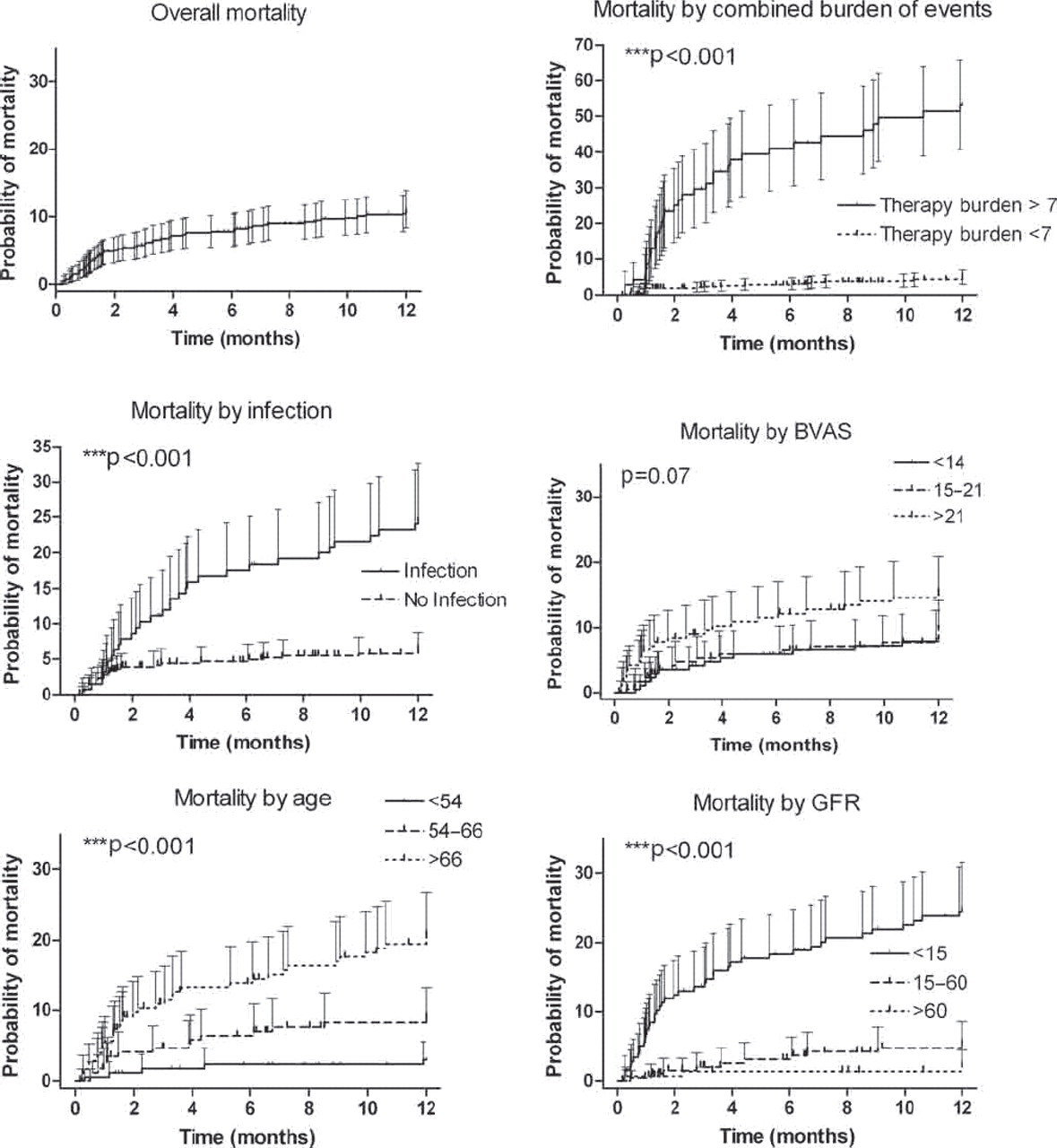
Fifty-six patients (10.7%) died in the first year following trial entry (table 1). Overall, 1-year survival probability was 88.9% (95% CI 86.1% to 91.7%; figure 2). Adverse event and AAV-associated factors associated with overall 1-year mortality are summarised in table 2 and figure 2. Fifty-nine patients (11.3%) developed end-stage renal failure within the first year, of whom 23 died. The 1-year probability of end-stage renal failure (censored for patient death) was 8.6% (95% CI 5.9% to 11.3%).

