Article Text

Abstract
Background: Primary myocardial involvement due to microcirculation impairment is common in systemic sclerosis (SSc). Cardiovascular magnetic resonance imaging (MRI) and tissue Doppler echocardiography (TDE) were recently shown to be more sensitive than conventional methods for the respective assessment of myocardial perfusion and contractility. Previous studies have suggested that dihydropyridine-type calcium channel blockers mitigate both myocardial perfusion and function abnormalities.
Objective: To investigate the effects of nifedipine on myocardial perfusion by MRI and on contractility by TDE, in patients with SSc.
Patients and methods: 18 patients with SSc without clinical heart failure and with normal pulmonary arterial pressure (14 women, 4 men; mean (SD) age 59 (9) years; mean (SD) disease duration 7 (4) years, 10 with diffuse and 8 with limited cutaneous forms) were prospectively evaluated. The MRI perfusion index, determined from time-intensity curves, and systolic and diastolic strain rate determined by TDE were assessed at baseline, after a 72 hour vasodilator washout period, and after 14 days of oral treatment with nifedipine 60 mg/day.
Results: Nifedipine treatment led to a significant increase in the MRI perfusion index (mean (SD) 0.26 (0.07) v 0.19 (0.05) at baseline, p = 0.0003) and in systolic and diastolic strain rate (2.3 (0.6) v 1.5 (0.4) s−1 at baseline, p = 0.0002, and 4.2 (1.6) v 3.0 (1.2) at baseline, p = 0.0003, respectively).
Conclusion: Fourteen days of treatment with nifedipine simultaneously improves myocardial perfusion and function, as evaluated by highly sensitive and quantitative methods.
- CT, computed tomography
- DTPA, gadolinium-diethylenetriamine pentaacetic acid
- LV, left ventricular
- MRI, magnetic resonance imaging
- SI, signal intensity
- SPECT, single photon emission computed tomography
- SR, strain rate
- SSc, systemic sclerosis
- TDE, tissue Doppler echocardiography
- Tlco, carbon monoxide transfer factor
- systemic sclerosis
- calcium channel blockers
- magnetic resonance imaging
- tissue Doppler echocardiography
- nifedipine
Statistics from Altmetric.com
- CT, computed tomography
- DTPA, gadolinium-diethylenetriamine pentaacetic acid
- LV, left ventricular
- MRI, magnetic resonance imaging
- SI, signal intensity
- SPECT, single photon emission computed tomography
- SR, strain rate
- SSc, systemic sclerosis
- TDE, tissue Doppler echocardiography
- Tlco, carbon monoxide transfer factor
- systemic sclerosis
- calcium channel blockers
- magnetic resonance imaging
- tissue Doppler echocardiography
- nifedipine
Systemic sclerosis (SSc) is a connective tissue disease characterised by widespread vascular lesions and fibrosis of the skin and internal organs. Primary myocardial involvement is common in SSc1–5 and is recognised as a poor prognosis factor.6,7 SSc vascular lesions display generalised impairment of the microcirculation, including vasospasm. Myocardial fibrosis is thought to follow repeated focal ischaemia, resulting from abnormal vasoreactivity with or without associated structural vascular disease. Indeed, some histological examinations have disclosed diffuse patchy fibrosis, with contraction band necrosis unrelated to epicardial coronary artery stenosis,2 whereas other studies have shown concentric intimal hypertrophy associated with fibrinoid necrosis of intramural coronary arteries.8
Single photon emission computed tomography (SPECT), echocardiography, and radionuclide ventriculography have previously been used to investigate respectively myocardial perfusion and contractility. The data showed that myocardial perfusion abnormalities together with various degrees of left and right ventricular dysfunction were common.3–5,9,10 Moreover, using these methods, vasodilators such as nifedipine, nicardipine, and captopril were shown to mitigate acutely both myocardial perfusion and function.10–13 However, these methods may have some limitations in the assessment of the efficacy of vasodilator treatments. SPECT is a qualitative and semiquantitative method, but quantitative methods may be preferable for a direct comparison. Moreover, echocardiography and radionuclide ventriculography, which are valuable methods for determining global and regional contractility, may be influenced by loading conditions and adjacent segment motion.
