Article Text

Abstract
Background We investigated the effects of individualised combined resistance and aerobic exercise on microvascular and macrovascular function in rheumatoid arthritis (RA) patients.
Methods Forty age-matched, gender-matched and body mass index (BMI)-matched patients were allocated to either an exercise group, receiving a 6 months tailored aerobic and resistance exercise intervention, or controls receiving only information about the benefits of exercise. Participants were assessed for microvascular (acetylcholine (Ach) and sodium nitroprusside (SNP)) and macrovascular (flow-mediated dilatation (FMD) and glyceryl trinitrate (GTN)) endothelial function, maximal oxygen uptake, disease activity and severity (C-reactive protein (CRP), disease activity score 28 and health assessment questionnaire). Data were collected at baseline, 3 months and at the end of the intervention (6 months).
Results At baseline, demographic, anthropometric, disease-related characteristics and endothelial function parameters were similar between the exercise and control groups (p>0.05). Repeated measures analysis of variance revealed a significant improvement in endothelial function parameters at 3 (GTN: p<0.001) or 6 months (Ach: p=0.016, SNP: p=0.045, FMD: p=0.016) in the exercise but not in the control group. Generalised estimated equations detected that maximal oxygen uptake was a strong predictor for the observed changes in Ach (p=0.009) and GTN (p<0.001) whereas logCRP for SNP (p=0.017) and GTN (p=0.008).
Conclusions An exercise programme designed to meet individual needs and physical abilities significantly improves microvascular and macrovascular function in parallel with disease-related characteristics in RA patients. The potential long-term beneficial effects of such interventions at reducing cardiovascular risk in these patients merit further exploration.
Clinical Trial Registration ISRCTN50861407.
- Cardiovascular Disease
- Inflammation
- Rheumatoid Arthritis
- Rehabilitation
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a chronic disease characterised by joint destruction, functional disability and increased mortality. The latter is mainly attributed to cardiovascular disease (CVD) and may be due to increased prevalence of traditional CVD factors1–4 as well as the vascular effects of high-grade inflammation. This may be why RA patients demonstrate inferior endothelial function in different vascular beds compared with the general population.5 ,6
To date, research has focused only on the effects of medication on microvascular or macrovascular function in patients with RA. However, exercise is a cost-effective intervention that may significantly improve cardiorespiratory fitness, CVD risk factors and 10-year CVD event probability in RA.7–9 Exercise training has also been shown to improve endothelial function in other populations10 but this has not yet been studied in RA. The aim of the present study was to investigate the effects of an individualised exercise training programme on microvascular and macrovascular function in patients with RA.
Methods
Participants
Forty consecutive RA patients were allocated into two groups matched for age, gender and body mass index: 20 patients performed a 6 month individualised resistance and aerobic exercise training intervention whereas the remaining 20 (control group) received only advice about the benefits of exercise using commercially available leaflets (Registered trial: ISRCTN50861407). A consort flow diagram with the details of enrolment, allocation and analyses appear in figure 1. Details about the power calculations (with VO2max as the main outcome measure) and the inclusion/exclusion criteria of this project are described elsewhere.8 All patients were assessed at baseline, 3 and 6 months for demographic, anthropometric, cardiovascular and RA-related parameters. Assessors were blinded to the procedures.