Factors associated with 1-year mortality on univariable Kaplan–Meier analysis. Factors compared using the log-rank test are combined therapy burden greater than 7/less than 7, the presence or absence of an infectious episode during follow-up, tertiles of Birmingham vasculitis activity score (BVAS) at presentation, tertiles of age and approximate tertiles of glomerular filtration rate (GFR). Error bars depict the 95% CI.
In 33 of the 56 patients who died (59%), the cause of death was classified primarily as a result of an adverse event (including 28 deaths due to infection, table 1), whereas death as a result of active vasculitis occurred in only eight patients (14%). The last median recorded BVAS before death was 0 (interquartile range (IQR) 0–14), 12 individuals having some active vasculitis at the time of death. One-year infection-related mortality probability was 5.6%. The actuarial probability of death due to active vasculitis was 1.4% at 1 year.
There were 698 adverse events in 347 (66%) patients (25% classified as grade 3–4). The overall median weighted CBOE score was 2 (range 0–75.3). The frequency of CBOE is shown in supplemental figure 1 (available online only). There was a marked increase in mortality as the CBOE score climbed above 7 (figure 3); a CBOE score greater than 7 was associated with a probability of death of 53.1% (95% CI 40.7% to 65.0%) by 12 months compared with those with a CBOE score less than 7, who had a 1-year probability of death of 5.0% (95% CI 3.0% to 7.1%). In those with a CBOE score greater than 7 (N=70, 13.4%), the most common cause of death was infection (24 of 34 deaths, 71%), whereas in those with a score less than 7 (N=454, 86.6%), the commonest cause of death was active vasculitis (five of 22 deaths, 23%). No centre effect was detected in the reporting of adverse events (data not shown).

Probability of mortality in the first year after trial enrolment according to the combined burden of events (CBOE) score. Probability of death was determined for each incremental increase in CBOE by Kaplan–Meier analysis. The error bars depict the 95% CI. 12-Month mortality was under 10% until the combined score rose above 7, above which the probability of death increased dramatically. This analysis provided the rationale for choosing this level as the cut-off point. CBOE=0 implies no adverse events.
As morbidity associated with adverse events accumulated over time, the probability of dying from a cause directly associated with those adverse events escalated: the 100-day probability of adverse event-associated death was 0.7% (95% CI 0% to 2.2%) upon acquiring a CBOE score of 1, 8.1% (95% CI 1.2% to 14.9%) once reaching a score of 4, and 27.8% (95% CI 4.5% to 51.1%) once reaching a score of 8 (p<0.001).
Multivariable analysis
Mortality
To look at predictive factors of mortality we performed a multivariable analysis using factors associated with mortality in the univariate analysis. The degree of renal impairment remained predictive of mortality on multivariable analysis, but age and vasculitis type were not. Infection and leucopenia were only moderately correlated in this study and, therefore, we included these as independent variables in the multivariable analysis. Weighted infection, leucopenia and adverse event scores were each independently associated with early mortality (table 2), even after controlling for cumulative cyclophosphamide dose (as a time-dependent covariate), which was itself weakly associated with mortality. As we had performed the analysis using heterogeneous trials, we examined the data further to ensure our findings were not confounded by trial allocation. After adjusting for the glomerular filtration rate (GFR) and the CBOE score, mortality did not vary significantly between the four trials (p=0.19), and there was no evidence to suggest that the relationship between CBOE and mortality (adjusted for GFR) varied between trials (p=0.52). Mortality was independently predicted by both the severity of disease and the accumulation of adverse events.
