Article Text

Abstract
Objective: To evaluate a low field dedicated extremity MRI unit for detection of bone erosions, synovitis, and bone marrow oedema in wrist and metacarpophalangeal (MCP) joints, with a high field MRI unit as the standard reference.
Methods: In 37 patients with RA and 28 healthy controls MRI of the wrist and 2nd–5th MCP joints was performed on a low field MRI unit (0.2 T Esaote Artoscan) and a high field MRI unit (1.0 T Siemens Impact) on 2 subsequent days. MRI was performed and evaluated according to OMERACT recommendations. Additionally, conventional x ray, clinical, and biochemical examinations were performed. In an initial low field MRI “sequence selection phase”, based on a subset of 10 patients and 10 controls, sequences for comparison with high field MRI were selected.
Results: With high field, spin echo MRI considered as the reference method, the sensitivity, specificity, and accuracy of low field 3D gradient echo MRI for erosions were 94%, 93%, 94%, while the corresponding values for x ray examination were 33%, 98%, and 83%. Sensitivity, specificity, and accuracy of low field MRI for synovitis were 90%, 96%, and 94%, and for bone marrow oedema 39%, 99%, and 95%. Intraclass correlation coefficients between low field and high field scores were 0.936 (p<0.005) for bone erosions and 0.923 (p<0.05) for synovitis.
Conclusion: Low field MRI provides high accuracy for detection and grading of erosions and synovitis, with high field MRI as the standard reference. For bone marrow oedema, specificity is high, but sensitivity only moderate. Low cost, patient compliant, low field dedicated extremity MRI provides similar information on bone erosions and synovitis as expensive high field MRI units.
- FOV, field of view
- FS, fat saturated
- GE, gradient echo
- ICC, intraclass correlation coefficient
- MCP, metacarpophalangeal
- MRI, magnetic resonance imaging
- RA, rheumatoid arthritis
- SE, spin echo
- STIR, short τ inversion recovery
- TE, echo time
- TR, repetition time
- high field magnetic resonance imaging
- low field magnetic resonance imaging
- rheumatoid arthritis
Statistics from Altmetric.com
- FOV, field of view
- FS, fat saturated
- GE, gradient echo
- ICC, intraclass correlation coefficient
- MCP, metacarpophalangeal
- MRI, magnetic resonance imaging
- RA, rheumatoid arthritis
- SE, spin echo
- STIR, short τ inversion recovery
- TE, echo time
- TR, repetition time
The treatment strategy in rheumatoid arthritis (RA) has changed markedly during the past decade with emphasis on completely suppressing joint inflammation and preventing structural joint damage and functional disability as early as possible during the course of the disease.1–3 Owing to this early and extensive treatment approach, there is a growing need for sensitive and specific tools for both early diagnosis and monitoring disease activity and joint damage. Furthermore, markers of prognostic significance are also needed.
The examination modalities currently used for assessment of disease activity and structural joint damage—clinical examination, composite disease activity scores, biochemical assessment, and conventional radiography—are not sufficiently sensitive or specific, especially in early disease.4–6
In recent years new methods for diagnosing and monitoring RA have evolved. In particular, magnetic resonance imaging (MRI) is a promising tool as it offers the opportunity for an examination of all aspects of the rheumatoid joint disease, visualising both destructive and inflammatory disease manifestations.
MRI performed on high field units has in previous studies been more sensitive than conventional methods for detection of synovitis and bone changes in patients with RA.5,7,8,9,10
Low field dedicated extremity MRI units are more comfortable for the patients and less expensive, but, largely unvalidated.11–14
The objective of this study was to evaluate a low field dedicated extremity MRI unit for the detection and grading of synovitis, bone marrow oedema, and MRI erosions in wrist and metacarpophalangeal (MCP) joints, with a high field MRI unit as the standard reference, and to compare the MRI findings with the destructive joint changes seen on x ray examination.
