Article Text

Abstract
Purpose: To study patterns and predictors of medication use and laboratory monitoring in gout.
Methods: In a cohort of veterans with a diagnosis of gout prescribed allopurinol, colchicine or probenecid, quality of care was assessed by examining adherence to the following evidence-based recommendations: (1) whether patients starting a new allopurinol prescription (a) received continuous allopurinol, (b) received colchicine prophylaxis, (c) achieved the target uric acid level of ⩽6 mg/dl; and (2) whether doses were adjusted for renal insufficiency. The association of sociodemographic characteristics, healthcare utilisation and comorbidity with the recommendations was examined by logistic/Poisson regression.
Results: Of the 643 patients with gout receiving a new allopurinol prescription, 297 (46%) received continuous allopurinol, 66 (10%) received colchicine prophylaxis and 126 (20%) reached the target uric acid level of ⩽6 mg/dl. During episodes of renal insufficiency, appropriate dose reduction/discontinuation of probenecid was done in 24/31 episodes (77%) and of colchicine in 36/52 episodes (69%). Multivariable regression showed that higher outpatient utilisation, more rheumatology care and lower comorbidity were associated with better quality of care; more rheumatology clinic or primary care visits were associated with less frequent allopurinol discontinuation; more total outpatient visit days or most frequent visits to a rheumatology clinic were associated with a higher likelihood of receiving colchicine prophylaxis; and a lower Charlson Comorbidity Index or more outpatient visit days were associated with higher odds of reaching the target uric acid level of ⩽6 mg/dl.
Conclusions: Important variations were found in patterns of medication use and monitoring in patients with gout with suboptimal care. A concerted effort is needed to improve the overall care of gout.
Statistics from Altmetric.com
Gout is a common debilitating arthritis affecting 1% of the adult population; its incidence is increasing. Effective affordable treatments are available, leading to less frequent flares; almost no flares occur when the serum uric acid (SUA) level is <6 mg/dl.1 Prescription errors are common.2–6 Flare-ups of chronic gout occur frequently, bringing significant pain and disability.7 Fewer than 50% of patients reach the target SUA of ⩽6 mg/dl using allopurinol at the most common dose of 300 mg/day,8 9 which a few patients exceed.10–12 SUA checks are recommended before initiating uric acid-lowering therapies and again within 6 months to titrate the dose needed to achieve the target uric acid level.13 Interrupting allopurinol use leads to more frequent exacerbations/flares.14
Owing to transient increases in flares after allopurinol initiation/titration, colchicine prophylaxis is recommended.15 The optimal duration of colchicine prophylaxis is unknown; suggestions have included 3 months beyond attaining SUA <6.5 mg/dl,16 6 months,15 17 at least 2 months8 or “long term”.18
Evidence-based quality indicators13 and European League Against Rheumatism guidelines19 for gout care have recently been published. Compliance with quality indicators is suboptimal.3 20 Detailed population-based phase IV studies of gout medication use and laboratory monitoring in the USA are lacking.21 Few population-based studies have identified factors associated with higher uric acid surveillance,21 22 allopurinol compliance22 23 or adherence with three quality indicators20 in multivariable-adjusted analyses. To our knowledge, only one previous study has assessed predictors of inappropriate care during gout flare.4 No previous study has examined physician/patient factors associated with discontinuation of allopurinol, use of colchicine or achievement of target SUA.
We hypothesised that a large proportion of patients with gout do not receive high-quality drug treatment or SUA monitoring. In a cohort of patients with gout newly prescribed allopurinol or probenecid, we assessed: (1) the proportion receiving a new allopurinol prescription who (a) received uninterrupted allopurinol therapy, (b) received colchicine prophylaxis at allopurinol initiation, and (c) achieved a target SUA of 6 mg/dl or less; (2) patient, comorbidity and healthcare utilisation characteristics associated with quality care as defined above; and (3) the proportion in whom colchicine and probenecid doses were adjusted to renal function.
