Article Text

Abstract
Background: The ASAS/EULAR (Assessment of SpondyloArthritis International Society/European League Against Rheumatism) recommendations for the management of ankylosing spondylitis (AS) have been developed by rheumatologists for a target population of health professionals.
Objective: To extend the cooperation between ASAS and EULAR by translating the recommendations into a language that can be easily understood by patients in order to further disseminate and evaluate the recommendations.
Methods: In cooperation with patient organisations 18 patients with AS (17 European, one Canadian) were invited to attend a meeting in February 2008. As a starting point the original publication and a version created by Canadian patients with AS were used. To improve the understanding of potential problems, data on the evaluation of a recent German translation were presented. After intensive discussions the wording was adjusted and a vote was held on the new wording of the recommendations aiming for >80% agreement on each sentence. Finally, patients were asked to indicate their level of agreement with the content of the recommendations.
Results: Ten recommendations were successfully translated into a patient-understandable version. The original text was changed in most cases. In all but one case (recommendation No 4) there was broad agreement with the proposed translation. The overall agreement with the content of the recommendations was high: 8.7 (0.6).
Conclusion: For the first time, EULAR recommendations were successfully converted into a patient-understandable language version by a large international group of patients in collaboration with rheumatologists. The evaluation showed broad agreement. Translations into different languages and further dissemination in individual countries will be performed.
Statistics from Altmetric.com
Ankylosing spondylitis (AS), the main entity of the spondyloarthritides, is a chronic inflammatory disease characterised by specific musculoskeletal features: inflammation and ankylosis of the axial skeleton, peripheral arthritis, enthesitis and involvement of other organs such as the eye.1 Major advances in the management of AS have recently been made by introduction of magnetic resonance imaging (MRI) and the tumour necrosis factor (TNF)α inhibitors.2 ,3 To assist all health professionals involved in the care of patients with AS, evidence-based recommendations for the management of this disease were developed.4
The Assessment of SpondyloArthritis International Society (ASAS) has published recommendations for the use of anti-TNF therapy in AS,5 and together with the European League Against Rheumatism (EULAR) recommendations for the management of AS in 2006 (supplementary data 1 and 2, available online) based on a systematic literature search.6 ,7 These were drafted by a combination of evidence and expert consensus. Treatment recommendations for AS have also been released by the Canadian Rheumatology Association/Spondyloarthritis Research Consortium of Canada working group.8 ,9
The ASAS/EULAR recommendations were an important step forward in generating an international consensus on the appropriate management of AS. However, they have been developed by rheumatologists and orthopaedic surgeons for a target population of mainly health professionals and payers, and the language of the publication is largely medical. In a chronic disease, sustainable patient knowledge is beneficial and patient input into the decision-making process of recommendations is a requirement by various institutions. The importance of patients’ views and preferences is also included in the Appraisal of Guidelines for Research and Evaluation (AGREE) instrument for evaluation of guidelines.10 However, the mechanism by which this is best accomplished has not been well defined.
ASAS and EULAR have agreed to extend their cooperation by translating recommendations into a language that can be easily understood by patients. At a consensus meeting of rheumatologists and deputies of national patient organisations, the ASAS/EULAR recommendations for the management of AS were translated into a language that can be understood by patients with AS in order to further disseminate and evaluate the recommendations among patients.
Methods
Participants
In cooperation with EULAR (PARE, People with Arthritis/Rheumatism in Europe), the Ankylosing Spondylitis International Federation (ASIF), the Deutsche Vereinigung Morbus Bechterew (DVMB), the National Ankylosing Spondylitis Society (NASS) and other national patient organisations, 18 patients with AS (including one rheumatologist) of 10 different countries (Belgium, Canada, Germany, Ireland, the Netherlands, Portugal, Romania, Switzerland, Turkey, United Kingdom) were invited to attend a consensus meeting at the EULAR house near Zurich in February 2008. A planning committee was formed from within ASAS (J Braun as convener, D van der Heijde as clinical epidemiologist, H Mielants as an experienced clinician and ASAS member), EULAR (M de Wit) and ASIF (E Feldtkeller). Demographic characteristics, partial history and current health status of the participants were collected. This included questions to be answered by a visual analogue scale, the Bath AS Disease Activity Index (BASDAI) and the Bath AS Functional Index (BASFI).