PATIENTS AND METHODS
Thirty seven patients (13 men, 24 women) with RA, fulfilling the American College of Rheumatology 1987 revised diagnostic criteria15 and 28 healthy controls (8 men, 20 women) were enrolled in the study. All subjects were recruited from the Department of Rheumatology, Copenhagen University Hospital at Hvidovre. Local ethics committee approval was obtained before starting the studies.
Clinical and biochemical examination
All clinical examinations were performed by the same rheumatologist and included assessment of joint swelling and joint tenderness as recommended by EULAR.16 Furthermore, every person taking part in this study completed a Health Assessment Questionnaire.17 The laboratory tests covered serum C reactive protein (reflection photometry) and IgM rheumatoid factor (turbidometry). Disease Activity Scores based on 28 joint assessments were computed for all patients.18
Conventional radiography
An x ray examination of the wrists and hands was performed in the posteroanterior and oblique projections.19 All radiographs were evaluated by the same radiologist, who had no access to data and results of the MRI findings. Radiographic bone erosions were evaluated separately in each wrist bone and MCP bone quadrants.
Magnetic resonance imaging
MRI of the wrist and 2nd–5th MCP joints of the dominant hand was performed twice on two different MRI units—that is, a 1.0 T Siemens Impact high field MRI unit equipped with a circular polarised transmit-receive coil and a 0.2 T Artoscan (Esaote Biomedica) low field dedicated extremity MRI unit equipped with a dual phased array coil.
The MRI scans were performed on two subsequent days to ensure complete clearance of the intravenously injected contrast agent (0.1 mmol gadolinium-DTPA-BMA/kg body weight; Omniscan (Amersham Health)) and still allowing only minimal time for biological variations.
High field MRI
On the high field MRI unit, the following procedures were performed: the subjects were positioned prone with the hand fixed above the head in the centre of the coil (superman position). T1 weighted, spin echo (T1-SE) sequences were obtained in the coronal and axial planes before and after intravenously injected contrast medium (Omniscan). In addition, coronal short τ inversion recovery (STIR) and coronal T2 weighted, spin echo, fat saturated (T2-SE-FS) sequences were obtained in the coronal plane before the contrast agent was administered.
The imaging variables for the different MRI sequences were as follows: T1-SE images: repetition time (TR) 600 ms, echo time (TE) 15 ms, slice thickness 3 mm, field of view (FOV) 109 mm×145 mm, matrix 192×256, number of acquisitions 2, number of repetitions 1; STIR sequence: TR 4500 ms, TE 30 ms, inversion time 150 ms, slice thickness 3 mm, FOV 109 mm×145 mm, matrix 182×256, number of acquisitions 3, number of repetitions 1; T2-SE-FS sequence: TR 4500 ms, TE 96 ms, slice thickness 3 mm, FOV 109 mm×145 mm, matrix 182×256, number of acquisitions 3, number of repetitions 1.
Low field MRI
On the low field MRI unit the following procedures were performed: the subjects were seated in an adjustable chair with the dominant hand positioned in the centre of the coil in a neutral position. T1-SE sequences were obtained in the coronal and axial planes supplemented with a T1 weighted three dimensional gradient echo (T1-GE), with isometric voxels, before and after intravenously injected contrast medium (Omniscan). The gradient echo images were subsequently reconstructed with a slice thickness of 1 mm. A coronal STIR sequence was obtained before the contrast agent was administered.
The imaging parameters for the different MRI sequences were as follows: T1-SE images: TR 550 ms, TE 18 ms, slice thickness 3 mm, FOV 200 mm×200 mm, matrix 256×256, number of acquisitions 3; 3D-GE sequence: TR 30 ms, TE 12 ms, slice thickness 1 mm, FOV 140 mm×140 mm×80 mm, matrix 192×160×80, number of acquisitions 1, flip angle 65°; STIR: TR 1100 ms, TE 24 ms, inversion time 85 ms, slice thickness 3 mm, FOV 200 mm×200 mm, matrix 192×160, number of acquisitions 3, interslice gap 0.3 mm.