METHODS
Patient population
We identified a cohort of veterans receiving International Classification of Diseases (ICD)-9 codes for gout (274.xx) in Minneapolis Veterans Affairs (VA) Medical Center databases between 1 January 1999 and 31 December 2003 which we have reported to be valid.24 From this cohort we selected patients receiving a new allopurinol or probenecid prescription between 1 July 1999 and 30 June 2003, excluding the first and last 6 months of the study period to ensure the prescription was a new VA prescription and to allow 6 months of follow-up. Those included also had two or more VA outpatient visits/year over the study period (including the index prescription year) to ensure that VA clinics had assumed responsibility for their care.
Definitions
New long-term prescription was defined as ⩾90-day prescription with no prescription in the preceding 180 days. Colchicine or non-steroidal anti-inflammatory drug (NSAID) prophylaxis was defined as a prescription starting at least 2 weeks before a new allopurinol prescription (as in recent studies). Renal failure was defined as most recent creatinine clearance <50 ml/min or creatinine ⩾2 mg/dl (creatinine clearance was often unavailable).
Data sources
The VA databases capture all VA-dispensed medications, VA healthcare utilisation and demographic data for veterans receiving care from VA facilities. From the VA pharmacy database we extracted prescription data, including number of days’ supply, dose, number of pills and refills. From the Veterans Information System Technology Architecture (VISTA) database we obtained data on age and race of patients. From VA administrative databases we extracted all SUA levels during the study period, healthcare utilisation (inpatient admissions/year, inpatient admissions/year with gout as primary diagnosis, days/year with outpatient primary care visits, rheumatology outpatient visits/year), service connection status and percentage and means test. Service connection ranges from 0% to 100% and is awarded for conditions beginning during or as a result of active military duty. It is considered a marker for VA access, since veterans with at least 50% service connection get priority in access to VA health care. The means test is a surrogate for socioeconomic status and is categorised as follows: AN, most needy but not service connected; AS, most needy and service connected; C, not “most needy”. The Charlson Comorbidity Index,25 with higher numbers denoting more comorbid conditions, was calculated using VA databases.
Outcomes
The outcomes were chosen for patients with gout who received a new long-term prescription of allopurinol or probenecid based on randomised controlled trials, retrospective cohort studies, retrospective case series or pharmacokinetic studies from Micromedex Drugdex Evaluations (table 1).
Statistical analyses
For simple associations the Fisher exact test was used for categorical predictors or t tests for continuous predictors (using the outcome as the grouping variable). Predictors included: (1) demographic data (age and race; sex was not considered because only four patients were women); (2) healthcare utilisation (described above); (3) access to health care and socioeconomic status (percentage service connection, means test); and (4) comorbidity (Charlson Index). We then performed multivariate analysis to adjust simultaneously for predictors. To describe continuous vs intermittent allopurinol use, the dependent variable was the number of times a patient discontinued allopurinol for at least 30 days (not counting death); the analysis used Poisson regression with the log link, with offset being days the person was alive and on allopurinol. Multiple logistic regression analyses were used for colchicine prophylaxis and achieving the SUA target. Analyses used the GENMOD procedure in SAS Version 9.1 (SAS Institute, Cary, North Carolina, USA); p values <0.05 were considered statistically significant. For multivariate analyses, the results are presented with predictors remaining after a stepwise variable selection procedure that removed, one at a time, the predictor with the largest p value.
RESULTS
Of 3658 patients with a diagnosis of gout, 695 had a new allopurinol prescription lasting ⩾90 days and beginning at most 30 days before the diagnosis. Of these, 643 (93%) had two or more VA visits/year; all analyses use this group. The median initial allopurinol dose was 200 mg/day (mean 207 mg/day): 0.9% received ⩾400 mg/day, 44% received 300–399 mg/day, 13% received 200–299 mg/day, 41% received 100–199 mg/day and 1.2% received <100 mg/day.
