Article Text

Abstract
Objective: Infliximab is effective in improving signs and symptoms of joint/skin involvement, functional status, and quality of life in patients with psoriatic arthritis (PsA). Using IMPACT trial data, we assessed the effect of infliximab (IFX) on structural damage in PsA.
Methods: Patients with active PsA were randomly assigned to receive placebo (PBO/IFX) or infliximab 5 mg/kg (IFX/IFX) at weeks 0, 2, 6, and 14, with the primary endpoint at week 16. The PBO group received infliximab loading doses at weeks 16, 18, and 22. Thereafter, all patients received infliximab 5 mg/kg every 8 weeks through week 50. Hand/feet radiographs were obtained at weeks 0 and 50. Total radiographic scores were determined using the PsA modified van der Heijde-Sharp (vdH-S) score. Projected annual rate of progression was calculated by dividing x ray score by disease duration (years).
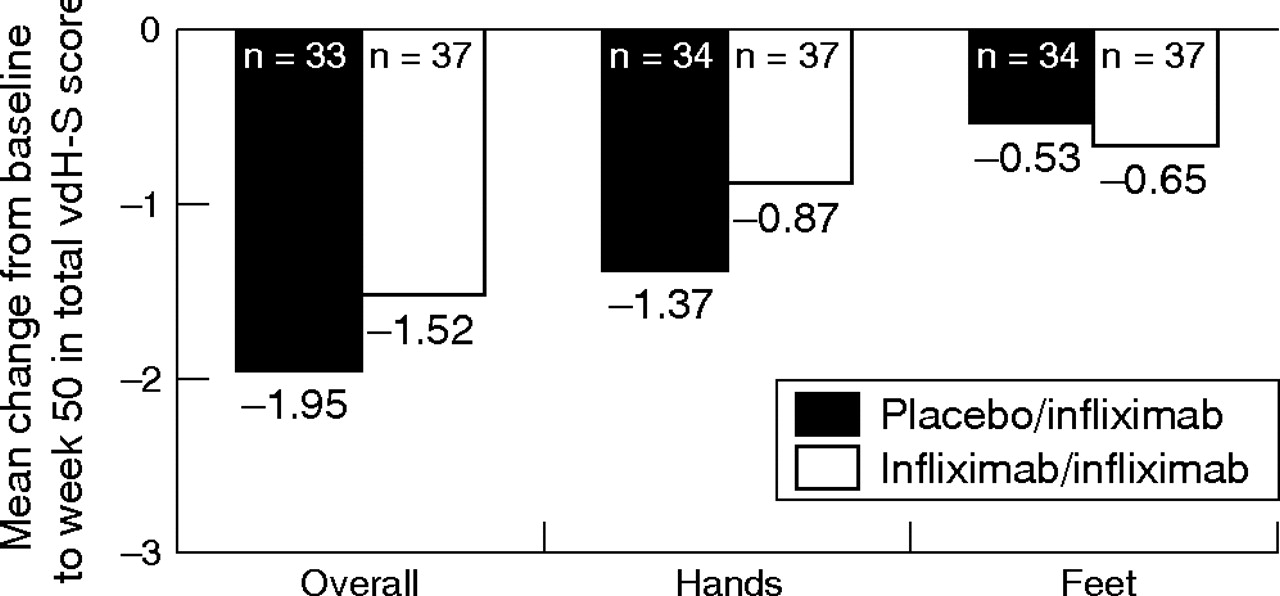
Results: As reported previously, 65% of infliximab treated patients versus 10% of PBO treated patients achieved an ACR20 response at week 16 (p<0.001). At week 50, 69% of patients achieved an ACR20 response. Radiographs (baseline and week 50) were available for 72/104 patients. At baseline, estimated mean annual rate of progression was 5.8 modified vdH-S points/year. Mean (median) changes from baseline to week 50 in the total modified vdH-S score were −1.95 (−0.50) for PBO/IFX and −1.52 (−0.50) for IFX/IFX patients (p = NS). At week 50, 85% and 84% of patients in the PBO/IFX and IFX/IFX groups had no worsening in the total modified vdH-S score.