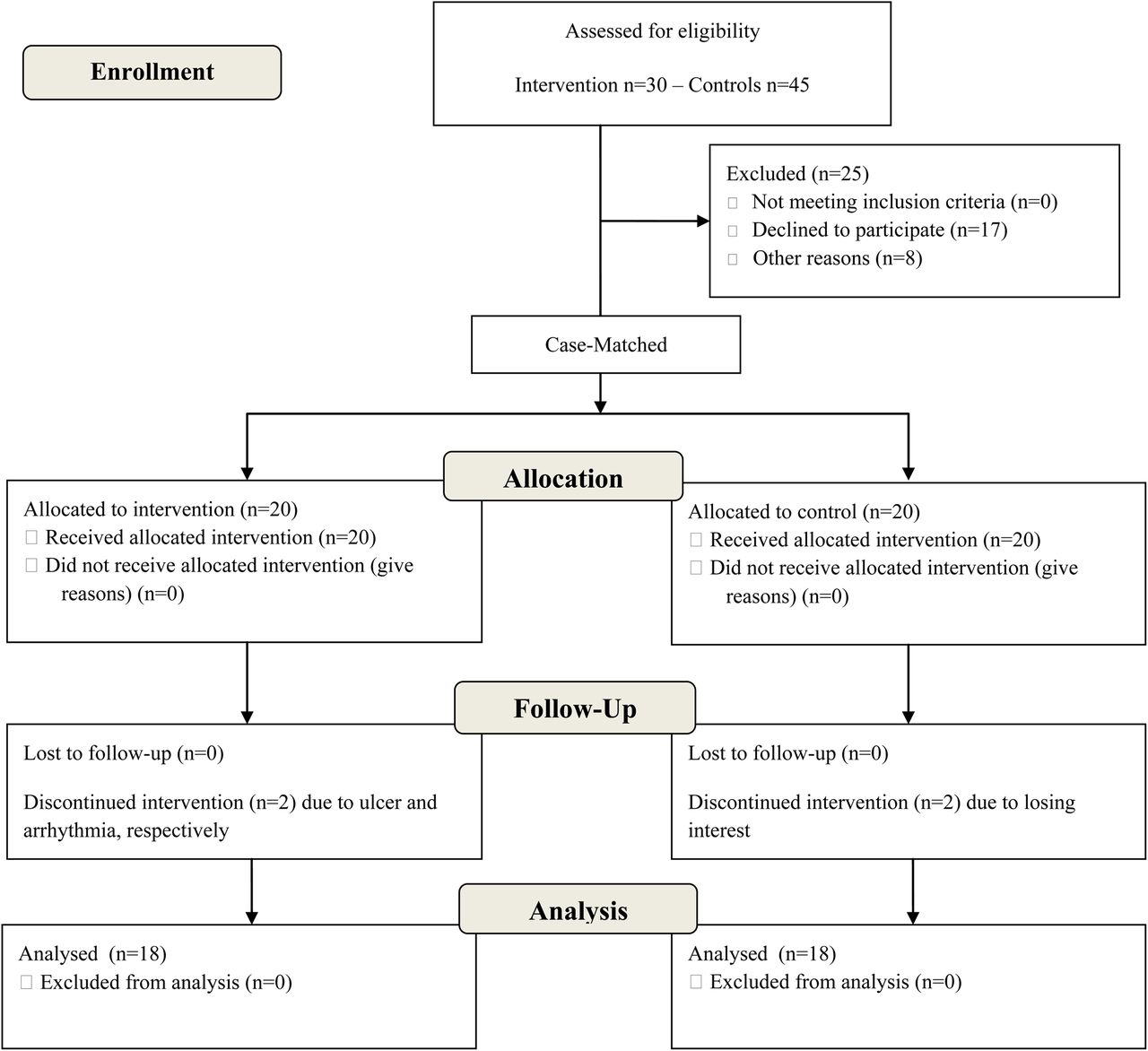
{kind=link}
CONSORT flow diagram.
General procedures
Within 1 week, participants were assessed for VO2max, demographic and anthropometric characteristics, physical function, disease activity (first appointment) and endothelial function (second appointment). Based on each patient's VO2max results, functional ability, personal preferences and the guidelines for exercise prescription by the American College of Sports Medicine,11 an individualised resistance and aerobic exercise training programme was developed.
Weight, body fat and fat-free mass were evaluated using a Tanita BC-418 Analyser (Tokyo, Japan). Demographic data were collected via a self-administered questionnaire. All patients were assessed on a treadmill for VO2max (HP Cosmos Mercury, Germany). Cardiorespiratory parameters were evaluated via breath-by-breath analyses (CORTEX, Germany). Disease activity was assessed using the 28 joint disease activity score (DAS28) and physical function via Stanford Health Assessment Questionnaire (HAQ).8
Endothelial function
Microvascular
Endothelium-dependent and endothelium-independent functions were evaluated via Laser Doppler imaging (Moor LDI 2 SIM, UK) using iontophoresis (1% acetylcholine (Ach) endothelium-dependent and 1% sodium nitroprusside (SNP) endothelium-independent (Sigma Chemical Co., USA) in 0.5 mL of saline).