Table 2 summarises the demographic characteristics of the cohort. The mean (SD) age was 67.9 (9.7) years (range 30.8–93.1), 639 (99%) were men, 43% were white, 1.4% were non-white and 56% were of unknown race. The mean (SD) maximum Charlson Comorbidity Index during the study period was 2.5 (2.3) (range 0–15).
A total of 135 patients had a probenecid prescription, 90 patients had 125 episodes of a probenicid prescription of ⩾90 days. The maximum dose of probenecid was 250–500 mg/day for 54 patients (43%), 1000 mg/day for 66 (53%), 1500 mg/day for 3 patients (2%) and 2000 mg/day for 2 patients (2%).
Medication use after new allopurinol prescription
Among the 643 patients starting a new allopurinol prescription, 297 (46%) had a continuous allopurinol prescription (table 3). The other 54% (346/643) discontinued allopurinol at least once. Of these, 63% (217/346) discontinued once, of whom 14% (49/346) resumed allopurinol use and were using it on 31 December 2003. A further 23% (80/346) had two episodes of allopurinol use ending in discontinuation, of whom 15 were in a third episode on 31 December 203. The remaining 14% (49/346) repeatedly discontinued and restarted allopurinol.
Only 26% (166/643) received colchicine or NSAID prophylaxis at least 2 weeks before allopurinol use; of these, 10% (66/643) received colchicine prophylaxis and 16% (100/643) received only NSAID prophylaxis (table 3); 48% (311/643) had colchicine or NSAID prophylaxis prescribed before or on the day of the index allopurinol prescription. For the 66 patients who received colchicine prophylaxis at least 2 weeks before the new allopurinol prescription, the median time from colchicine prescription to allopurinol prescription was 92 days (interquartile range 44–226). After the date of the new allopurinol prescription, the median duration of colchicine use was 260 days (interquartile range 95–521).
Besides those described above, 29% (186/643) received a colchicine prescription for a period not including the beginning of the allopurinol prescription, while 59% (377/643) received no colchicine prescription.
Laboratory monitoring and achieving target SUA after new allopurinol prescription