Conclusion: Infliximab inhibits radiographic progression in patients with PsA through week 50.
- CRP, C-reactive protein
- DIP, distal interphalangeal
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- IFX, infliximab
- IMPACT, Infliximab Multinational Psoriatic Arthritis Controlled Trial
- JSN, joint space narrowing
- MTX, methotrexate
- PBO, placebo
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- SDD, smallest detectable difference
- TNFα, tumour necrosis factor alpha
- vdH-S score, van der Heijde-Sharp score
- infliximab
- psoriasis
- psoriatic arthritis
- structural damage
- tumour necrosis factor α
Statistics from Altmetric.com
- CRP, C-reactive protein
- DIP, distal interphalangeal
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- IFX, infliximab
- IMPACT, Infliximab Multinational Psoriatic Arthritis Controlled Trial
- JSN, joint space narrowing
- MTX, methotrexate
- PBO, placebo
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- SDD, smallest detectable difference
- TNFα, tumour necrosis factor alpha
- vdH-S score, van der Heijde-Sharp score
Psorioatic arthritis (PsA) is a chronic inflammatory arthropathy characterised by the association of arthritis and psoriasis. While it was initially thought to be a mild, non-progressive disease when compared to rheumatoid arthritis (RA), it is now known that a substantial proportion of patients with PsA have persistent inflammation. Moreover, many patients develop progressive joint damage and disability, and have reduced life expectancy.1 It is also now known that the extent of radiological damage is more frequent than initially reported in PsA,2 in that the extent of radiographic progression in patients with established PsA is comparable with that of RA patients matched for age, sex, and disease duration.3 Treatment of PsA remains largely empirical, and in the majority of cases the rationale for use of a particular modality has come from extrapolation of efficacy in RA. Similar associations have been made for measures of disease activity.
Recent evidence has suggested that activated T cells and proinflammatory cytokines, in particular tumour necrosis factor alpha (TNFα), serve an important etiopathogenic role in PsA.4–7 As a result, biologic agents targeting TNF have been evaluated in the treatment of PsA. In published reports, both etanercept, a dimeric p75 TNF receptor (CD120b)/Ig Fc-fusion protein, and infliximab, a chimeric monoclonal antibody specific for TNFα, have been shown to be effective in treating PsA.8,9,10 Recently, in the Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT), therapy with infliximab 5 mg/kg was shown to significantly improve both the signs and symptoms of arthritis, as well as skin psoriasis, in patients with active PsA resistant to prior disease modifying antirheumatic drug (DMARD) therapy. Benefits were sustained through 50 weeks with continued infliximab treatment.11
Based on the current understanding of the immunopathogenesis of PsA, radiological damage is thought to represent a sequela of uncontrolled inflammation. As such, radiological assessment is a useful measure to gauge treatment outcome over time in PsA.3 In an evaluation of 205 patients with PsA receiving treatment with etanercept, radiographic assessment of hands and wrists was utilised. Study findings indicated etanercept was superior to placebo in inhibiting disease progression at 12 months.12
While the combination of infliximab plus methotrexate (MTX) has been shown to inhibit progressive joint damage in a majority of patients with RA who have an incomplete response to MTX alone,13 much less is known about progressive joint damage in PsA relative to RA. Therefore, we conducted an analysis of radiographs obtained in patients from the IMPACT trial to assess the effect of infliximab on the progression of structural damage in PsA.