In contrast, cardiovascular magnetic resonance imaging (MRI) is an accurate quantitative method, lately developed for the non-invasive assessment of myocardial perfusion.14–17 In a recent study MRI detected subendocardial perfusion abnormalities in patients with cardiac syndrome X, suggesting that it has a higher sensitivity than conventional perfusion techniques.18
Tissue Doppler echocardiography (TDE) is a recently developed ultrasound technique, that allows direct measurements of myocardial velocities and strain rate (SR).19,20 Previous studies have demonstrated that SR determined by TDE is a powerful indicator of myocardial contraction, more sensitive, not affected by myocardial translational motion, and less load dependent than conventional echocardiography.21–24
We therefore investigated the effects of nifedipine on myocardial perfusion by MRI and on regional function by TDE in patients with SSc.
PATIENTS AND METHODS
Patients
Eighteen consecutive patients fulfilling LeRoy’s classification criteria for SSc25 were included. The clinical features of their disease were assessed as recommended.26 The exclusion criteria were pregnancy, symptoms of heart failure, venous distension and/or recent major lower limb oedema, pulmonary arterial hypertension (systolic arterial pressure >40 mm Hg and/or mean artery pressure >25 mm Hg determined by echocardiography), severe pulmonary involvement (forced vital capacity or carbon monoxide transfer factor <50% of the predicted value), renal involvement (creatinine concentration >106 μmol/l), or severe disease complications such as cancer or gangrene. Three months of stable current treatment were necessary for inclusion, and prednisone at a dose of <10 mg/day was authorised. Vasodilator treatments had to be withdrawn at least 3 days before inclusion, a time interval which was greater than five drug half lives. All patients gave informed consent for all procedures and the study was approved by the local ethics committee (Paris, Cochin).
The following investigations were carried out for all patients: laboratory tests including blood cell counts, Westergren erythrocyte sedimentation rate, C reactive protein levels, serum creatinine concentration, anticentromere and antitopoisomerase I antibody assays. Pulmonary involvement was assessed by computed tomography (CT), forced vital capacity, and the ratio of the carbon monoxide transfer factor to haemoglobin concentration (Tlco/Hb). Pulmonary arterial systolic pressure was determined by Doppler echocardiography at rest, based on the tricuspid and or pulmonary regurgitation, adding 10 mm Hg as an estimation of right atrial pressure.
Myocardial evaluations were performed over a 30 minute period, in patients at rest, at room temperature, at baseline and after 2 weeks of nifedipine treatment (20 mg three times/day). All measurements were performed under similar conditions, with MRI performed first, followed by TDE 1 hour later.
Magnetic resonance imaging
All patients were examined in the supine position (1.5 T Echospeed GEMS, Milwaukee, USA) using a phased array cardiac dedicated coil. After determination of the axis and length of the left ventricular (LV) cavity, three short axis planes were imaged. The distance between each plane was individually set as one third of the end systolic length of the LV cavity. An interleaved notched saturation segmented k-space turbogradient echo/echo planar imaging hybrid technique with notched saturation prepulse and T1 preparation (echo time = min full, R-R interval = 2, flip = 25; inversion time = 160 ms; matrix 128×128; slice thickness 8 mm) was used. Multislice acquisitions were performed during the first pass of 0.025 mmol gadolinium-diethylenetriamine pentaacetic acid (DTPA)/kg body weight (Guerbet) flushed with 10 ml 0.9% NaCl (flow rate, 5 ml/s; Medrad, Spectris). Images were acquired during breath holding for 10 heart beats before and 60 heart beats during the injection.
Visual image analysis
Hard copy images without any information (including name and date) were developed and the enhancement of axial images retrospectively analysed side by side by two radiologists. If a segment showed a reduced signal intensity (SI) or delayed wash-in, it was regarded as pathological (perfusion defect). The two readers, who were unaware of the treatment, independently evaluated the sets of images with a three point rating scale: 0 = homogeneous enhancement considered as normal myocardial perfusion; 1 = one segmental perfusion defect; 2 = two or more perfusion defects. A consensus reading was used for discordant grades. Figure 1 provides some examples.

Mid-ventricular short axis view after bolus of gadolinium-DTPA exhibiting different patterns of subendocardial perfusion defect (visual analysis) before treatment with nifedipine. Notice that these defects do not correspond with any epicardial coronary artery distribution. (A) small inferoseptal defect (scored as grade 1); (B) larger defect anterior and septal defect (scored as grade 2); (C) diffuse subendocardial defect (scored as grade 2).