Factors associated with infection, leucopenia and other adverse events
As we observed a sharp increase in 1-year mortality (figure 3) as the CBOE rose above 7 we performed a multivariable logistic regression model (table 3) to identify those factors independently associated with developing a CBOE score greater than 7, using vasculitis type and gender as fixed factors, and age, eGFR, BVAS and relapse rate as covariates. The degree of renal impairment and, to a lesser extent, advanced age, were independently associated with a CBOE score greater than 7. The median eGFR in those with a CBOE score greater than 7 was 8.2 ml/ min (IQR 4.9–29) compared with 32.2 ml/min in those with a CBOE score less than 7 (IQR 12.2–70.0, p<0.001). There was a sharp increase in the CBOE score in those with eGFR less than 25 ml/ min (figure 4). We repeated the logistic regression analysis in each of the four trials separately to assess whether there was a trial-specific effect. Although the strength of the association was much less as a result of the smaller sample sizes, the overall association of age and GFR with severe adverse events held true across the trials, except for NORAM (in which all patients had essentially normal GFR, thereby removing the association with GFR).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Factors associated with combined burden of events (CBOE) score on univariable analysis. (A) Association of excretory renal function with the development of a combined therapy score greater than 7. Line and error bars indicate median and interquartile range. (B) Association of age with the development of a CBOE score greater than 7. Line and error bars indicate median and interquartile range. (C) Scatter plot depicting the change in combined therapy burden score with changing estimated glomerular filtration rate (eGFR). The line depicts the best-fit non-linear regression line (one phase exponential decay) with 95% CI. There was a steep increase in CBOE score with eGFR less than 25 ml/min. (D) Burden of therapy according to the trial enrolled in. Bars depict the mean±SEM, ***p<0.001.
To illustrate the importance of age and GFR in the accumulation of adverse events in clinical practice, we compared two groups of patients: the mean CBOE score in those aged over 60 years with an eGFR less than 15 ml/min (n=128) was 7.3 (95% CI 5.4 to 9.2), compared with 1.3 (95% CI 0.9 to 1.7) in those under 50 years and with eGFR greater than 60 ml/min (n=72).
Description of adverse events
Infection
One hundred and forty-two episodes of infection (60 with score 3–4) occurred in 128 patients (24%). The commonest bacterial infections were of the respiratory tract (47 episodes) or generalised septicaemia (29 episodes, see supplemental table 4, available online only). Half the infections occurred within the first 2 months.
Leucopenia
Three hundred and ten episodes of leucopenia (57 graded 3–4) occurred in 215 patients (41%). There was an incremental increase in mortality risk with increasing leucopenia severity. Compared with no episode of leucopenia, leucocyte counts of 1–2×109/litre and less than 1×109/litre were associated with a hazard ratio for death within the first year of 2.6 (95% CI 1.1 to 6.3, p=0.036) and 6.7 (95% CI 2.9 to 15.5, p<0.001), respectively. At the time of leucopenia 74% of patients were receiving cyclophosphamide.
Steroid-associated side-effects
Forty-three patients (8.2%) developed new-onset steroid-associated diabetes (event rate 9.4/100 patient years, 95% CI 6.8 to 12.5), 50% within the first 1.7 months. Thirteen patients (2.5%) had a fracture, two (0.4%) developed avascular necrosis of the hip, 13 (2.5%) developed peptic ulceration and nine (2%) developed cataracts during the period of follow-up. There was no difference in the incidence of steroid-related complications between trials (p=0.75).
Cyclophosphamide, methotrexate and azathioprine intolerance
Twenty-five of 206 (12%) patients exposed to azathioprine developed intolerance/hypersensitivity to the drug. Three of these (1%) had persistent fever and one had altered liver blood tests. Cyclophosphamide hypersensitivity occurred in four patients of 478 (1%) exposed. In addition, four (1%) developed chemical cystitis and five cases of amenorrhoea were reported. However, we cannot calculate the true incidence of amenorrhoea as we did not collect information on which patients were at risk. Methotrexate intolerance was present in three of 46 (7%) patients, all of whom had abnormalities in liver function.