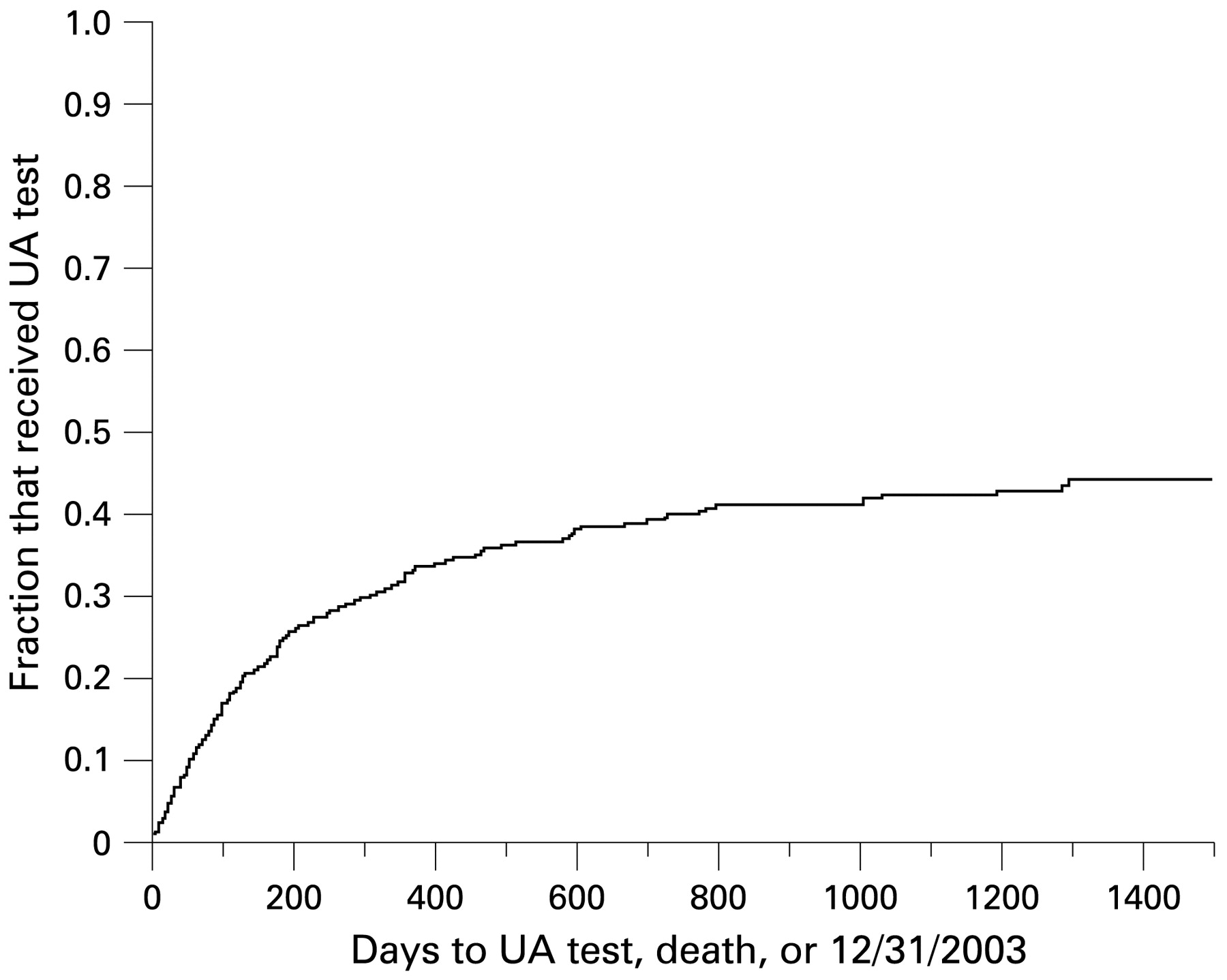
Of the 643 patients starting a new allopurinol prescription, 155 (24%) had SUA checked within 6 months, as reported previously.20 Of the remaining 488 patients, 98 (15%) had SUA checked after the recommended 6 months, 6 (1%) died during the 6-month period and 134 (20%) died after the 6-month period without having SUA checked, and 250 (39%) reached 31 December 2003 without an SUA check. Thus, excluding the 6 patients who died within 6 months of allopurinol initiation, the proportion with an SUA check changes minimally (155/637, 24%). The Kaplan-Meier curve in fig 1 shows the time to SUA monitoring after a new allopurinol prescription; only 27% of patients received SUA monitoring by 200 days and 40% by 1400 days.
{kind=link}
Kaplan-Meier plot showing time from a new allopurinol prescription to monitoring of serum uric acid (UA).
Of the 643 patients, 126 (20%) reached the target SUA, 127 (20%) had SUA checked but did not reach the target and the remaining 390 (61%) had no SUA check in the study period (table 3). Exclusion of the 22 patients diagnosed with tophaceous gout before the qualifying allopurinol prescription had little effect on these proportions.
Of the 127 patients who had a post-prescription SUA check and did not achieve the target level, 47 (37%) had at least one change in the allopurinol dose: 39 (31%) had increases, 13 (10%) had decreases and 5 (4%) had both an increase and a decrease during the study period. Some patients had more than one increase or decrease; among these 47 patients, a total of 61 dose changes occurred. Most dose changes (50/61, 82%), were made after an SUA check.
Of the 390 patients who did not receive post-prescription SUA monitoring, 92 (24%) had at least one allopurinol dose change: 59 (15%) had increases, 43 (11%) had decreases and 10 (3%) had both an increase and a decrease during the study period.
Of the 126 patients meeting the target SUA during the study period, 35 (28%) had at least one allopurinol dose change: 22 (17%) had increases, 21 (17%) had decreases and 8 (6%) had both an increase and a decrease during the study period. Most changes (41/48, 85%) occurred after an SUA check.