Parametric image analysis
The endocardial and epicardial contours were traced by an examiner, who was unaware of the angiography thanks to a dedicated software (MASS, Medical Imaging Solutions, Leiden, Netherlands), and corrected manually for displacements (for example, breathing). The outer 50% of the myocardium was excluded to get stronger weighting of the subendocardium. Cavitary and myocardial SIs of the LV cavity were determined for all time points. This software allows the determination of a time-intensity curve for the whole myocardium. The SIs before injection of the agent at time zero are averaged and used as offset. The peak SI, time to peak, and maximum upslope of the SI time curves were thus determined. If the whole myocardium showed a diffuse reduced peak SI or reduced time to peak on a parametric image (bull’s eyes view from apex to base), it was graded as 2—two or more perfusion defects. Segmental perfusion defect initially assessed with visual analysis was also analysed on parametric images and regarded as pathological only if a reduced peak SI or reduced time to peak was found on the same segment. Figure 2 shows an example of one patient representative of the whole group. A myocardial perfusion index was determined by dividing the myocardial upslope through the myocardium by the myocardial upslope through the LV cavity. This correction allows for the differences of speed and compactness of the contrast agent bolus and thus avoids taking into account the interstudy variation of extrinsic parameters such as the heart rate and the arterial pressure.
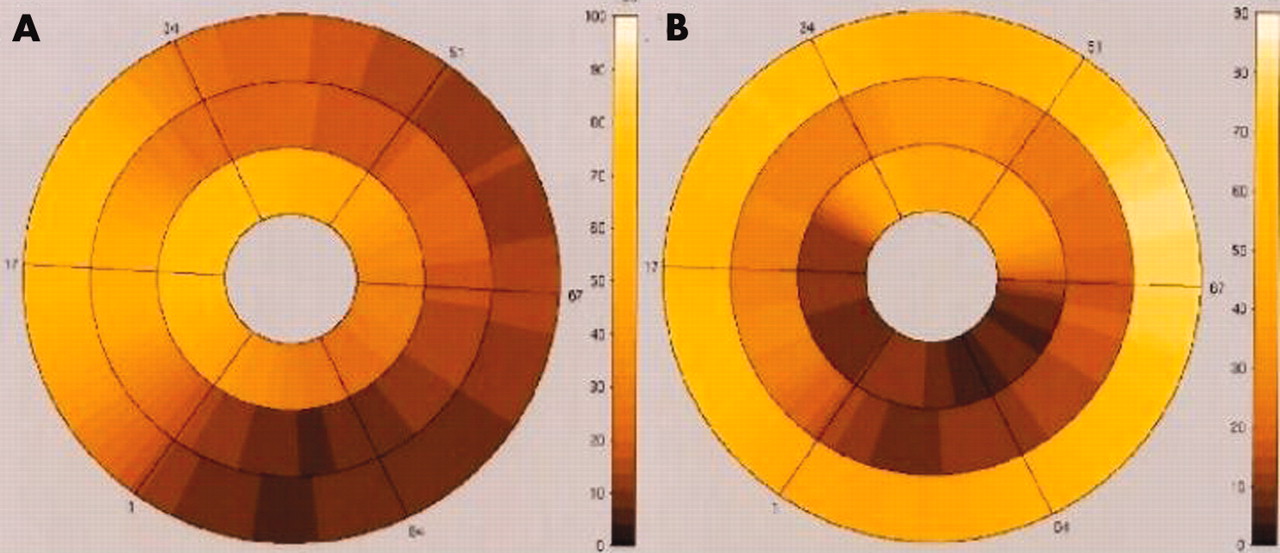
Parametric analysis by MRI in one patient. (A) Parametric analysis (peak SI on bull’s eye) confirming diffuse hypoperfusion (scale from yellow for high peak SI to dark red for low peak SI) before treatment with nifedipine. (B) Parametric bull’s eye analysis (peak SI) showing global improvement of myocardial perfusion with almost diffuse increased peak SI after treatment with nifedipine.
Tissue Doppler echocardiography
TDE was performed with an ATL HDI5000 system (ATL ultrasound, Bothell, Washington, DC) equipped with tissue Doppler, second harmonic imaging technologies, and a 2–3.5 MHz phased array transducer. Myocardial velocities were measured by an experienced practitioner, in the posterior wall, from a parasternal short axis view at the level of the papillary muscle on M mode TDE recordings. Special attention was paid to the proper alignment of the beam perpendicular to the left ventricular wall, and gains were adjusted to optimise the images. Offline TDE measurements were made by two cardiologists (CM, OP), according to a blind protocol, with the HDI Laboratory software package installed on a standard PC workstation.
We first manually drew lines in the subendocardium and in the subepicardium, in order to determine endocardial and epicardial velocity patterns over time.
Peak systolic velocity and peak early diastolic velocities, defined as maximal velocity during LV ejection time and early diastole, respectively, were then determined from endocardial (EndoVSYS, EndoVDIA) and epicardial (EpiVSYS, EpiVDIA) velocity patterns.