METHODS
Patients
The details of the IMPACT study have been previously published. In summary, 104 adult patients with an established diagnosis of PsA of 6 month duration or longer were recruited into the study.11 To be eligible, patients had to have previously failed treatment with one or more DMARDs. At enrolment, patients were required to have active peripheral polyarticular arthritis, defined as the presence of five or more swollen joints of 66 evaluated joints and five or more tender joints of 68 evaluated joints in conjunction with at least one of the following: erythrocyte sedimentation rate (ESR) ⩾28 mm/h, C-reactive protein (CRP) ⩾15 mg/l, and/or morning stiffness lasting at least 45 min. Patients also were required to have negative results on serum testing for rheumatoid factor.
This investigator initiated study was conducted at nine centres in Europe, the United States, and Canada. Institutional Review Boards at each of the participating sites approved the protocol. All patients provided written informed consent prior to the performance of any study related activities.
Study design
This was an investigator initiated, multimember, randomised clinical study with a 16 week, double blind, placebo controlled treatment phase with infliximab (stage I) and a blinded treatment portion (stage II) through week 50. In addition, a protocol amendment allowed patients to enter a long term extension through week 98. In this manuscript, we report findings from a study of a cohort of 72 patients with evaluable radiographs to assess the effect of infliximab on the progression of structural damage through the first 50 weeks of open label infliximab treatment. In this phase II trial, no attempt was made to impute for missing data.
In stage I, patients were randomly assigned to receive placebo (n = 52; group I or PBO/IFX group) or infliximab 5 mg/kg (n = 52; group II or IFX/IFX group) at weeks 0, 2, 6, and 14. At the start of stage II, to preserve the blinded condition, patients in the placebo group received infliximab 5 mg/kg at weeks 16, 18, 22, 30, 38, and 46, while those in the infliximab group received placebo at weeks 16 and 18, followed by infliximab 5 mg/kg at weeks 22, 30, 38, and 46. This infusion scheme allowed open label treatment during stage II for all patients without unblinding the treatment assignments from stage I. Although all patients received infliximab in stage II, they remained blinded to the stage I treatment assignment.
The study was designed by the lead investigators (AK and CA) in consultation with the other study investigators and representatives from Centocor and Schering-Plough. Radiographic study data were collected by the investigators at each study site and analysed by Centocor personnel. The lead investigators wrote the manuscript in collaboration with the other study investigators and assistance from Centocor.
Study agent
Infliximab (Remicade; Centocor, Malvern, PA) was supplied in 20 ml vials containing 100 mg of the lyophilised concentrate; placebo was identically formulated. The infusion solution was administered by blinded investigators using an infusion set with an in-line, sterile, non-pyrogenic, low protein binding filter (pore size of 1.2 μm) through a peripheral venous access site over 2 h.
Concomitant medications
Patients were allowed, but not required, to receive concomitant therapy with one of the following DMARDs: MTX (at a dose of 15 mg/week or more, with concurrent folic acid supplementation), leflunomide, sulfasalazine, hydroxychloroquine, intramuscular gold, penicillamine, and azathioprine. For patients receiving a DMARD at enrolment, it was required that the dose be stable for at least 4 weeks prior to randomisation and remain at that stable dose throughout the study.
Concomitant therapy with oral corticosteroids (10 mg prednisone equivalent/day or less) and non-steroidal anti-inflammatory drugs was permitted, provided doses were stable for 2 weeks or more prior to screening; doses were required to remain stable throughout the study. Use of cyclosporine, tacrolimus, or intramuscular or intravenous corticosteroids was prohibited within 4 weeks of screening and during the study. Eligible patients could not have received any investigational drug within 3 months of screening or any previous treatment with a monoclonal antibody or fusion protein.