Working document
As a starting point, the original publication and a version created by Canadian patients with AS were used. K Mulholland, a patient with AS who was strongly involved in the Canadian project, attended the meeting to explain the development of this patient-based version.9 To improve the understanding of potential problems, data on the evaluation of a recent German translation of the experts version evaluated by patients were presented during the meeting.11
Translation process
Each participant of the consensus meeting was asked to contribute independently proposals relevant to translation of the patient version of the ASAS/EULAR recommendations for the management of AS. The aim was to create a new manuscript that was produced and understood by patients. To achieve this, the main task was to translate the original text by simplifying the wording and to explain the original text by adding comments to a patient-friendly version. However, it was stated at the beginning of the meeting that modification of the meaning of the original recommendations was not allowed. After the participants had generated 10 patient-adapted recommendations, comments explaining difficult terms were discussed and a wish list was developed for possible consideration in the next update of the ASAS/EULAR recommendations for the management of AS.
Evaluation
After intensive discussions a vote was held on the new translation of the recommendations aiming for >80% agreement on the translation. The participants had the option to agree (positive vote), to disagree (negative vote) or to be neutral (no vote) on the translation of the patient version. When a vote was negative the participants were asked to state the reason for their disagreement. Finally, based on the content of the recommendation, patients were asked to rate the strength of recommendation on a numerical rating scale for each recommendation (0 = do not agree at all, 10 = fully agree).
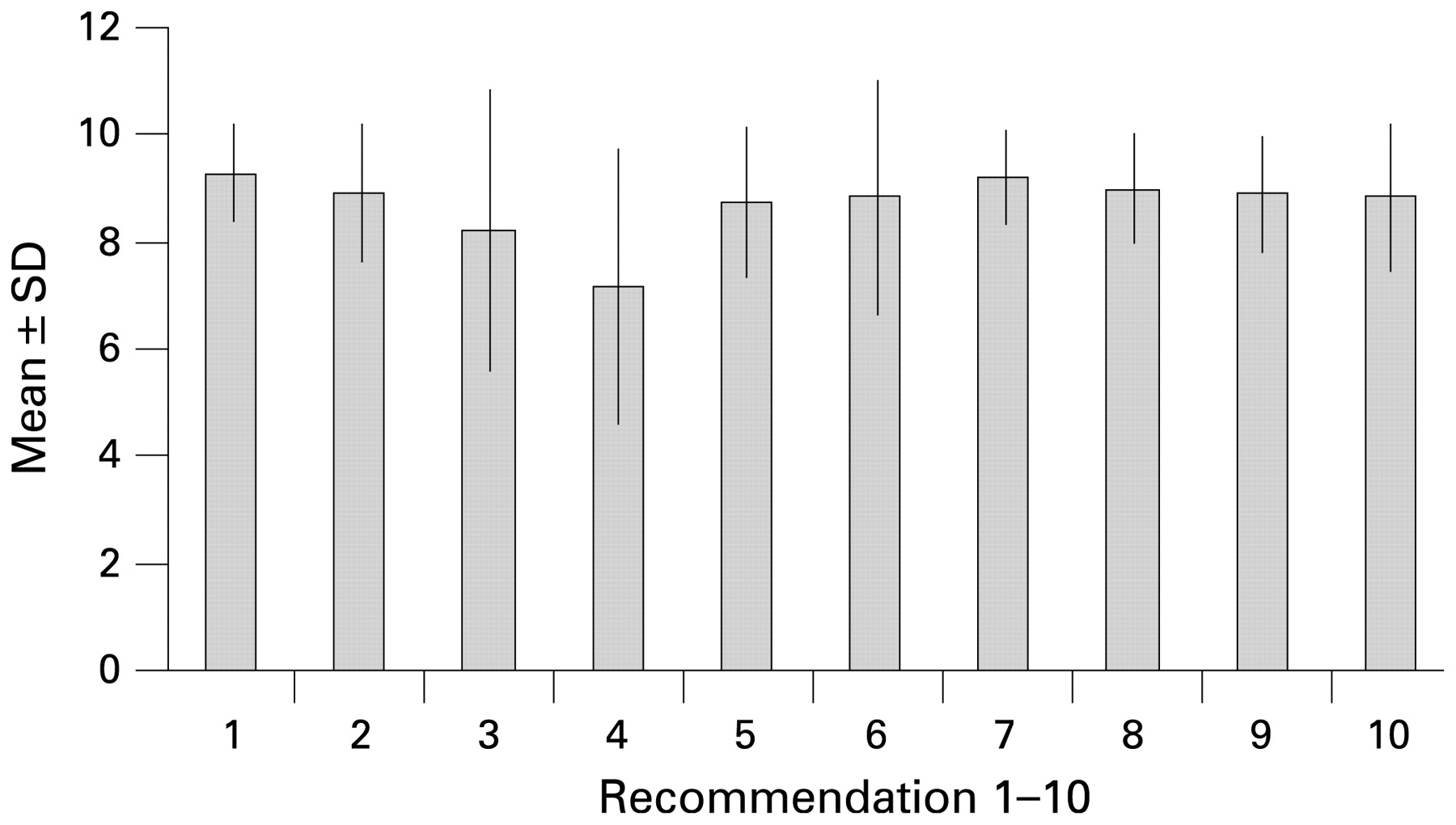
Figure 1 gives the strength of each recommendation as assigned by the participants.

