Article Text

Abstract
Background: The study was based on the Danish DANBIO and the Norwegian NOR-DMARD databases.
Objective: To investigate changes in prescription practice during the first 3 years of post-marketing use of biological drugs, and to determine the proportion of patients who would not have received tumour necrosis factor (TNF) blocking agents if the prescription guidelines of the UK and the Netherlands had been applied.
Methods: Patients with rheumatoid arthritis (RA) receiving TNF blocking agents from Denmark (n = 823, median age 56.0, 72.2% women) and Norway (n = 371, median age 52.5, 75.4% women) were studied. Prescription guidelines in the UK and the Netherlands were applied to the data.
Results: Baseline disease activity and number of previous DMARDs declined significantly during the 3 years (median baseline DAS28 decreased from 5.8 to 5.2 in Denmark (p<0.001) and from 6.0 to 5.6 in Norway (p<0.01)). 47.9% and 41.3% of the Norwegian and Danish patients, respectively, did not meet the UK criteria for using TNF blocking agents, and 10.5% and 5.7% did not meet the Dutch criteria.
Conclusion: Danish and Norwegian prescription practices of biological treatments in RA were similar, and became less stringent from 2000 to 2003. Prescriptions agreed well with the Dutch guidelines, but almost half the patients did not meet the UK guidelines.
- CRP, C reactive protein
- DAS28, Disease Activity Score 28
- DMARD, disease modifying antirheumatic drug
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
- rheumatoid arthritis
- tumour necrosis factor blocking agents
- pharmacosurveillance
- clinical databases
Statistics from Altmetric.com
- CRP, C reactive protein
- DAS28, Disease Activity Score 28
- DMARD, disease modifying antirheumatic drug
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
The tumour necrosis factor alpha (TNF) antagonists adalimumab, etanercept, and infliximab have demonstrated high efficacy in clinical trials in patients with rheumatoid arthritis (RA).1–,3
Guidelines for post-marketing use typically require failure of one or more traditional disease modifying antirheumatic drugs (DMARDs; usually including methotrexate) and a certain minimum level of disease activity before starting biological treatment. In some countries the right to prescribe the drugs has been centralised (van Riel PL, Dutch guidelines for the use of TNF blocking agents, personal communication),[4 5] in other countries the decision to start treatment is made by the treating rheumatologist.
An international consensus recommendation on the use of biological drugs in rheumatic diseases was first published in 2000. Yearly updates have remained largely unchanged, and the consensus statement from May 20036 recommends that patients starting biological treatment should have active disease and have tried a minimum of one traditional DMARD (unless they are relatively contraindicated), and that cost considerations should be taken into account. However, little is known about how the prescription patterns for the biological agents have changed in clinical practice over time, and how the access to such treatments may vary between countries owing to different national guidelines. Clinical databases have been established in Denmark and Norway—as well as in other countries—to examine the effectiveness and adverse events of the biological drugs.7,8,9,10,11
The present analyses aimed at investigating changes in prescription practice during the first 3 years of post-marketing use of TNF blocking agents in Norway and Denmark and examining the proportion of patients who would not have received these blocking agents if the prescription guidelines of the United Kingdom (UK) and the Netherlands had been applied.
MATERIALS AND METHODS
Patients registered in the Danish (DANBIO) and the Norwegian (NOR-DMARD) databases from 2000 to 2003 were included. DANBIO is a nationwide, voluntary, rheumatological database of biological treatments. NOR-DMARD includes patients with inflammatory arthropathies starting DMARDs or biological treatments in five Norwegian departments of rheumatology.8
Both databases cover about 85% of all prescriptions, and the patients are followed up longitudinally for an examination of effectiveness and tolerance. Registration began in autumn 2000, and included detailed information about population demographics and previous treatments, as well as core measures of disease activity (table 1⇓). The 28 joint count Disease Activity Score (DAS28) based on the C reactive protein (CRP)12 was calculated. The present analyses focused on patients who fulfilled the classification criteria of RA13 and started TNF antagonists during the period 2000–2003.
Patient characteristics and disease activity at the initiation of biological treatment
Analyses
The patients starting TNF inhibitors were divided into three groups according to the period of treatment initiation (2000–2001, 2002, and 2003), and the baseline characteristics of the groups were compared. The prescription guidelines of two European countries (the United Kingdom (UK): minimum two previous DMARDs and DAS28 >5.1 and the Netherlands (NL): minimum one previous DMARD and DAS28 >3.2) were applied to the data from each year, and the proportions of patients who would not be considered eligible for TNF inhibitors if they were living in the UK or the NL were calculated.
Statistical analyses were undertaken with the SPSS (Statistical Package for Social Sciences) program, version 11.5 (SPSS, Chicago, Illinois, USA). Non-parametric tests (Kruskal-Wallis and Mann-Whitney) were used for the comparison of continous variables. Probability (p) values <0.05 were considered significant.