MRI interpretation: preliminary evaluation
To compare the sensitivity and specificity of the 3D gradient echo (recalled images) and the 2D spin echo sequence of the low field MRI unit, we initially evaluated MR images from 10 patients and 10 healthy subjects. Conventional high field MRI was considered the standard reference.
At the time of the preliminary MR image analysis there was no internationally accepted scoring system for MR images in RA, as later developed by the OMERACT MRI in RA Group.20 Accordingly, the scoring in the preliminary MR image evaluation was based on the methods used by our group in previous studies.21,22
Each image set (low field spin echo, low field gradient echo, and high field spin echo) was evaluated in a blinded setting for the presence or absence of MRI erosions and synovitis. The evaluation of bone erosions comprised separate assessment of each MCP quadrant and wrist bone, and the evaluation of synovitis covered assessment of each joint.23 In view of the results of the preliminary evaluation (see later), we chose to use the 3D-GE recalled images from the low field unit for the subsequent main MR image evaluation.
In the preliminary “sequence selection” phase, bone marrow oedema was not assessed because the low field MRI unit used only allows assessment of bone marrow oedema by the STIR sequence, while spectral fat saturation is not technically possible.
MRI interpretation: main evaluation
Each image set was evaluated separately for the presence or absence of MRI erosions, synovitis, and bone marrow oedema by an observer who was unaware of the findings by other modalities.
MRI bone erosions were evaluated separately in the metacarpal head and the phalangeal base of each MCP joint and in each wrist bone. Synovitis in MCP joints was evaluated for the whole joint, while the wrist joint was divided into three regions: the radioulnar area, the radiocarpal area, and the intercarpal-carpometacarpal area. Finally, bone marrow oedema was evaluated separately in the metacarpal head and the phalangeal base of each MCP joint and in each wrist bone. MRI bone erosions, synovitis, and bone marrow oedema were defined according to the latest OMERACT recommendations.20
Statistical analysis
Agreement was calculated as sensitivity, specificity, and accuracy. Intraobserver agreement was expressed as an intraclass correlation coefficient24 (ICC, two-way mixed effects model with absolute agreement) using the Statistical Package for the Social Sciences for Windows, version 12 (SPSS, Chicago, Illinois). For the ICC calculations, p<0.05 was considered significant.
RESULTS
Table 1 shows the characteristics of the patients.
Characteristics of patients and healthy controls
The results of the evaluations of the MR images are divided into two parts—that is, the results from the preliminary MR image evaluation and the results from the main MR image evaluation.
Results of the preliminary MR image evaluation
Below, the performance of spin echo and gradient echo imaging on the low field unit, with high field MRI as standard reference, is described.
For destructive joint changes, the sensitivity of the T1 weighted gradient echo images (T1-GE) was markedly higher than the sensitivity of the T1 weighted spin echo images (T1-SE) (table 2). This gain in sensitivity was obtained without compromising the specificity and accuracy.
Preliminary MRI evaluation*: detection of bone erosions and synovitis of low field spin echo and gradient echo MRI with high field spin echo MRI as standard reference
When synovitis was evaluated, the sensitivity was moderately higher on T1-GE images than on T1-SE images, but this was at the expense of slightly lower specificity, but not accuracy (table 2).
Based on the findings of an overall higher accuracy of the GE sequence in the preliminary study, it was decided to do all subsequent analyses—that is, the “main MRI evaluation”, based on the data obtained on the T1-GE images of the low field MRI units.
Results of the main MR image evaluation
Bone erosions on high field and low field MRI
In total 1431 wrist and MCP joint bones were evaluated for the presence of bone erosions. High field MRI detected 318 erosions and low field MRI detected 370 erosions. The mean sensitivity, specificity, accuracy, and ICCs of low field MRI for detection and grading of erosions, when high field MRI was considered the standard reference, were found to be 94%, 93%, 94% and 0.936 (p<0.005), respectively (table 3, figs 1 and 2).