Vascular and thrombotic events
Eleven (2%) and six (1%) patients had a cerebrovascular event and myocardial infarct, respectively. The rate for a cardio/cerebrovascular event was 3.7 episodes/100 patient years (95% CI 2.24 to 5.82). Eighteen patients (3.4%) had venous thrombotic events, including six pulmonary emboli, 11 deep vein thromboses and one episode of vascular access thrombosis. Excluding the vascular access thrombosis, the event rate was 3.7 episodes/100 patient years (95% CI 2.23 to 5.82).
Discussion
In this study, the largest reported study of AAV, we have reported the morbidity and mortality in the first year of patients with AAV, and have highlighted the importance of both disease severity and the accumulation of adverse events in early death in this group. Using a novel scoring mechanism to quantify the CBOE, we found that the triad of leucopenia, infection and other adverse events were strong independent predictors of early mortality. The previously reported association between death and GFR (the most robust marker of ‘vasculitis burden’) also remained predictive of mortality in this multivariable analysis, although less so than the burden of adverse event scores. The greatest challenge facing the clinician treating patients with AAV is to recognise those patients at highest risk of death. We have demonstrated that the burden of adverse events is predicted by the severity of renal impairment and advanced age. These together hold the greatest threat to the patient in the first year, supporting the drive to find new and safer therapies for patients with AAV. We have proposed the use of the adverse event scoring mechanism in individual patients as a means of monitoring the level of risk of mortality. This study highlights the multifactorial nature of factors underpinning early death in these patients.
The EUVAS study group has stratified patients into disease severity groups to study therapeutic protocols. This study shows the success of this approach as patients with more severe disease have worse outcomes requiring a different approach to therapy. These studies support the approach of tailoring therapeutic regimens towards disease severity. One-year survival in this study was 88.9%, with most deaths occurring in the first 3 months, in concordance with the early mortality seen in other studies.8 19 This reflects the period of both greatest immunosuppression and vasculitis activity.8 19 The complex interplay between vasculitis severity and the risk of experiencing adverse events was illustrated by the finding that the principal predictor of adverse events was renal function. It is likely that this interrelationship underlies findings in previous studies, in which GFR has been consistently found to be the greatest overall predictor of mortality.7 It is probable that renal failure predisposes to adverse drug metabolite excretion characteristics20 (among other factors) and, consequently, a markedly increased risk of adverse events. Renal insufficiency in itself also increases the risk of infection irrespective of treatment.19
The association between vasculitis severity and the risk of adverse events is also exemplified by the strong relationship between GFR and leucopenia. As most patients developed leucopenia while receiving cyclophosphamide this study supports that dose reductions of this drug are required in those with impaired renal function. Despite the frequent use of cyclophosphamide in patients with impaired renal function, dose alterations are controversial in renal failure and, when implemented, may be undertaken in a crude step-wise manner. Some studies report no changes in pharmokinetics or toxicity profiles,21,–,23 whereas others have shown decreased clearance with enhanced toxicity in severe renal failure.24 25 A recent well-conducted study showed reduced clearance of cyclophosphamide metabolites with impaired GFR.20 Given the clear overrepresentation of infection and leucopenia in those with reduced GFR, research efforts should focus on improved cyclophosphamide dosing and the development of a more clinically sensitive biomarker to detect effective cyclophosphamide over-dosage than leucopenia. Indeed, the dose reductions for renal impairment in patients treated in the CYCLOPS study with pulse cyclophosphamide resulted in less leucopenia than in the daily oral limb, which reduced dose for age but not renal function.12
Despite improving survival, adverse events remain problematical and greater emphasis should be placed on prevention. This study supports EUVAS guidelines advocating Pneumocystis carinii pneumonia prophylaxis (which is cost-effective in patients with AAV),26 27 vaccination against Streptococcus pneumoniae and influenza28 and the use of granulocyte colony-stimulating factor therapy during neutropenic episodes29. Thrombotic events are common30 31 and prophylactic therapy during high-risk periods should be considered. This study supports previous studies, which reported that current therapeutic regimens are associated with significant toxicity (particularly infection).19 However, unlike other studies, our study attempts to quantify the risk of death associated with cumulative adverse events.