Radiographic evaluations
Radiographs of the hands and feet were obtained at baseline and at week 50. Original films were sent to Bio-Imaging Technologies for digitisation. Digitised images for each patient were stored as a set (baseline and week 50) in a random and blinded manner. Two central independent radiograph readers, both blinded to treatment arm and radiograph sequence, analysed the digitised images. Bone erosion, joint space narrowing (JSN), and total radiographic scores were determined using a PsA modified van der Heijde-Sharp (vdH-S) scoring method14 that included the second through fifth distal interphalangeal (DIP) joints of each hand. Erosions (0–5 in the hands and 1–10 in the feet) and JSN (0–4) were graded separately in six wrist joints, all metacarpal phalangeal, proximal interphalangeal, and DIP joints of each hand, and the first interphalangeal joint and all metatarsal phalangeal joints for each foot. For JSN, a score of 1 represented focal narrowing, a score of 2 joint space loss less than 50%, a score of 3 joint space loss more than 50%, and a score of 4 complete joint space loss or ankylosis.15 The total radiographic score (hands and feet combined) ranged from 0 to 528, with higher scores indicating more articular damage. Radiographic progression at week 50 was defined as a change from baseline in the modified vdH-S score that was greater than the smallest detectable difference (SDD) based on the limits of agreement.16 The SDD was 7.64. No radiographic worsening at week 50 was defined as a change from baseline in the modified vdH-S score that was 0.5 or less.
Statistical methods
To assess the difference between immediate and 4 month delayed infliximab treatment in preventing structural damage, the change from baseline in the total modified vdH-S score for hands and feet at week 50 was compared between treatment groups using analysis of variance based on the van der Waerden normal score. Positive changes from baseline indicate progression of structural damage in the joints of the hands and feet at week 50 compared with that observed at baseline.
Changes from baseline to week 50 in the erosion score and JSN, that is, the individual components of the total radiographic score, were compared between treatment groups to evaluate the effect of treatment on different aspects of disease progression. In addition, changes from baseline to week 50 in the total modified vdH-S score were compared between treatment groups by hands and feet separately to evaluate treatment effect on these different locations.
The annual estimated progression rate of radiographic damage with 1 year of infliximab treatment was calculated by dividing the change from weeks 0 to 50 in the modified vdH-S score for the infliximab group by 50 (weeks of follow up) and multiplying by 52 (weeks in a year). The annual progression rate of radiographic damage prior to infliximab treatment was calculated by dividing the modified vdH-S score at week 0 for both treatment groups by PsA symptom duration (years) under the assumption that the modified vdH-S score at the time of PsA symptom onset was 0. The annual progression rate of radiographic damage was analysed using 95% confidence intervals based on Tukey’s method.
Two additional radiographic endpoints, that is, proportions of patients with radiographic progression and proportions of patients with no radiographic worsening at week 50, were compared between treatment groups using the χ2 test. Data for all but one randomised patient (with both baseline and week 50 data) were included in these analyses. Data for one patient in the PBO/IFX group were excluded from the analysis due to inconsistent scoring by the readers, attributed to the poor technical quality of the foot films for this patient (smaller than regular size). Joints with surgery/joint replacement at baseline were considered unevaluable for erosion and JSN; if surgery/joint replacement was noted at a follow-up visit, the joint was considered as having the worst score for erosion and JSN. If a joint had subluxation/superimposition, osteoarthritis or other arthritis, or was radiographically inadequate at baseline and/or a follow-up visit, the joint was considered unevaluable for erosion and JSN for that visit. If a joint was unevaluable at baseline for a given reader, it was considered unevaluable during the study for that reader and overruled the actual joint assessment. A variance components model was used to estimate intraclass correlation to assess agreement between the two radiograph readers.
RESULTS
Baseline characteristics and patient disposition
The disposition of the overall study population has been described elsewhere.11 Of the 104 randomised patients, 72 patients were included in the analysis of radiographic data: 35 in the PBO/IFX group and 37 in the IFX/IFX group. Reasons for patient exclusion from the radiographic analysis are presented in fig 1. Baseline disease characteristics were similar between treatment groups, both in the overall study population and in the subset of patients with evaluable radiographs, with the exception of baseline MTX use in the patients with evaluable radiographs (71% of patients in the PBO/IFX group versus 38% of patients in the IFX/IFX group; p = 0.009). The numerical differences between treatment groups in the baseline radiographic scores were statistically significant (p = 0.02), with less baseline damage in the group starting with placebo treatment. In addition, baseline characteristics were consistent between the overall study population and the subset of patients with evaluable radiographs (table 1).
