Article Text

Abstract
Background: Rheumatoid arthritis is a chronic autoimmune inflammatory condition characterised by polyarthritis and severe change in body mass and neuroendocrine environment.
Objectives: To investigate plasma levels of adipocytokines (leptin, adiponectin, visfatin and resistin) in patients with rheumatoid arthritis and to compare them with levels in healthy controls.
Methods: Adiponectin, resistin, visfatin and leptin concentrations were measured in 31 patients with rheumatoid arthritis and 18 healthy controls by using specific enzyme-linked immunosorbent assays.
Results: Patients with rheumatoid arthritis showed considerably higher plasma levels of leptin, adiponectin and visfatin than healthy controls. No marked difference was observed in resistin levels between patients and controls.
Conclusion: A marked increase in plasma levels of leptin, adiponectin and visfatin was noted in patients with rheumatoid arthritis, whereas resistin levels were similar to those observed in healthy controls. Coordinated roles for adiponectin, leptin and visfatin are suggested in the modulation of the inflammatory environment in patients with rheumatoid arthritis, whereas the lack of modulation in resistin levels is predictive of an irrelevant role for this peptide, suggesting that resistin level is probably not one of the main signals associated with the pathogenesis of this disease.
- BMI, body mass index
- CRP, C reactive protein
- PBEP, pre-B cell colony-enhancing factor
- TNF, tumour necrosis factor
- WAT, white adipose tissue
Statistics from Altmetric.com
- BMI, body mass index
- CRP, C reactive protein
- PBEP, pre-B cell colony-enhancing factor
- TNF, tumour necrosis factor
- WAT, white adipose tissue
Chronic inflammation in rheumatoid arthritis triggers body energy adjustments that include high-energy expenditure, fat mobilisation, enhanced gluconeogenesis, protein catabolism and negative nitrogen balance. These homeostatic perturbations are believed to accelerate morbidity and mortality in patients with rheumatoid arthritis and are associated with increased production of inflammatory factors, as well as disturbances of the endocrine system. Thus, rheumatoid arthritis-associated wasting syndrome is characterised by a considerable loss of body cell mass. In addition, rheumatoid cachexia is often accompanied by increased fat mass and stable body weight. In patients with rheumatoid arthritis, all these metabolic changes lead to an apparently contradictory condition, rheumatoid cachectic obesity, which affects roughly more than 50% of all patients with rheumatoid arthritis.1 On the other hand, obesity may increase susceptibility to rheumatoid arthritis, and at present is considered to be a chronic metabolic disorder characterised by systemic low-grade inflammation, as adults who are obese and overweight have increased levels of inflammatory markers in the blood, most of them produced by the white adipose tissue (WAT).2 WAT, which is now considered to be a frank endocrine organ, produces a large number of molecules that share the functional and structural properties of cytokines and are therefore called adipocytokines. Leptin, the 16-kDa product of ob gene, is a pleiotropic hormone mainly produced by WAT.3 Leptin acts as a negative feedback signal for neurones in the central nervous system to decrease food intake and to increase energy expenditure, and the physiological importance of leptin is that low levels signal starvation.4 Leptin exerts peripheral functions, including regulation of endocrine function, reproduction and immunity.4 Several studies have shown that circulating levels of leptin increase during infection and inflammation, suggesting that leptin is part of the immune response and host defence mechanisms.4 Furthermore, leptin levels are raised during experimental inflammation5 and exert an evident pro-inflammatory effect on cultured chondrocytes by synergistically activating nitric oxide synthase II.6,7
In addition to leptin, other hormones derived from the adipose tissue, with a suggested role in the regulation of energy metabolism and insulin sensitivity, have been discovered. Recently, three hormones produced by adipose tissue have drawn major attention: adiponectin, resistin and visfatin.