Association of patient characteristics with outcomes
These results are from the multivariate analyses. Allopurinol discontinuations were significantly lower for patients with more primary care or rheumatology visits (p = 0.018): an increase of 1SD in the rate of such visits (2.7 visits/year) was associated with a 12% decrease (95% confidence interval (CI) 2% to 21%) in the annual rate of discontinuations. Lack of colchicine prophylaxis was significantly less likely for patients having more days per year with outpatient visits (p<0.001) and depended on the clinic that saw the patient most frequently (p<0.001). An increase of 1SD in days per year with outpatient visits (13.6 days/year) was associated with an odds ratio of 0.48 (95% CI 0.36 to 0.65) of not receiving colchicine prophylaxis. Adjusting for the annual rate of outpatient visits, patients who were seen most frequently at a rheumatology clinic had a 66% rate of not receiving colchicine prophylaxis, while those seen most frequently at other clinics had rates of 92–94%. Failure to achieve the target SUA was significantly more likely for patients with a higher Charlson Comorbidity Index (p = 0.001) and less likely for patients with more days per year with outpatient visits (p = 0.003). An increase of 1SD in the Charlson Comorbidity Index (2.2 units) was associated with an odds ratio of 1.64 (95% CI 1.20 to 2.25) of not reaching the target, and an increase of 1SD in days per year with an outpatient visit (13.6 days/year) was associated with an odds ratio of 0.63 (95% CI 0.45 to 0.87) of not reaching the target.
Dose adjustment in patients with renal insufficiency
Probenecid
Only 55 (41%) of the 135 patients who received probenecid prescriptions had renal function checked while receiving probenecid. Twenty-one (38%) of the 55 patients had an episode of renal failure; of the total of 31 episodes, 24 (77%) ended with probenecid being discontinued while, in the remaining 7 (23%), renal function improved. The median duration of probenecid prescription during renal failure episodes was 295 days (interquartile range 209–525).
Colchicine
Fifty-two patients received colchicine and had a renal failure episode; 16 had an inappropriate dose (31%) while in 14 it was not clear whether or not the dose was inappropriate (creatinine ⩾2 mg/dl but no available creatinine clearance data). Among the 16 patients who received an inappropriate dose, 4 did so for ⩽4 days while the other 12 did so for periods ranging from 86 to 623 days.
DISCUSSION
At one VA Medical Center we found a low prevalence of quality use of allopurinol, colchicine and probenecid and SUA monitoring in patients with gout. A 54% discontinuation rate for new allopurinol prescriptions, although high, is much lower than previously reported rates of 84% in patients with newly diagnosed haematological malignancies28 and 90% in a US health maintenance organisation.22 Both earlier studies had reasonably long follow-up periods (2–3 years). Better compliance with allopurinol in our study may arise from differences in populations (gout vs gout with malignancy vs gout); age and gender (68 years and 99% men vs 42 years and 62% men vs 57 years and 76% men); institutional setting (VA referral centre vs county hospital vs health maintenance organisation);29 30 or comorbidity (Charlson score of 2.5 vs data not given vs 0.9).
An important novel finding of our study was the description of correlates of inappropriate use of allopurinol, colchicine prophylaxis and of SUA monitoring in a large cohort. Higher comorbidity was associated with a lower chance of achieving the target SUA. There are several possible explanations for this: (1) worse renal function limiting the choices of SUA-lowering therapies and the maximum dose; (2) poorer compliance with gout medication in those with multiple medical conditions and more concomitant medications; and (3) poorer absorption of gout medications due to congestive heart failure and other medical conditions. More primary care or rheumatology clinic visits had a positive protective association with allopurinol continuation, and more rheumatology clinic visits or more total outpatient visits improved the odds of receiving colchicine prophylaxis. Both of these findings suggest that rheumatologists are more likely to prescribe colchicine prophylaxis and that “more eyes on the problem” leads to better quality care, extending similar observations made for rheumatoid arthritis.31 These findings add to previous observations that shorter gout duration or physician consultations are associated with inappropriate care during flare-ups of gout.4 Potential strategies for improving colchicine/NSAID prophylaxis include physician education or system-based interventions such as pharmacy automatic ordering or physician prompts on a new allopurinol prescription.