The scoring system and adjustment for the duration of follow-up that we used to quantify adverse events are imperfect. First, they assume that severe and mild adverse events occur with the same time distribution. This is not strictly accurate as more severe adverse events tended to occur earlier than mild adverse events (data not shown). Second, the correction factor applied to account for those with incomplete follow-up will underestimate the duration for those with a follow-up, say, of 5.2 months (which would be considered as 6 months). Third, the total number of patients at risk falls slightly (from 524 to 424) as one moves through the first year of follow-up. The latter two caveats mean that the correction factor would tend to underestimate the given CBOE score. Given this small underestimation, the models as described actually tend to be conservative in their estimates of risk attributable to the burden of therapy. We felt that the benefit of using more complex models would be outweighed by a loss of potential clinical utility of the scoring systems. The scoring system as presented represents, in our opinion, the best balance of complexity versus utility.
Is it possible to predict those who will run into life- threatening problems? It is clear that morbidity accumulates progressively over time and that, as incremental morbidity events occur, the risk of a subsequent life-threatening event occurring increases dramatically. Indeed, the risk of death due to an adverse event within the following 100 days after an adverse event increased from under 1% with one minor event, to almost 10% as one reaches a CBOE score of 4, and up to nearly 30% as one reaches a score of 8. These CBOE scores are not uncommon in clinical practice. For example, if a patient with AAV developed steroid-induced diabetes, followed by cyclophosphamide-induced leucopenia to 1.0×109/litre, followed by an episode of pneumonia requiring hospital admission, this patient would have, statistically, an approximately one in three chance of dying from an adverse event over the following 3 months. The accumulation of adverse events to this extent should provide a strong alert to the clinician that the patient is at high risk of death, particularly in the elderly and in those with reduced renal function. Measures should be taken to prevent further toxicity. Recording of CBOE scores may be a useful component of patient care and clinical trial design, analogous to BVAS and VDI.
The principal strength of this study is that all data were captured prospectively under trial conditions, thereby maximising the accurate reporting of adverse events and vasculitis activity. The study population was drawn from four studies representing a diverse group of patients. Although the demographics and treatment regimens differ between the trials, this strengthens our conclusions. We statistically excluded an effect specific to a given trial (over and above the severity of disease in that trial), the overall findings remaining robust across the four trials. Our findings should therefore be applicable to most patients with AAV.
Although there has been considerable improvement in survival since the introduction of cyclophosphamide-based treatment regimens, this study highlights the large number of adverse events that occur following the diagnosis and treatment of AAV. There remains a need for therapies that are quickly efficacious in controlling disease activity to reduce scarring and that have a low toxicity profile. Mortality is predicted by age, impaired renal function and the accumulation of adverse events.
Acknowledgments
The authors are very grateful to Dr Michael Walsh, Addenbrooke's Hospital, Cambridge, for statistical advice. This study was presented in part at the American Society of Nephrology annual meeting, Philadelphia, November 2008.
References
Supplementary materials
Web Only Data ard.2009.109389
Files in this Data Supplement:
Footnotes
-
Funding Funding for this study was provided by the Higher Education Funding Council of England (HEFCE), the European Union (European Community Systemic Vasculitis Trial project, contract nos BMH1-CT93-1078 and CIPD-CT94-0307, and the Associated Vasculitis European Randomised Trial project, contract nos BMH4-CT97–2328 and IC20-CT97-0019), European Union League Against Rheumatism project grant 2004–7 EULAR Standardisation of Disease Assessment in Systemic Vasculitis, and the Renal Association, UK.
-
Ethics approval Each of the four trials had full ethics approval.
-
Provenance and peer review Not commissioned; externally peer reviewed.