Baseline disease activity by treatment group

Patient disposition and evaluability.
ACR20 response
As reported, 65% of all infliximab treated patients compared with 10% of placebo treated patients achieved an ACR20 response at week 16 (p<0.001).11 At week 50, 69% of all infliximab treated patients achieved an ACR20 response. Response rates by treatment group were 68% (34/50) in the PBO/IFX group and 69% (34/49) in the IFX/IFX group.
Radiographic progression
The intraclass correlations of modified vdH-S scores at baseline and week 50 were estimated to be 0.93. The values close to 1 are caused by large subject variability in the modified vdH-S score relative to variability from all other sources. This may reflect the heterogeneous nature of the population, and indicates that the modified vdH-S score was a good measurement to differentiate individual subject’s radiographic damage in this population. Weighted κ statistics estimating inter-reader correlation of individual joints for foot JSN at baseline (0.79) and week 50 (0.76), foot erosions at baseline (0.71) and week 50 (0.70), hand JSN at baseline (0.69) and week 50 (0.55), and hand erosions at baseline (0.53) and week 50 (0.54) indicated consistency between readers. For the vast majority of radiographs, discrepancies between readers were small.
Total modified vdH-S score
Mean changes from baseline to week 50 in the total modified vdH-S score for the hands and feet combined, hands, and feet were similar for the two treatment groups (p = 0.844, 0.466, and 0.902, respectively; fig 2). Overall, mean (±SD) changes in the total modified vdH-S score from baseline to week 50 were −1.72±5.82, −1.11±4.87, and −0.59±1.99 for the hands and feet combined, hands, and feet, respectively.
Mean change from baseline to week 50 in the total modified vdH-S score.
Erosion scores
Mean changes from baseline to week 50 in the erosion score for the hands and feet combined, hands, and feet were similar for the two treatment groups (p = 0.780, 0.921, and 0.536, respectively; fig 3). Overall, mean (±SD) changes in the erosion score from baseline to week 50 were −1.22±4.46, −0.81±3.40, and −0.43±1.81 for the hands and feet combined, hands, and feet, respectively.

Mean change from baseline to week 50 in the erosion score.
JSN scores
Mean changes from baseline to week 50 in the JSN score for the hands and feet combined and hands were similar for the two treatment groups (p = 0.211 and 0.391, respectively; fig 4). A significant difference between the treatment groups was observed for the change in JSN in the feet over 1 year, with patients in the PBO/IFX group showing less reduction in mean radiographic progression in the feet (0.03±0.54) than those in the IFX/IFX group (−0.35±0.86; p = 0.016). Overall, mean (±SD) changes in the JSN score from baseline to week 50 were −0.51±1.99, −0.30±1.83, and −0.17±0.75 for the hands and feet combined, hands, and feet, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean change from baseline to week 50 in the JSN score. The difference between the treatment groups was statistically significant (p<0.05) for erosion score in the feet.
No worsening in modified vdH-S score over 1 year
The treatment groups were similar with regard to no worsening in radiographic progression, defined as a change from baseline in the modified vdH-S score that was 0.5 or less. The majority of patients had no worsening in radiographic progression at week 50 based on the total modified vdH-S score (59 patients, 84.3% overall; 28, 84.8%, in PBO/IFX group and 31, 83.8%, in IFX/IFX group; p = 0.903), erosion score (61 patients, 87.1% overall; 30, 90.9%, in PBO/IFX and 31, 83.8%, in IFX/IFX; p = 0.374), or JSN score (63 patients, 90.0% overall; 28, 84.8%, in PBO/IFX and 35, 94.6%, in IFX/IFX; p = 0.175).