{kind=link}
Strength of recommendations 1–10.
Results
Characteristics of the participants
The baseline characteristics of the participants are given in table 1.
Characteristics of the participants (17/18 with available data)
Translation and evaluation of the patient version
Ten recommendations were successfully translated into a patient-adapted version. The first three recommendations deal with general concepts in the management of AS, the remaining seven describe specific treatments in use for AS. The original text was changed in most cases.
Box 1 shows the full recommendations of the patient version; comments on each recommendation are presented in table 2, while the evaluation of the recommendations (translation and agreement) is shown in table 3.
Comments on recommendations 1–10
Evaluation of the recommendation
Box 1 Recommendations for the management of ankylosing spondylitis (AS) in lay language
Recommendation 1: General principles for management
The treatment of AS should be specifically adapted for individual patients according to:
-
How the disease currently affects the patient (spine, joints, attachments of ligaments and tendons*, other locations*)
-
The level of current symptoms, findings on examination and features that predict how the disease may progress, as indicated by:
-
-
disease activity*/inflammation
-
pain
-
function and disability
-
damage to the spine and hip*†
-
-
The general medical condition (age, sex, other diseases, medication)
-
The patient’s wishes and expectations
Recommendation 2: Disease monitoring
-
Disease monitoring* should relate to the patient’s current health. It includes patient history (eg, questionnaires), physical examination, laboratory tests and imaging* (eg, x-rays), based on the core set* of measurements recommended by ASAS*
-
The frequency of monitoring should be decided for each individual patient based on current symptoms, severity and medication
Recommendation 3: Management strategy
Optimal management* of AS requires the use of both drug and non-drug treatments
Recommendation 4: Non-drug treatment
Non-drug treatment of AS should include patient education† and regular exercise. Individual and group physiotherapy† under the supervision of a qualified therapist should be considered. Patient associations and self-help groups† may be useful
Recommendation 5: Drug treatment: anti-inflammatory drugs
-
Anti-inflammatory drugs* (not including steroids) are recommended as first choice for patients with AS suffering from pain and stiffness
-
For patients with an increased risk of side effects in the stomach there are two options:
-
-
an additional drug that protects the stomach, or
-
an anti-inflammatory drug with a reduced risk for side effects in the stomach (selective COX-2 inhibitor*)
-
Recommendation 6: Drug treatment: pain killers
Pain killers such as paracetamol and opioids* might be considered for pain control when anti-inflammatory drugs:
-
Have not provided sufficient relief
-
Have caused unacceptable side effects
-
Cannot be used because of other medical reasons
Recommendation 7: Drug treatment: steroids
-
Local injections of steroids* at the site of inflammation* may be considered
-
The benefit of steroids given in other ways is not proven when the disease is only present in the spine
Recommendation 8: Drug treatment: DMARDs
-
It is not proven that so-called disease-modifying antirheumatic drugs (DMARDs*), such as sulfasalazine† and methotrexate, are effective for the treatment of AS in the spine
-
Sulfasalazine may be effective in those patients who have inflammation in joints outside the spine
Recommendation 9: Drug treatment: anti-tumour necrosis factor (anti-TNF)
-
If the treatments outlined above do not control disease activity sufficiently, anti-TNF* drugs should be given in line with the ASAS recommendations*
-
It is not necessary to use DMARDs before or together with anti-TNF treatment in those patients who only have disease in the spine
Recommendation 10: Surgery
-
Total hip replacement* should be considered, regardless of age, in patients with pain or disability not responding to treatment and where there is x-ray evidence of joint damage
-
Spinal surgery may be of value to correct severe deformity* or stabilise* the spine
*See comments 1–10 (table 2); †see wish-list (table 4).