Bone erosions and bone marrow oedema in wrist and MCP joint bones. Performance of low field MRI and x ray examination when high field MRI is considered as standard reference
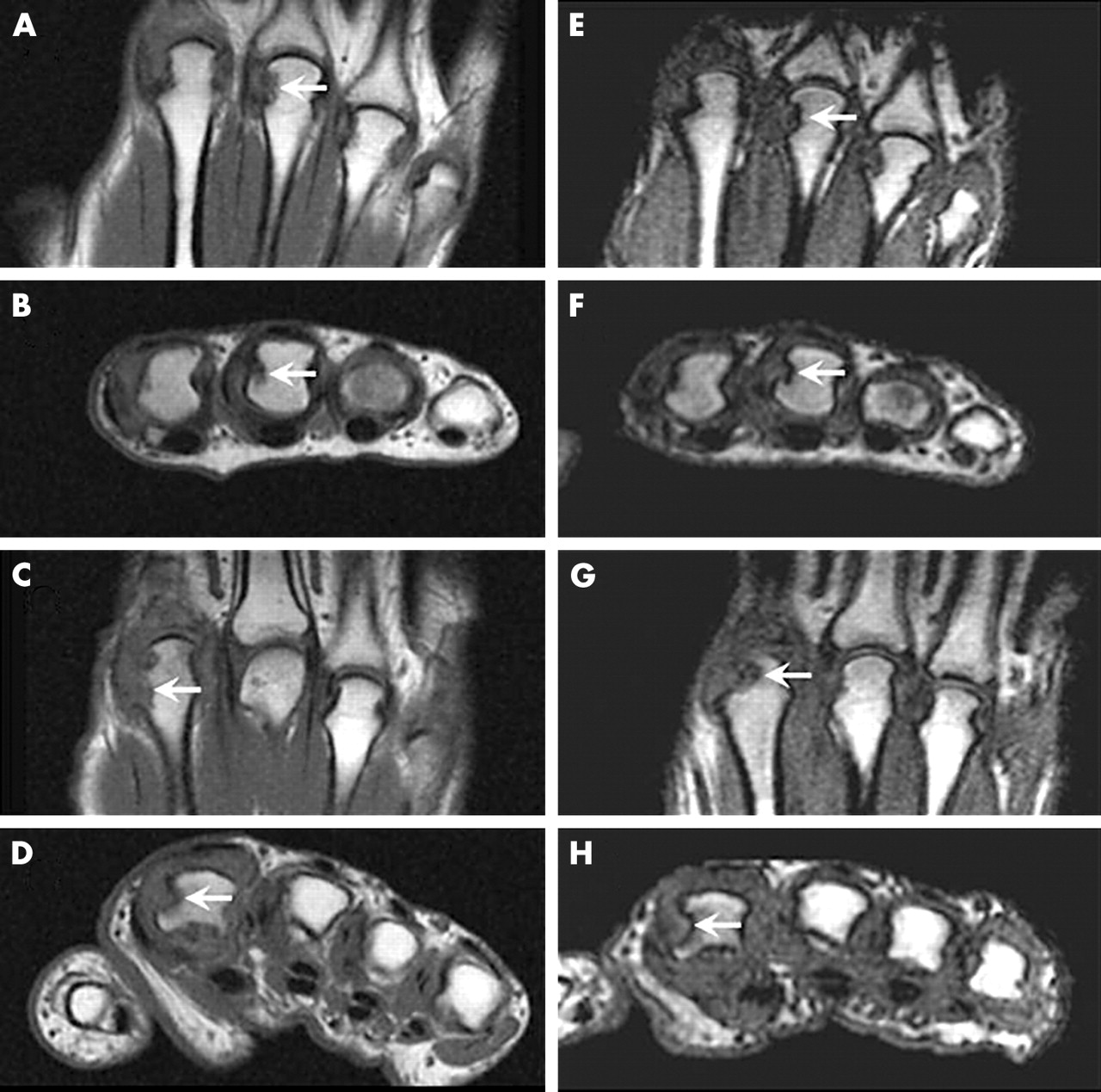
Erosions in RA MCP joint bones visualised by high field and low field MRI. High field (A, B, C, D) and low field (E, F, G, H) coronal (A, C, E, G) and axial (B, D, F, H) images of the 2nd–5th MCP joints. On high field MRI as well as low field MRI, an erosion (OMERACT grade 2) (arrows) is depicted in the 3rd metacarpal head (A, B, E, F) in patient 1 (upper four images). In patient 2 (lower four images) an erosion (OMERACT grade 3) (arrows) is depicted in the 2nd metacarpal head at both field strengths. All displayed images were obtained before contrast injection.