Annual progression
The mean annual progression rate at baseline was 3.8 modified vdH-S points per year in the PBO/IFX group and 7.7 modified vdH-S points per year in the IFX/IFX group, equivalent to 5.8 modified vdH-S points per year for the overall study population. Following treatment, the overall mean annual x ray progression rate over the course of the trial was −1.79 modified vdH-S points per year. The mean annual rates of progression following infliximab therapy by treatment group were −2.03 modified vdH-S points per year in the PBO/IFX group and −1.58 modified vdH-S points per year in the IFX/IFX group. Comparison of the median annual progression rates between treatment groups (−0.52 modified vdH-S points per year for both groups) indicated no significant difference (p = 0.84).
Sensitivity of findings
We tested the sensitivities of our findings on covariates of interest using rank analyses of covariance with each of the following variables included as the covariate: baseline CRP level, week 50 CRP level, baseline MTX use, baseline total vdH-S score, baseline itemised radiographic score, baseline Health Assessment Questionnaire, and baseline patient assessment of pain (visual analogue scale). Results of these analyses showed that the conclusions based on total vdH-S score, erosion scores, and JSN scores remain valid, indicating our study findings are robust.
DISCUSSION
The natural course of PsA progression in a population appears to be broad, ranging from mild to severe. It is now known that joint damage among patients with PsA may be more severe than previously thought.17 Thus, it has been shown that the severity of radiological changes in the hands and feet of patients with PsA may be comparable to that of patients with RA. Although some radiographic features of PsA are very characteristic and differ from those observed in RA, especially in terms of the distribution of affected joints and the presence of destructive changes and bone proliferation at the same time,18 PsA potentially has the same overall progressive course of destruction as RA. Therapies capable of inhibiting the progression of joint damage could be valuable, for example, by preserving function over time.
The results of our analysis of the IMPACT trial data indicate a potential for change in the structural damage aspect of PsA with infliximab therapy. Overall, the estimated annual x ray progression rate, assuming such progression is linear in patients with PsA, was reduced by infliximab from a predicted rate of 5.8 modified vdH-S points per year to −1.79, indicating progression of structural damage as measured by radiographic assessment was halted.
Most scoring methods for the assessment of joint damage were developed for use in patients with RA. The most commonly used of these methods, that is, those developed by Sharp et al, and their modifications have been validated in RA.19 Although the use of such methodology has expanded to patients with PsA, similar validation exercises have not yet been conducted. Based on results from our analysis, it is encouraging that κ statistics are relatively high, indicating that two expert readers are able to consistently score the structural damage present in these PsA patients. Further work is required to validate the van der Heijde hand and foot modification of the Sharp methodology in a larger PsA population, as well as to address face validity, reproducibility, and implications for predicting further structural damage and to compare its performance with other methods that have been proposed to assess radiographic features unique to PsA.18,20 Of note, pencil-in-cup deformity and joint osteolysis were counted in our study, but the analysis did not reveal clear trends for change. Pencil-in-cup deformity is a special, not separate, case of joint osteolysis, and the pathophysiology of the two disease manifestations are likely very similar.21 Assessing the degree of progression of these radiographic findings will require additional methodology.