RESULTS
In total, 823 Danish patients with RA (median age 56.0 years (range 20–88), 72.2% women) and 371 Norwegian patients with RA (median age 52.5 years (range 17–89), 75.4% women) started treatment with TNF inhibitors in the period 2000 to 2003 (table 1⇑). A high degree of similarity was seen in the demographic characteristics and disease activity measures of the two patient populations.
The number of new patients increased considerably from 2000 to 2003 in both countries (table 1⇑), as did the number of patients with disease duration of less than 2 years (Denmark: 0 to 27 patients, Norway: 9 to 23 patients). No significant differences in patient age and proportion of women within the three groups were seen.
Table 1⇑ shows that the number of previous DMARDs and levels of disease activity declined with time. For example, the median baseline DAS28 declined from 5.8 (2000–01) to 5.2 (2003) in the Danish patients (Kruskal-Wallis, p<0.001) and from 6.0 to 5.6 in the Norwegian patients (Kruskal-Wallis, p<0.01) (fig 1⇓).
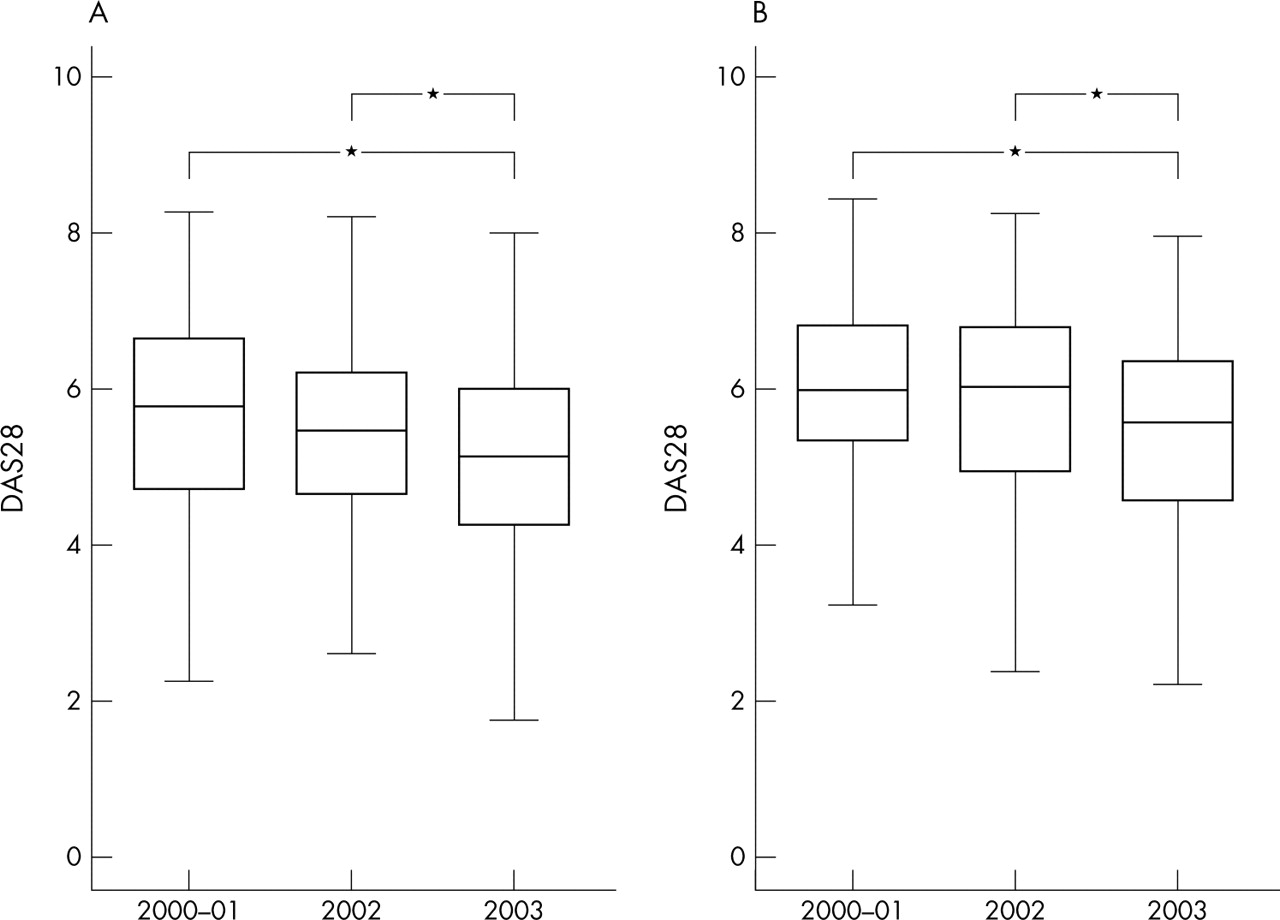
Median disease activity score of 28 joints (DAS28 CRP based) at treatment initiation presented as box plots with 25th and 75th centiles in years 1, 2, and 3 of post-marketing use of the biological drugs. *p<0.05 (Mann-Whitney). (A) Denmark, (B) Norway.