Wish list of the patients for possible consideration in the generation of the next update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis (AS)
Table 4 contains the wish list.
Translation
In general, common speech was preferred as a translation of Latin terms in the expert’s version (eg, comorbidity → other diseases, concomitant drugs → medication (recommendation 1)). But not all medical language can be rendered in lay terms (eg, COX-2 inhibitor). In such cases, the term is commented on in table 2. We deleted words in some instances (like “structural” (recommendations 1 and 10) or “persistently” (recommendation 9) where the use or translation of these words did not contribute to a better understanding of the patient-adapted version.
To emphasise the heterogeneity of the clinical picture of AS, the term “current manifestation” in recommendation 1 was changed to “other locations” as explained in the “comments” section. The participants needed an explanation for the understanding of the term “clinical” in recommendations 1 and 2. We consequently decided to change it to “findings on examination” or “medical condition”.
The term “function, disability, handicap” in recommendation 1 refers to the model of functioning developed by the World Health Organization (WHO). Most patients accepted dropping “handicap” in the patient-adapted version, deciding that handicap is included in the word “disability”.
For the division into non-pharmacological and pharmacological treatment options (recommendation 3) it was decided to generally change the word “pharmacological” to “drug” for better understanding. As the majority of the recommendations deal with pharmacological treatment, there was an intense discussion about several problems with understanding of, and agreement with, recommendations 5–9. Because participants expected that many non-health professionals would have difficulty understanding pharmacological terminology, we used the common term “anti-inflammatory” instead of non-steroidal anti-inflammatory drugs (NSAIDs), emphasising explicitly that this does not include corticosteroids. The experts and participants discussed the translation of “gastrointestinal” intensively. In the patient version the term “stomach” is used ignoring the potential intestinal side effects of NSAIDs. The terms “gut” and “bowel” were also discussed but the majority of the participants found the term “stomach” easier to understand. The structure of recommendation 5 and 6 was changed extensively for improved understanding.
Evaluation
Agreement with translation of the recommendation was evaluated separately for each recommendation. In all but one case there was broad agreement with the proposed translation. Full agreement of all participants with the translation was achieved in recommendations 1, 7, 8 and 9. Not more than one disagreement was achieved in recommendations 2, 3, 5, 6 and 10. For recommendation No 4 disagreement was expressed by 4/18 participants (22%). However, this largely related to the content of the recommendation and not to the actual translation.
The overall agreement with the content of the recommendations was high (mean (SD) agreement: 8.7 (0.6)). Agreement was highest for recommendation 1 (general principles for management) and for recommendation 7 (drug treatment: steroids) (mean (SD) 9.3 (0.9) and 9.2 (0.9), respectively). Agreement was lowest for recommendation 4 (non-drug treatment) with a mean (SD) value of 7.2 (2.6).