The peak systolic and early diastolic SR was defined as the maximal transmural velocity gradient during systolic (SRSYS) and early diastolic (SRDIA) times and was calculated as: SR (s−1) = (EndoV−EpiV)/d (where d is the distance between endocardium and epicardium). Figure 3 shows the SR determination in one patient at baseline.

SR measurement by TDE at baseline in one patient. (A) Colour M mode TDE acquisition in the inferior wall from a short axis parasternal view—subendocardium and subepicardium delimitation. (B) Extraction of myocardial velocities in the subendocardium (black) and subepicardium (grey line). (C) SR determination.
The mean of the two cardiologists’ results was used for statistical analysis.
Statistical analysis
To detect a Δ/SD = 1 increase in the perfusion index,3 with a unilateral α value of 0.05 and a β value of 0.1, 18 patients were enrolled. Data, expressed as means (SD), were analysed using Mann-Whitney (unpaired data) and Wilcoxon (paired data) tests for comparison of the groups. Spearman’s rank correlation test was used for assessment of the relationship between quantitative variables. McNemar’s test, a χ2 test for paired analysis, was used to compare the number of ischaemic segments on MRI. Values of p<0.05 were considered significant (Statview Software, Abacus Concept, Berkeley, CA, 1998).
RESULTS
Clinical findings
Eighteen patients were included (14 women, 4 men, 10 patients with diffuse cutaneous disease and 8 with limited cutaneous disease); table 1 presents their clinical and biological characteristics. Blood pressure was not affected by 14 days of nifedipine treatment and although the heart rate increased, the systolic pressure-heart rate product remained unchanged (table 2).
Clinical and biological characteristics of the patients with systemic sclerosis (SSc)
Haemodynamic, myocardial perfusion, and strain rate values
Magnetic resonance imaging
Thirteen patients had at least one segmental perfusion defect at baseline; seven had one and six had two or more. The myocardial perfusion index was significantly reduced in patients with more than one segmental defect (n = 6) as compared with the other patients (n = 12; 0.154 (0.01) v 0.213 (0.04), p = 0.01), and there was a trend for reduced perfusion when patients with one segmental defect (n = 7) were compared with patients without any defect (n = 5; 0.183 (0.05) v 0.208 (0.03), p = 0.09).
Nifedipine treatment increased the myocardial perfusion index (from 0.19 (0.05) to 0.26 (0.07), p = 0.0003) (fig 4, table 2) and significantly decreased the number of patients with at least one segmental perfusion defect from 13/18 (72%) to 6/18 (33%; p = 0.02). The number of patients with more than one segmental perfusion defect decreased from 7/18 (39%) to 0/18 (p<0.05). Figure 2 shows MRI images with baseline aspect (A) and changes after nifedipine treatment (B) for one patient representative of the whole group. Age, disease duration, cutaneous form of the disease, pulmonary artery pressure, pulmonary fibrosis, carbon monoxide transfer factor, autoantibody status, and treatment were not associated with baseline MRI results or changes in perfusion index values after treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual data (25th to 75th centile) of significant increase in myocardial perfusion index, as measured by MRI (A) and increase in systolic strain rate as measured by TDE (B), after 14 days of treatment with nifedipine (60 mg/day).
Tissue Doppler imaging
The interobserver variability was 0.13 for systolic strain rates and 0.17 for diastolic strain rates, results which are consistent with previous studies.24 Nifedipine significantly increased systolic SR from 1.5 (0.4) s−1 at baseline to 2.3 (0.6) s−1 at 14 days (p = 0.0002) and diastolic strain rates from 3.0 (1.2) s−1 at baseline to 4.2 (1.6) s−1 at 14 days (p = 0.0003). Figure 3 shows the systolic SR results. The characteristics of the patients with SSc were not associated with significant differences in TDE baseline values or changes.
DISCUSSION
Our main finding was that 14 days of treatment with nifedipine improved both myocardial perfusion and function, as evaluated by two modern, highly sensitive and quantitative methods, MRI and TDE.