Adiponectin, also called GBP-28, apM1, Acrp-30 or adipoQ, is a 244-amino acid adipose tissue-specific protein that has structural homology to collagen VIII and X and complement factor C1q.6 Plasma levels of adiponectin are inversely correlated with fat mass and are diminished in diabetes mellitus type 2 and in cardiovascular diseases. Adiponectin has antiatherogenic function and it improves insulin sensitivity and reduces circulating fatty acid concentration and triglyceride levels in muscle and in the liver.8 Moreover, adiponectin is postulated to be associated in the modulation of inflammatory responses8 as it attenuates the inflammatory response mediated by tumour necrosis factor α (TNFα), inhibits macrophage phagocytic activity and TNFα production and also inhibits myelomonocytic cell proliferation by inducing apoptosis.
Resistin is a newly discovered protein primarily produced by adipocytes. It was initially considered to be a potential link between obesity and insulin resistance.9 Later studies did not fully support this original hypothesis.8,10 Resistin belongs to the family of resistin-like molecules, also known as “found in inflammatory zone”. Levels of resistin have been reported to be either increased, unchanged or decreased in murine and human obesity and type 2 diabetes, somewhat dampening the initial enthusiasm for resistin as a possible link between adiposity and insulin resistance.8 In humans, resistin acts as a critical mediator of the insulin resistance associated with sepsis and possibly other inflammatory conditions.10,11 Finally, visfatin is a recently discovered adipokine produced and secreted primarily by visceral WAT.12 Visfatin binds to and activates the insulin receptor, exerting insulin-mimetic effects both in vitro and in vivo. Visfatin is identical to pre-B cell colony-enhancing factor (PBEF), a cytokine that is increased in the bronchoalveolar lavage fluid in animal models of acute lung injury and in neutrophils of patients with sepsis.12,13 Interestingly, the presence of specific single nucleotide polymorphisms in the visfatin or PBEF gene, which decrease the gene transcription rate, highly increase the risk of development of acute lung injury in patients with sepsis.13 PBEF or visfatin is produced by endotoxin-stimulated neutrophils and inhibits neutrophil apoptosis through a mechanism mediated by caspase 3 and caspase 8.13 Although the connection between the insulin-mimetic and anti-apoptotic effects of PBEF or visfatin still have to be investigated, this protein clearly represents an additional link between adipose tissue and inflammation.8,13
We compared plasma levels of leptin, adiponectin, visfatin and resistin in patients affected by rheumatoid arthritis with those in healthy controls.
SUBJECTS AND METHODS
Determination of leptin, adiponectin, visfatin and resistin in patients and controls
In all, 31 patients with a diagnosis of rheumatoid arthritis (mean age 46.1 (SEM 14.1) years; body mass index (BMI), 25.88 (SEM 0.63) kg/m2; male:female ratio 9:22) according to the classification criteria of the American College of Rheumatology were enrolled in the study. Of them, 22 had more than eight inflamed joints along with an increased erythrocyte sedimentation rate (all patients with rheumatoid arthritis have erythrocyte sedimentation rate >20 mm at the end of first hour) and C reactive protein (CRP mean 0.61 (SEM 0.19) mg/dl). In all, 28 (81%) patients were being treated with methotrexate, 23 (62%) with low doses of prednisone (<10 mg daily) and 9 (26%) with TNF antagonists.
Eighteen healthy people of similar sex and age (mean 48.3 (SEM 16.1) years; BMI 24.36 (SEM 0.83) kg/m2; male:female ratio 8:10) were used as controls. Informed consent was obtained from patients and controls according to the Declaration of Helsinki; the Galician Ethical Committee of Clinical Investigation approved the design of the work. In all the participants, blood was collected in Vacutainer tubes containing EDTA between 09:00 and 11:00 after overnight fasting.
Leptin, adiponectin and resistin levels in plasma were determined by a specific enzyme-linked immunosorbent assay using materials and protocols supplied by the provider (LINCO Research, St Charles, Missouri, USA). Visfatin level in plasma was determined by the enzyme immunoassay kit purchased by Phoenix Pharmaceuticals (Belmont, California, USA).