Erosions in RA wrist joint bones visualised by high field and low field MRI. High field (A, B, C, D) and low field (E, F, G, H) coronal (A, C, E, G) and axial (B, D, F, H) images of the wrist joints. On high field MRI as well as low field MRI, an erosion (OMERACT grade 5) (arrows) is depicted in the lunate (A, B, E, F) in patient 1 (upper four images). In patient 2 (lower four images) an erosion (OMERACT grade 1) (arrows) is depicted in radius (C, D, G, H) at both field strengths. All displayed images were obtained before contrast injection.
Bone erosions on high field MRI and x ray examination
A total of 1495 bones were evaluated by x ray examination and high field MRI for the presence of erosions. The number of erosions detected in the wrist and MCP joint bones was 123 and 318, respectively. The mean sensitivity, specificity, and accuracy of x ray examination for detection of erosions, when high field MRI was considered the standard, was 33%, 98%, and 83%, respectively (table 3).
Synovitis on high field and low field MRI
The numbers of areas with synovitis detected by high field MRI and low field MRI in the three wrist areas (distal radioulnar joint, radiocarpal joint, and the intercarpal-carpometacarpal area) and the MCP joints in all subjects were 172 and 164, respectively. The mean sensitivity, specificity, accuracy, and ICC of low field MRI for detection of synovitis, when high field MRI was considered the standard, were 90%, 96%, 94%, and 0.923 (p<0.05), respectively (table 4, figs 3 and 4).
Synovitis in wrist joint areas and MCP joints detected on high field and low field MRI. Agreement rates of low field MRI were calculated with high field MRI as standard reference
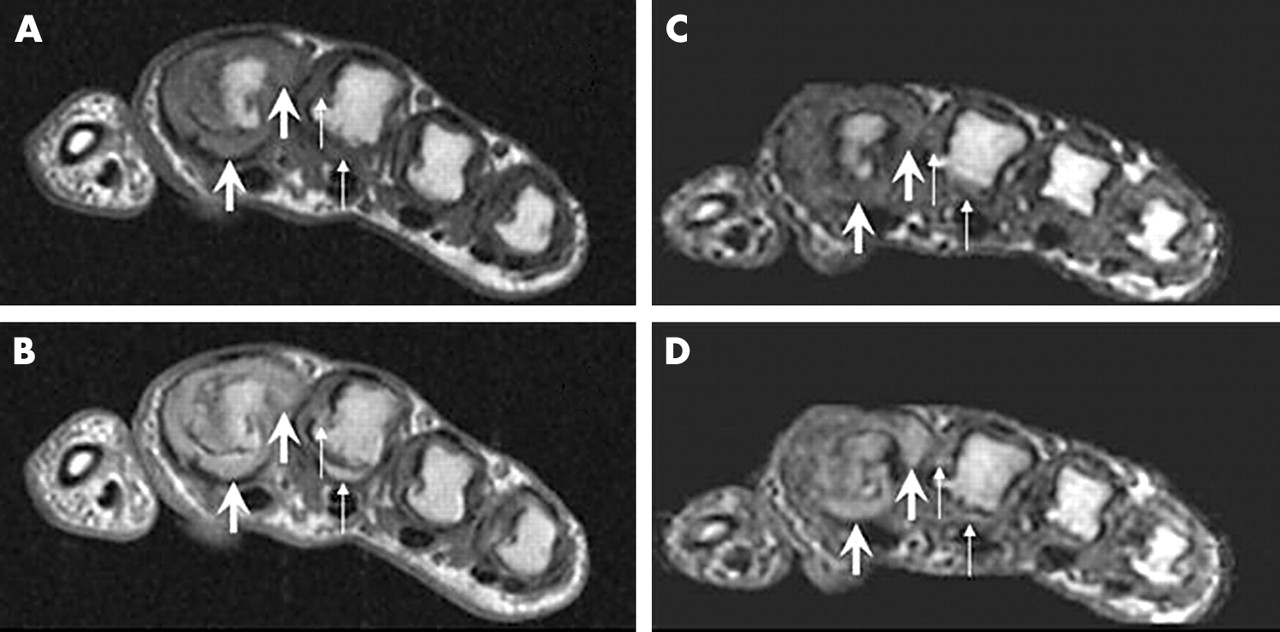