The results of our analysis are consistent with radiographic changes reported in an evaluation of 205 patients with PsA who participated in a randomised, blinded trial of etanercept versus placebo.12 In that trial, patients received placebo or etanercept 25 mg twice weekly in the initial 24 week blinded stage. Patients continued to receive blinded therapy in a maintenance stage until all patients completed the 24 week blinded stage. After database lock and study unblinding, all patients were eligible to receive open label etanercept in the 48 week extension. In the etanercept study, which utilised radiographic assessment (modified Sharp score) of hands and wrists only at baseline and after 24 and 48 weeks in the study, radiographic disease progression was inhibited by etanercept at 12 months, at which time the mean annualised rate of change in the total modified Sharp score was −0.03 units, compared with +1.00 units in the placebo group (p = 0.0001). In that study, baseline estimated annual rates of disease progression were 2.0 and 2.9 modified Sharp points per year, respectively, in the placebo and etanercept groups.12 In the IMPACT study presented here, which included assessment of the hands and feet by the modified vdH-S scoring method, mean annual rates of progression following infliximab therapy by treatment group were −2.03 modified vdH-S points per year in the PBO/IFX group and −1.58 modified vdH-S points per year in the IFX/IFX group. Of note, baseline estimated annual rates of radiographic progression were 3.8 and 7.7 modified vdH-S points per year, respectively, in the placebo and infliximab groups in our study. As this baseline difference was statistically significant (p = 0.02), with the infliximab treated patients having more structural damage to begin with, the study findings showing no progression following infliximab therapy are potentially even more noteworthy since these patients would be expected to have more progression. However, baseline CRP levels were higher in the PBO/IFX group than in the IFX/IFX group, and higher CRP levels are associated with more aggressive disease. While this paradox may be due to differences in prior disease management or other unknown reasons, small populations such as the one we studied are prone to natural asymmetries in baseline characteristics. Nonetheless, several factors may have contributed to the observed differences in the results. In the etanercept trial, the duration of time patients were not treated with an active agent was longer, possibly explaining the progression in the placebo group that was not seen in IMPACT. It is also worth noting that radiographic evaluations were limited to the hands in the etanercept trial, while both the hands and feet were assessed in our trial. Finally, there may be a differential effect between the treatments on radiographic progression.
The results of our analysis also indicate that treatment of the placebo group with infliximab from week 16 to week 50 inhibited x ray progression to an extent comparable to that seen with patients receiving 50 weeks of infliximab therapy. This is despite significant differences in clinical parameters at week 16 between the placebo and infliximab groups, that is, 65% of infliximab treated patients versus 10% of placebo treated patients achieved an ACR20 response (p<0.001).11 Factors potentially affecting the lack of a statistical difference between our study groups in terms of radiographic changes at week 50 may include relatively small numbers of patients and/or differences in baseline annual rates of progression between the treatment groups. We also hypothesise that the ability of patients initially treated with placebo to catch up with those who received a full year of infliximab therapy in terms of radiographic progression indicates a strong possibility for remodelling/healing in PsA. It is possible that in this regard, bony changes in PsA are more plastic than those in RA.
A tangible consequence of the results from this study relate to the optimal time at which radiographs should be obtained in clinical studies. Given the established clinical efficacy of TNF inhibitors in PsA, it is probably not ethical to withhold treatment from patients who have persistent inflammation for 6 months; some might suggest more than 4 months may be ethically tenuous.22 This study illustrates that given such design constraints, it is not practical to wait 12 months to obtain radiographs in such a situation. This concept has also been introduced in RA.23
Acknowledgments
The authors wish to thank the Medical Affairs Writing Group at Centocor, Inc., Malvern, PA and Michelle Perate, MS for their assistance in preparing this manuscript and Karen Xia for her assistance with statistical analyses.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 26 January 2006
-
This study was partially funded by Schering-Plough, Kenilworth, NJ, USA
-
Competing interests: Dr Kavanaugh has conducted research and training for Centocor for which he has been compensated. Dr Antoni has received consulting fess of less than $10 000 from Centocor and Schering-Plough and is currently an employee of Schering-Plough. Dr Gladman has received consulting fees from Centocor. Dr Furst has received research funds from Centocor. Dr Weisman has received consulting fees and research support from Centocor. Professor Smolen has received speaking fees from Centocor, Schering-Plough, Abbott, and Wyeth; research funds from Centocor; and consulting fees from Centocor, Schering-Plough, Abbott, and Wyeth. Professor van der Heijde has received speaking and consulting fees and research funds from Centocor. Professor Burmester has received funds from Centocor for conducting clinical research and serving as a consultant. Ms Zhou and Drs Beutler and G Keenan are employees of Centocor.