Statistical analysis
Data were expressed as means (SEM) and analysed with a computer package for statistical analysis (Instat-Graphpad Software, Inc., San Diego, California, USA). Statistically significant differences were determined by Mann–Whitney non-parametric signed rank test. Values of p<0.05 were considered to be significant. Correlation was calculated by Spearman’s non-parametric test, and the relationship between plasma adipocytokine levels and CRP was analysed by linear regression.
RESULTS
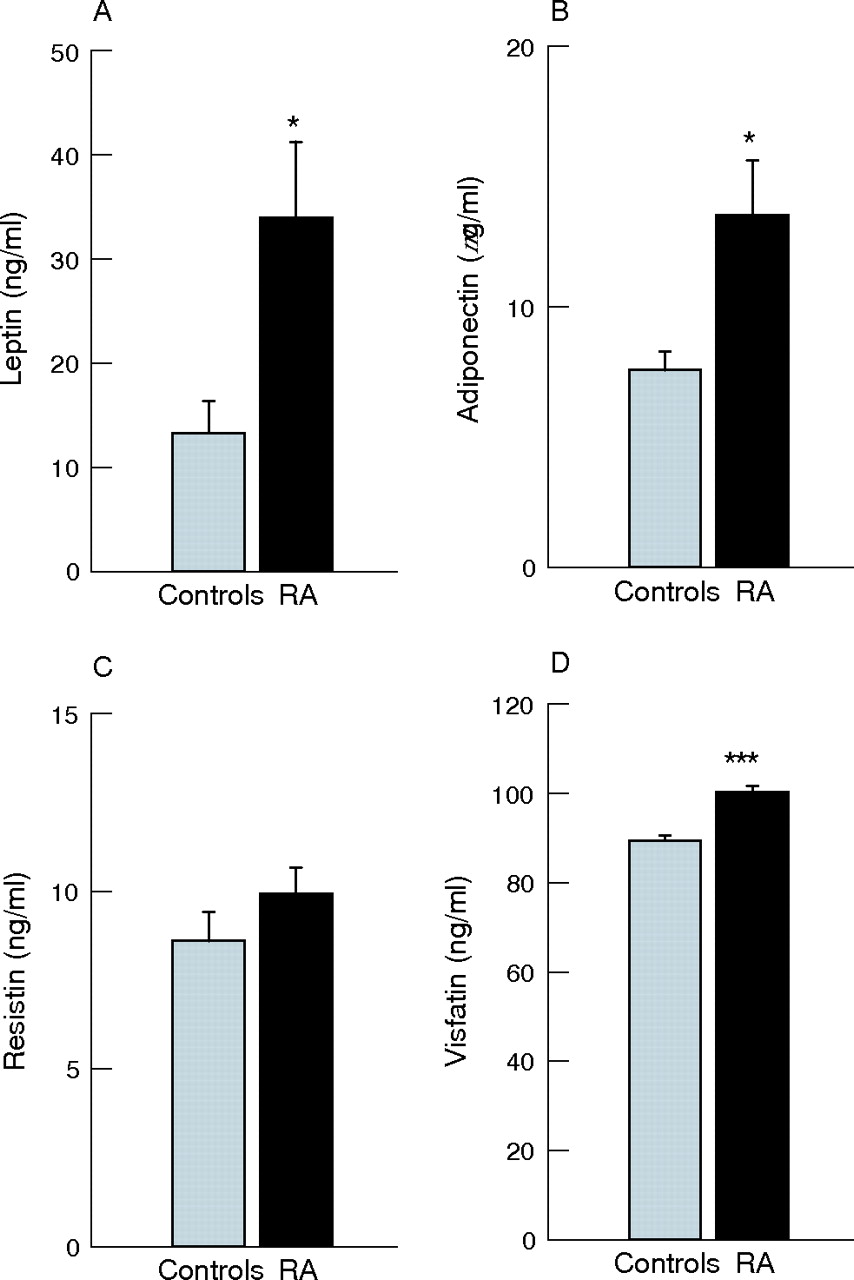
Patients with rheumatoid arthritis showed significantly higher concentrations of leptin (mean 33.9 (SEM 7.3) ng/ml v controls, mean 13.3 (SEM 3.04) ng/ml; p = 0.0144), adiponectin (mean 13.56 (SEM 2.1) μg/ml v controls, mean 7.6 (SEM 0.7) μg/ml; p = 0.0375) and visfatin (mean 100.35 (SEM 1.2) ng/ml v controls, mean 89.56 (SEM 1.1) ng/ml; p<0.001) in plasma than controls. We observed no marked difference in resistin levels between patients with rheumatoid arthritis and controls (mean 9.956 (SEM 0.7) ng/ml v controls, mean 8.62 (SEM 0.8) ng/ml) (fig 1). Furthermore, we analysed the relationship between adipocytokine and CRP levels in patients with rheumatoid arthritis and found that CRP levels significantly correlated with leptin (r = 0.71, p = 0.0079), adiponectin (r = 0.59, p = 0.031) and visfatin (r = 0.63, p = 0.043). We, however, failed to show any significant correlation between resistin and CRP levels in patients with rheumatoid arthritis (r = 0.15, not significant).
{kind=link}
Adipocytokine levels in plasma of patients with rheumatoid arthritis (RA) and in healthy controls. Plasma levels of (A) leptin (ng/ml), (B) adiponectin (μg/ml) (*p<0.05), (C) resistin (ng/ml) and (D) visfatin (ng/ml) (***p<0.001).
DISCUSSION
Although not completely proved, the current working hypothesis is that adipokines, cytokines and other factors produced and released by WAT are responsible for a chronic subclinic pro-inflammatory state. The ultimate reason for increased production of anti-inflammatory or pro-inflammatory factors by WAT has not been identified, however. Changes in levels of systemic adipokine, local adipokine or both have been reported in a variety of inflammatory autoimmune conditions, with most studies focusing on leptin. It has been shown that leptin-deficient mice have reduced inflammation in models of rheumatoid arthritis,4 although the opposite results were obtained when septic arthritis was studied.4 In patients with rheumatoid arthritis, leptin