Discussion
This is the first translation/transformation of EULAR recommendations into a patient-adapted version. This effort is a major step forward in the process of evaluation and dissemination to health professionals as well as to non-health professionals as required in the EULAR standardised operating procedures.12 The original ASAS/EULAR recommendations for the management of AS published more than 2 years ago have already been evaluated in different countries.4 ,13 ,14 ,15 In Canada, a first effort was undertaken to try this also at the patient level.9 Support of patient knowledge and participation in the management of chronic diseases is likely to be beneficial since it is well established that one powerful strategy to change behaviour of patients is to involve them directly in the development of guidelines or recommendations.16
This is the first time that patient-adapted recommendations for the management of AS have been developed with direct participation of patients in a consensus meeting. In this way the 10 key recommendations of the expert’s version (online supplementary data 1) were successfully translated into a patient-understandable language (box 1). Indeed, the notable and most important experience in this meeting was that it was not a great problem to agree on this patient-adapted version of the recommendations for the management of AS among a rather mixed group of patients with AS from 10 different European countries. The involvement of patients with many different native tongues enhances the likelihood that the present language version can be easily understood by many patients and also easily translated into various languages as specific English wording is avoided. Although there was a lot of discussion, it was eventually possible to agree on the basis of a majority vote, with >80% agreement in almost all cases. Participants accepted that the basic content of the original recommendations could not be changed during this translation process. Considerable time was spent on discussions relating to the content of the recommendations (importance of non-pharmacological treatment options, use of opioids and corticosteroids, etc). The patients prepared a wish-list for further consideration in the next update of the recommendations, in which most of the discussion regarding the content is summarised (table 4). Although patients were aware that the content of the recommendation could not be changed, it is quite obvious that in some cases (eg, recommendation No 4) the patients vote on the translation was influenced by disagreement about the content of the recommendation. This difficulty can be reduced if the patients with AS are allowed to participate in the development of recommendations at an earlier stage.
This patient version of the ASAS/EULAR recommendation for the management of AS should serve as a preliminary step for the development of the ASAS/EULAR management recommendation update and also for further evaluation and dissemination in individual countries where a broader array of patients should be included. Thus, the patient version will be forwarded to ASAS members in all EULAR countries with the request that they perform a translation in cooperation with their national patient organisation. For this national translation process, the disease status and educational level of the group of participants should be heterogeneous. This was not the case in our group of patients with AS because the success of creating an international patient version depends on excellent knowledge of the English language of all participants. The dissemination and evaluation of the national patient versions will be checked after 1 year.
The participants stated during the discussion that factors other than body functions and structures have to be discussed as an important aspect of disease progress (recommendation No 1). According to the composition of the International Classification of Functioning, Disability and Health developed by the WHO for describing functioning of people with ill health, aspects of activity and participation of the patients have also to be considered.17 In this framework, function is not narrowed to a biomedical function but environmental and personal factors are also taken into account. Recently, this was applied to patients with AS.18
The study on dissemination and evaluation of the health professionals’ publication of the ASAS/EULAR recommendations for the management of AS among European rheumatologists has already shown that conceptual agreement with the recommendations was very high, as was self-declared application by rheumatologists (8.9 (0.9) and 8.2 (1.0), respectively).13 Potential barriers to the application of the ASAS recommendations include primarily insufficient funding and administrative burden for anti-TNF therapy and patient concern about the safety of pharmacological therapy. Barriers to the use of the non-pharmacological treatment are lack of consultation time, insufficient number of qualified physiotherapists, lack of facilities for education and lack of patient compliance with recommendations. Similar to the European evaluation, a broad agreement with the recommendations was achieved by an evaluation in the German language area and in Mexico.14 ,15
For the first time, EULAR recommendations were successfully converted into lay terms by a large international task force of patients in collaboration with rheumatologists. This can be seen as a starting point for the dissemination and implementation of the patient version to provide guidance for monitoring and treatment of patients with AS. Further translations into different languages and appropriate evaluations in larger patient groups will be performed.
Acknowledgments
We acknowledge the contributions of NASS, the AS patient organisation of the UK in identifying the participants. We appreciate the explanation by K Mulholland of the development of the Canadian patient-based version of the ASAS/EULAR recommendations.
Appendix 1: List of participants
John Barnes; Ireland; Campbell Barr, UK; David Blythe, UK; Philippe Carron, Belgium; Cor van Drogen, The Netherlands; Eric Eustance, UK; Ernst Feldtkeller, Germany; Barbara Foster, UK; Hedley Hamilton, UK; Merryn Jongkees, The Netherlands; Uta Kiltz, Germany; Jose Luis Lopes, Portugal; Ken Mulholland, Canada; Joke Nijns, Belgium; Salih Özgocmen, Turkey; Eckhard Pfeiffer, Germany; Peter Staub, Switzerland; Corina Stefan, Romania.
REFERENCES
Supplementary materials
Web Only Data 68:9;1381
Files in this Data Supplement:
Footnotes
-
▸ Additional data are published online only at http://ard.bmj.com/content/vol68/issue9
-
Funding The consensus meeting in Zürich was financially supported by EULAR. There are no other financial disclosures. The sponsors had no role in voting, or in developing the final document.
-
Competing interests None.