Our study has several strengths and limitations. We studied a large cohort with a long follow-up period. All VA prescriptions and laboratory measures and various patient characteristics were available from computerised databases. Since these were predominantly Caucasian men, generalising to women or other races may be tenuous. Gout is primarily a disease of middle-aged and elderly men, so our findings may be generalised to elderly men who constitute a large proportion of patients with gout. VA electronic databases are an excellent means of studying quality of care, but cannot account for adverse effects, gout flares or physician rationale for not prescribing certain medications; however, this is unlikely to explain the non-compliance rates of 52% and 76% with the use of prophylaxis and SUA monitoring, respectively. We could not obtain non-VA prescriptions or laboratory results and some veterans may have received care from non-VA sources. Since we confined our analyses to veterans with two or more visits to a VA centre per year, the VA can reasonably be held accountable for the quality of care of these patients, regardless of care received in non-VA settings. Additionally, a random chart review found that only 3% of new colchicine users had any previous non-VA prescription, so non-VA care is unlikely to result in a significant misclassification bias. Our cohort was selected using both a new long-term allopurinol prescription and an ICD-9 code for gout which was found to be valid at our medical centre.24 Future studies should examine if income, social support, distance from the medical centre and other factors explain poor medication use patterns in patients with gout.
The reasons for frequent allopurinol discontinuation are not clear, but are of concern. Possibilities include inadequate patient and physician knowledge regarding proper allopurinol use;4 occurrence of adverse effects or incomplete information regarding adverse effects; socioeconomic factors such as income and lack of health insurance; and system barriers. The high prevalence of intermittent allopurinol use parallels compliance rates of 21–36% with heart disease medications including beta-blockers and statins.32 33
For 40 years, colchicine/NSAID prophylaxis has been recommended due to a high flare rate during the first few months of treatment with allopurinol.18 34 Recent reviews have re-emphasised this.17 35 The rate of non-compliance far exceeded our expectation. A low rate of 50% of colchicine/NSAID prophylaxis—even with the most liberal definition regarding the time of prophylaxis initiation—is a “cry for help” by patients with gout about easily avoided recurrent acute flares.
Achieving and maintaining the target SUA level (6 mg/dl) is associated with no or a low rate of gout flares.1 8 Allopurinol at 300 mg/day, regardless of body mass index, SUA or renal function, achieves the target SUA level in only 50% of patients.8 9 Many of our patients (44%) received allopurinol in a dose of 300–399 mg/day, consistent with earlier literature.12 Most of our patients (58%) had no SUA check during follow-up, which is concerning because achieving the target SUA level requires at least one measurement for dose titration. Of those who underwent a follow-up measurement, only half achieved the target SUA. This low success rate resembles national trends for glycosylated haemoglobin36 37 and lipids,38–40 and is therefore a concern. More frequent SUA monitoring will likely lead to dose titration and increased achievement and maintenance of target SUA levels.
In summary, we found low rates of quality medication use and achievement of target SUA levels and a significant variation in medication use and monitoring patterns in patients with gout. This gives great scope to improve compliance with well-established evidence-based standards. Certain patient and utilisation characteristics were associated with deviation from recommended care. These results support the need for studies to investigate patient, physician and system factors associated with practice pattern variations and their impact on quality of life. System-based changes incorporating use of specialised teams (similar to the warfarin (Coumadin) clinic model) may improve care for patients with gout.
Acknowledgments
We thank Ms Ann Emery, administrative assistant, Minneapolis VA Medical Center for her help in typing the manuscript. This was investigator-initiated research supported by VA Scholar Grant from the Center for Epidemiological and Clinical Research, Minneapolis VA Medical Center, Minneapolis, MN and a research grant from TAP Pharmaceuticals. TAP Pharmaceuticals or its representatives did not contribute to the design, conduct or data analyses or to writing, editing or approving the manuscript.
REFERENCES
Footnotes
Competing interests: None.
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.