levels in serum remain normally correlated with BMI rather than disease stage, although our results clearly indicate that, independently of BMI, plasma levels of leptin increase markedly in patients with rheumatoid arthritis compared with controls. Popa et al14 suggested that chronic inflammation may lower leptin level in plasma. They, however, failed to show any marked difference in circulating leptin levels between patients with rheumatoid arthritis and controls, and the lack of an effect of anti-TNF treatment on leptin levels despite a considerable decrease of inflammation parameters. On the other hand, our result is in line with earlier studies recently reviewed by Otero et al4 and in agreement with a previous published observation from our group, which showed lower ghrelin levels in patients with rheumatoid arthritis than in controls. In this work,15 we hypothesised that low ghrelin levels can reflect the presence of inhibitory anorexigenic signals probably exerted by leptin, and the present result shows that our hypothesis may be correct.
An unexpected finding of this study was that patients with rheumatoid arthritis had considerably higher adiponectin levels than controls, the reasons for which are not evident, although increased levels of adiponectin are observed in the synovial fluid of these patients compared with those seen in patients with osteoarthritis.16 The increased levels of adiponectin in patients with rheumatoid arthritis suggests a compensatory mechanism under catabolic or anabolic imbalance. So, it is conceivable that an increase in adiponectin level represents an attempt to antagonise the anorexigenic and well-known pro-inflammatory effect of leptin, suggesting that these two adipokines may act in parallel as opposing metabolic counterparts. In addition, as adiponectin may be an important selectively controlled modulator of inflammatory response in patients with rheumatoid arthritis, it can be speculated that it may have a role in modulating the inflammatory response by inhibiting the expression of adhesion molecules on endothelial cells, suppressing macrophage function and inhibiting NFκB signalling, as reviewed by Fantuzzi.8 It is also believed that adiponectin has anti-inflammatory properties and can counteract the pro-inflammatory effects of TNFα, a pro-inflammatory cytokine, which may influence the production of IL6 and CRP in rheumatoid arthritis.8 The putative anti-inflammatory role of adiponectin in this scenario is worthy of further evaluation.