Synovitis in RA MCP joints visualised by high field and low field MRI. High field (A, B) and low field (C, D) axial images of the 2nd-5th MCP joints before (A, C) and after (B, D) intravenous contrast injection. Post-contrast images show high grade synovitis (OMERACT grade 3) (arrows) in the 2nd MCP joint on high field MRI as well as on low field MRI, while low grade synovitis (OMERACT grade 1) (thin arrows) is seen in the 3rd MCP joint on images obtained at both field strengths.

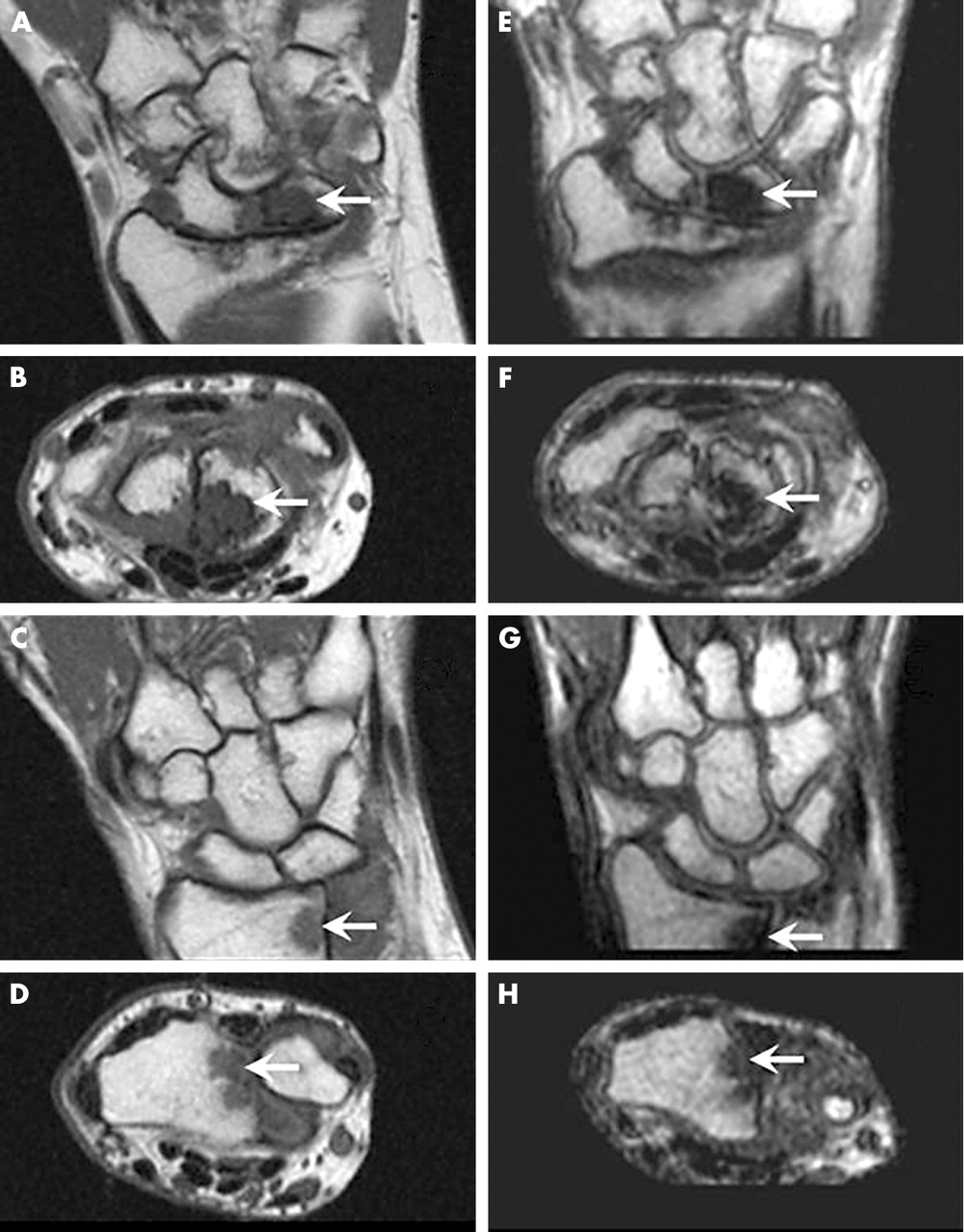
Synovitis in RA wrist joints visualised by high field and low field MRI. High field (A, B, C, D) and low field (E, F, G, H) axial images of the wrist joint before (A, C, E, G) and after (B, D, F, H) intravenous contrast injection. Post-contrast images in patient 1 (upper four images) show low grade synovitis (OMERACT grade 1) (arrows) in the intercarpal area of the wrist joint on high field MRI as well as on low field MRI, while high grade synovitis (OMERACT grade 3) (arrows) is seen in the radiocarpal area of the wrist joint in patient 2 (lower four images) on images obtained at both field strengths.
Bone marrow oedema on high field and low field MRI
As for erosions, 1431 bones were evaluated by high field MRI and low field MRI for the presence of bone marrow oedema. The numbers of bones with bone marrow oedema detected in the wrist and MCP joint bones were 102 and 55, respectively. The mean sensitivity, specificity, and accuracy of low field MRI for detection of bone marrow oedema (high field MRI was considered the standard reference) were 39%, 99%, and 95%. The overall ICC could not be computed because some of the measurements had fewer than two non-zero values (table 3, fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bone marrow oedema in RA wrist joint bones visualised by high field and low field MRI. High field (A) and low field (B) STIR images of the wrist. On high field MRI, a low grade bone marrow oedema (OMERACT grade 1) (arrow) is seen in the distal radius. The oedema at this site is not detected on low field MRI.