SPECT perfusion abnormalities have frequently been described in patients with SSc, and improvements in perfusion after treatment with nifedipine, nicardipine, and captopril have been reported previously, suggesting that at least some of the defects observed were not fixed fibrotic defects.3,9 However, SPECT is limited by the occurrence of attenuation artefacts, and the use of radioactive tracers precludes follow up examinations. MRI may constitute an ideal alternative as it is a non-invasive, quantitative, highly sensitive method for the assessment of myocardial perfusion. Indeed, parameters analysed for myocardial perfusion evaluation are usually determined by analysing the first pass of a contrast agent bolus through the myocardium. Visual assessment may facilitate rapid diagnosis without the need for quantification, and high resolution perfusion MRI techniques can be used to identify small subendocardial defects. These defects do not correspond to any epicardial coronary artery distribution, and therefore are highly suggestive of microvascular alteration. In our study, perfusion MRI disclosed segmental perfusion defects at rest in patients with SSc and showed that most of these segmental perfusion defects improved after 14 days of treatment with nifedipine.
Moreover, the myocardial gradient (the rate of increase of the myocardial signal) significantly increased after 14 days of treatment with nifedipine. Despite the use of an extravascular contrast agent (gadolinium-DTPA) that rapidly diffuses into the extracellular space, the rate of early myocardial signal enhancement during the first pass (gradient) is related to myocardial blood flow and vascular resistance. Therefore, the increase in the rate of myocardial signal enhancement after treatment with nifedipine may result from the lowering of myocardial vascular resistance. Intravascular contrast agents, which are currently under development, may constitute a step towards more accurate quantitative analysis in the future.
LV function in patients with suspected cardiomyopathy is commonly assessed by echocardiography or radionuclide ventriculography. Some measurements, such as end diastolic diameter, fractional shortening, and LV ejection fraction, are made in routine clinical practice. However, these indices are load dependent and do not systematically reflect the contractile state of the myocardium.
Here, TDE has been introduced as a quantitative, more objective, and sensitive method for the assessment of myocardial function. TDE is a new approach that allows direct and valid measurement of myocardial velocities and SR.19,20 Myocardial SR is related to the difference in velocities that exists between endocardium and epicardium (subendocardial velocities are higher than subepicardial velocity, resulting in an intramyocardial velocity gradient or SR), and has been shown to be a strong index of contractility, independent of myocardial translation21,22,23 and less dependent on loading conditions.27,28 Furthermore, SR determined by TDE is a more sensitive method than conventional echocardiography or radionuclide ventriculography for detecting changes in myocardium contractility.22,29,30 As peak systolic and early diastolic SR are respective markers of regional contractility and diastolic function,23,24,31 our study strongly suggest that nifedipine improves myocardial intrinsic properties, possibly by increasing the myocardial perfusion.
On the other hand, calcium channel blockers are antihypertensive agents and nifedipine has also been reported to result in an increase in sympathetic tone. Therefore, our result could be partially a result of these changes in loading conditions. However, SR determined by TDE is less load dependent than other methods,23,24,27,28 and afterload estimated by the systolic blood pressure-heart rate product did not change significantly after nifedipine treatment (table 2). In view of these results, together with the increased perfusion demonstrated by MRI, we assume that increases in myocardial perfusion may be the main determinant of the observed increased contractility.
Contrast echocardiography is a recent and accurate method for determining global and regional perfusion as well as global and regional contractility.32,33,34 MRI is also useful for determining local and global myocardial perfusion and provides a “one-stop shop” examination with fine analysis of the segmental contractility at the same time. These methods may be considered in future studies aimed at evaluating the cardiac impact of vasodilators in patients with SSc.
The limited number of patients included in this series, and the global nature of MRI evaluation in contrast with the segmental evaluation by TDE, may account for the absence of correlation between perfusion and function improvement. Moreover, myocardial perfusion may increase in segments with various degrees of fibrotic lesions, resulting in a different impact on function parameters.
The number of patients precluded effective comparison of cardiac results and SSc characteristics; however, it should be noted that no difference in cardiac baseline data or nifedipine-induced changes were seen for the two cutaneous subsets of SSc. This is consistent with myocardial involvement in both cutaneous subtypes of SSc.5 We assessed the effects of nifedipine treatment on myocardial perfusion and segmental function after only 14 days; thus, no formal conclusion can be drawn from this study about the possible sustained therapeutic benefits of this drug. Moreover, as this study was not conducted according to a randomised, controlled, double blind protocol, our results may be considered as preliminary and require confirmation. However, these results emphasise previous data and highlight the beneficial microvascular and cardiac effects of nifedipine, which should be regarded as a crucial treatment in SSc.
CONCLUSION
Fourteen days of treatment with nifedipine simultaneously improved myocardial perfusion and regional function, respectively, determined by quantitative, accurate, and highly sensitive methods, MRI and TDE. Our data demonstrate the strikingly beneficial short term myocardial effects of this drug in patients with SSc.
REFERENCES
Footnotes
-
↵* These authors contributed equally to this work.
-
Published Online First 11 February 2005