Visfatin, the newest adipokine discovered, simultaneously facilitates adipogenesis and has insulin-mimetic properties.12,13 It is currently unclear what would be its physiological role or relevance in the context of rheumatoid arthritis. Visfatin, according to our results, may be part of a compensatory mechanism that facilitates the accumulation of fat in the intra-abdominal depot, a feedback mechanism preventing the deleterious effects of the rheumatoid cachexia. Moreover, at present we cannot rule out that an increase in visfatin levels may be related to the modulation of inflammatory or immune response or may simply be an epiphenomenon. Finally, resistin, apart from its putative role in insulin resistance, has been recently proposed as a new pro-inflammatory adipokine. Notwithstanding, we have observed that resistin levels in patients with rheumatoid arthritis are unmodified in comparison to controls. This result is identical to that reported by other authors17 supporting our hypothesis that it is probably not one of the main signals in the pathogenesis of this disease.
It is increasingly evident that adipose tissue secretes a large variety of highly active proteins including cytokines, chemokines and hormone-like factors, such as leptin, adiponectin, resistin and visfatin, suggesting that WAT is an active player, and not simply a bystander, in the modulation of inflammatory immune response. A general consensus exists that increased adiposity is associated with augmentation of mortality in the Western population. Paradoxically, a recent report by Escalante et al18 showed an inverse relationship between body mass and mortality in patients with rheumatoid arthritis. Indeed, patients who are underweight are at increased risk of dying, whereas a higher BMI seems to diminish death risk, confirming the hypothesis that wasting phenomena in patients with rheumatoid arthritis are detrimental. On the other hand, and curiously, several investigators have reported that clinical improvement of patients with rheumatoid arthritis, from participating in therapeutic diet intervention studies, has been accompanied by a loss of body weight. At any rate, the efficacy of weight reduction strategies that include prolonged reduction of energy intake have little, if any, influence on inflammation in rheumatoid arthritis.19 Perhaps, the potential suppressive effect of a low-energy diet and starvation is not surprising with regard to what is already known from research on leptin physiology. Indeed, starvation is characterised by low leptin levels. So, the improvements of symptoms in energy-restricted patients with rheumatoid arthritis may be related to a marked decrease in circulating levels of leptin. In conclusion, patients with rheumatoid arthritis have a marked increase in plasma levels of leptin, adiponectin and visfatin, whereas resistin levels are unmodified. These data confirm a relevant role for adipokines produced by WAT in the metabolic changes of autoimmune articular diseases such as rheumatoid arthritis and suggest important therapeutic implications that need further exploration.
Acknowledgments
The research described in this article has been supported by the Spanish Ministry of Health, Fondo de Investigación Sanitaria, Instituto de Salud Carlos III (FIS PI 05/0525, PI030115, PI050419 and G03/152), and Xunta de Galicia. OG is a recipient of a research contract co-funded by SERGAS and Instituto de Salud Carlos III (Exp 00/3051); FL is a recipient of a contract under the "Programme of Stabilization of Researchers" co-funded by the Instituto de Salud Carlos III and SERGAS (BOE n°23 27/01/2006). MO is a recipient of a postdoctoral fellowship funded by Caixa Galicia Fundation, his present address is: Beth Israel Deaconess Medical Center, New England Baptist Bone & Joint Institute, Harvard Institutes of Medicine, Boston MA, USA. RL is a recipient of a predoctoral fellowship funded by the Instituto de Salud Carlos III. RG is a recipient of a project-associated fellowship from the Instituto de Salud Carlos III (FIS 05/0525).
REFERENCES
Footnotes
-
Published Online First 13 January 2006
-
Competing interests: None.