DISCUSSION
The main objective of this study was to investigate whether a low field dedicated extremity MRI unit could provide information on destructive and inflammatory joint changes equivalent to that of a standard high field MRI unit.
A most pertinent but often difficult question to answer when testing a new method is which reference method the new method should be tested against. In this study we chose to use high field MRI as the standard reference because most published MRI data are based on this method and because findings from high field MRI have been shown to be highly correlated with histopathological and miniarthroscopic findings25–28 and with future development of radiographic progression.29–32
Only a few published studies directly compare different MRI systems for the detection of arthritic joint disease. These studies have not incorporated any attempts to optimise the standard before starting the studies.13,14
The results of our study were divided into two major parts—namely, the results of the preliminary MR image evaluation and the results of the main study. In the preliminary image evaluation, the performance of the low field spin echo and gradient echo sequences was compared with high field MRI as the standard reference. Owing to markedly better sensitivity for bone erosions without loss of specificity, and better sensitivity for synovitis, although with a minor loss of specificity, the gradient echo sequence of the low field MRI unit was selected for the subsequent main image evaluation. Another advantage of gradient echo imaging was patient compliance, as the time needed for the MR examinations of the wrist and 2nd–5th MCP joints was about 45 minutes and 14 minutes for spin echo and gradient echo imaging, respectively.