Figure 2⇓ shows the proportions of TNF treated patients in Denmark and Norway who would not have received such treatments in the UK and the Netherlands. During the whole period 41.3% of the Danish and 47.9% of the Norwegian patients would not have been treated in UK, and as many as 49.8% and 57.0%, respectively, during the most recent period (year 2003). The proportions of patients who did not meet the criteria increased numerically from 2000 to 2003 (figs 2A and B⇓).

{kind=link}
{kind=link}
Percentage of Danish and Norwegian patients who would not have been treated in: (A) the United Kingdom (UK); (B) The Netherlands (NL).
DISCUSSION
The present analyses have two key messages: Firstly, less stringent disease activity criteria are currently used when prescribing TNF inhibitors for patients with RA in Denmark and Norway than during the years when these drugs were first available. Secondly, even in the Western Europe, access to modern treatments varies considerably based on national guidelines.
The change in prescription practice over time may also apply to other populations, as suggested by previous data.7 The widening indication for the use of biological treatments probably reflects the increased pool of experience in clinical use combined with the good efficacy and safety profile of the drugs, increased demand from patients, and a gradually changing treatment goal for many physicians towards aiming at remission in their patients. Finally, a treatment licence from the authorities may have been initially more difficult to obtain.
Although the patients starting treatment in 2003 had less clinically active disease than in 2000–01, they still had active and severe disease. The median disease duration continued to be more than 8 years in both the Danish and the Norwegian populations, although it decreased significantly in the Danish population during the period. This is comparable with data from clinical follow up studies in Sweden.7 The present data also show that an increasing number of patients with <2 years’ disease duration are being treated with biological agents. However, they comprise only a fraction of all patients. The recommendations to treat severe RA early and aggressively supports this development.14
The Scandinavian prescription practices agreed well with the Dutch guidelines. In contrast, about half of the patients in this study did not meet the UK prescription guidelines, and this proportion increased with time, indicating that population based studies of biological treatments in Scandinavia and the UK comprise different cohorts. This study also highlights the fact that despite international consensus statements,6 access to recent, effective treatments may vary across Europe.
This study has certain limitations. It compares Danish and Norwegian data, although the Danish database is nationwide and the Norwegian database is not. There is, however, no particular reason to expect that prescription practice in other parts of Norway should differ from the five centres participating in this study, which represent four of the five geographical health regions in Norway. The prescription guidelines of Denmark and Norway as well as, for instance, Germany,4 do not require a certain DAS28 level before treatment initiation. This hindered a strict evaluation of our own prescription practice for starting TNF blocking agents, but the study showed that patients had active disease and, generally, treatment with at least one DMARD had failed.
In conclusion, the prescription practices of biological treatments in RA in Denmark and Norway were similar and changed from 2000 to 2003 towards treating patients with lower (but still severe) disease activity, shorter disease duration, and fewer previous DMARDs. This study also highlights the fact that access to treatment differs across countries in the European Union, which must be a challenge for politicians and decision makers.
Acknowledgments
We thank contributing departments of rheumatology at hospitals in Denmark (Ålborg, Århus (Ulrik Tarp), Bispebjerg, Esbjerg, Fredericia, Frederiksberg (Anne Petri), Frederiksborg Amt, Gentofte, Glostrup (Anette Hansen), Gråsten (Lis Smedegaard Andersen), Herlev, Hjørring, Holbæk, Holstebro, Horsens, Hvidovre, Hørsholm, Køge, Kolding, Næstved, Nykøbing Falster, Odense, Rigshospitalet, Roskilde, Slagelse, Vejle and Viborg) and Norway (Drammen (Cecilie Kaufmann), Lillehammer (Knut Mikkelsen), Oslo, Tromsø (Bjørn-Yngvar Nordvåg), Trondheim (Erik Rødevand)).
The Danish Rheumatism Association and the Norwegian Directorate of Health supported the study. The Institute for Rational Pharmacotreatment (Janne Unkerskov and Tomaas Ravn) is also acknowledged. DANBIO is indebted to the head of the Institute for Rational Pharmacotreatment Jens Peter Kampmann, MD, DMSc, who hosted and financed DANBIO from 2000 to 2003. Since 2004 Abbott, Wyeth and Schering-Plough have supported DANBIO. These companies, and in addition Amgen, Aventis, and MSD, have supported NOR-DMARD. All are acknowledged for their support. The sponsors had no influence on data collection, analyses, or publication.
REFERENCES
Footnotes
Published Online First 7 January 2005