Comparison of findings on x ray examination and MRI showed that MRI detects more erosions than plain film radiography. This finding is in accordance with reports by several authors.7,33–35 It should be noted that plain film radiography seems to detect a higher proportion of erosions in small bones—that is, the pisiform and base of the 5th metacarpal bone compared with the larger bones (table 3). This was also reported recently by Forslind et al, who found that plain film radiography was as sensitive as MRI for the detection of bone erosions in 5th MTP joints.36
Low field MRI in the main MR image evaluation demonstrated an overall very good agreement with high field MRI for the detection of bone erosions and synovitis.
For bone erosions, the agreement rates of the low field MRI unit and the high field were very encouraging, with overall sensitivities, specificities, accuracies, and ICCs of 94%, 93%, 94%, and 0.936 (p<0.005), respectively. The findings are to some degree in accordance with data published by Savnik et al and Taouli et al.13,14 However, Savnik’s group found similar rates based on total destruction scores, but for the individual bone or joint area the agreement rates were not as high.13 Taouli et al have recently reported that high field and low field MRI are equally informative about erosive joint changes in wrists and finger joints. However, Taouli only reported erosion scores and not the results of the assessments of the individual bones. Our data show that the low field dedicated extremity MRI unit could provide information on bone erosions equivalent to that of high field MRI for the individual bones—both with respect to detection and grading.
The agreement rates for synovitis were comparable to the findings for the destructive changes. The low field MRI unit displayed overall sensitivities, specificities, accuracies, and ICCs of 90%, 96%, 94%, and 0.923 (p<0.05), respectively. These findings are also comparable to previously published data, although the agreement rates were slightly lower.13 The poorer accuracy for synovitis, as well as erosions, in this study may be attributed to the lack of optimisation of the scanning sequences on the reference MRI unit.13 The study by Taouli et al also compared the synovitis scores, but their study only assessed synovitis by non-enhanced MRI in the coronal plane. The study by Taouli may suffer from a lack of sensitivity owing to the fact that the assessment of synovitis was performed on non-enhanced MR images—but on the other hand, the premises were the same for both images sets (high field and low field).
In view of our data, we conclude that with optimal MRI sequence selection, the low field dedicated extremity MRI unit can provide information on inflammatory changes (synovitis) in RA peripheral joints comparable to that obtained by contrast enhanced high field MRI, using standard 2D spin echo sequences.
The results of the comparison of the two MRI units for detection of bone marrow oedema were not as encouraging as the corresponding findings for erosions and synovitis. The overall sensitivity, specificity, and accuracy of the low field MRI unit were 39%, 99%, and 95%, respectively. The ICC levels were generally low. Our conclusion was that the sensitivity for bone marrow oedema on the low field MRI unit was low. However, when bone marrow oedema was demonstrated on the low field MRI unit, the findings were almost always correct (high specificity).
The low sensitivity of the low field MRI unit for the detection of bone marrow oedema may limit the usefulness of this type of scanner in RA if bone marrow oedema is proved to be a pathological event of major prognostic significance, as has been proposed by McQueen and others.29,37 But if bone marrow oedema is only an interim phase between synovitis and bone erosion, this may not have major impact on the usefulness of low field MRI in RA because the precursor of bone marrow oedema is generally accepted as being synovitis. The latter statement still needs to be validated in further scientific studies.
We found joint changes resembling bone erosions and synovitis in the healthy population, although only a few and only low grade changes. On the contrary, bone marrow oedema was not detected in any healthy subject. A more detailed description of these aspects has been reported elsewhere.38
In conclusion the low field dedicated extremity MRI unit used in this study provided information on bone erosions and synovitis comparable to the information obtained by high field MRI. High overall agreement was achieved for these types of abnormalities. x Ray examination displayed a markedly lower sensitivity and accuracy, though the specificity for detection of bone erosions was slightly higher than in low field MRI.
The low field MRI unit displayed high specificity but only moderate sensitivity for detection of bone marrow oedema. Further studies are needed to clarify the diagnostic and prognostic significance of the observed sensitivity of low field MRI for bone marrow oedema.
Acknowledgments
Supported by: Amersham Health and the Danish Rheumatism Association.
REFERENCES
Footnotes
-
Published Online First 13 January 2005