Macrovascular
Endothelium-dependent function was measured via flow-mediated dilatation (FMD) with a high-resolution ultrasound (Acuson Antares, Siemens PLC, UK) and endothelium-independent function via a 500 mg sublingual tablet of glyceryl trinitrate (GTN), as previously described.12
Statistical analyses
Kolmogorov–Smirnov tests were used to investigate normal distribution and accordingly, Mann–Whitney or paired-samples t tests was employed to investigate differences between groups at baseline. Repeated measures analysis of variance (RMANOVA) with two levels (groups: exercise vs control and time: baseline vs 3 months vs 6 months) were used to investigate the changes in vascular function between the groups in the three different time points after log-transforming non-parametric variables. To investigate the effects of inflammation C-reactive protein (CRP) and aerobic capacity/fitness (VO2max) on the observed endothelial function differences between the groups, we used generalised estimation equations (GEE). Both VO2max and logCRP were used in all GEE models as predictors of the observed endothelial function changes along with their interaction with the variable group (exercise vs control). All GEE used unstructured correlation matrices. Data were analysed via SPSS V.18.0. Level of significance was set at p<0.05.
Results
The demographic, anthropometric and disease-related characteristics for both groups appear in table 1. No significant differences were detected at baseline in any of the studied variables between the groups (table 1).
Baseline demographic, anthropometric and disease-related characteristics (either in mean±SD or median (IQR)) of the total RA population as well as the exercise and control groups
Cardiorespiratory fitness and disease characteristics
RMANOVA detected a significant change in VO2max over time (p<0.001) in the exercise but not in the control group at 3 (p=0.004) and 6 months (p<0.001) compared with baseline. Disease activity and severity improved significantly in the exercise but not in the control group over time (HAQ: p=0.003, DAS28: p=0.008; logCRP: p=0.047).
Endothelial function
At baseline, Mann–Whitney revealed no significant differences between the exercise and control groups, in any of the endothelial function parameters (all at p>0.05). The median (IQR) as well as all log transformed equivalents appear in table 2.
Median (IQR) and log transformed percentage increases for endothelial function in the exercise and control groups
GEE analyses showed that VO2max was the strongest predictor for the observed changes in microvascular endothelium-dependent function (Ach: B=410.1, p=0.009), whereas logCRP was the strongest predictor for the observed changes over time for microvascular endothelium-independent function (SNP: B=0.061, p=0.017). Furthermore, logCRP and VO2max independently predicted the observed changes in macrovascular endothelium-independent function over time (GTN: VO2max: B=−6.5, p<0.001 and logCRP: B=−4.0, p=0.008).
Discussion
This study demonstrates for the first time that an individualised aerobic and strength training programme significantly improves both microvascular and macrovascular endothelial function in patients with RA. Importantly, Ach and FMD are part of endothelium-dependant responses whereas SNP and GTN are endothelium-independent, so different physiological adaptations and mechanisms may be responsible for the observed changes.
Endothelial-dependent function
Arterial remodelling can be induced by haemodynamic stimuli directly caused by exercise. This is evident for endothelium-dependent (Ach and FMD) improvements due to increased blood flow and shear stress (the frictional force generated by blood flow), resulting in increased long-term nitric oxide bioavailability, the key function in reducing vascular resistance.13 The GEE analyses revealed that the magnitude of improvement in aerobic capacity influenced the observed improvements, at least, in microvascular endothelial-dependent function (Ach). Although this was not the case for macrovascular endothelial-dependent dilatation (FMD), the concomitant exercise-induced improvements in blood pressure and lipid profile observed in the same sample of patients8 have been previously suggested to explain improvements in FMD in patients with diabetes.14
Endothelial-independent function
We found significant improvements in the exercise group for both micro-(SNP) and macro-(GTN) endothelium-independent function, which appeared to be partly moderated by concurrent significant reductions in the inflammatory load (CRP). Research findings may suggest a link between CRP and vascular disease; however, this association seems to be dependent on conventional risk factors.15 Therefore, it remains currently unclear whether CRP is a marker of underlying atherosclerosis or a definitive causal CVD factor. We also found that these beneficial improvements in, at least, macrovascular-independent function (GTN) could have been mediated by the observed improvements in aerobic capacity, which is in line with published studies.16
Exercise training may cause physiological adaptations that have a beneficial impact on important RA-related outcomes.17 ,18 Prescribing exercise to better manage RA may be a challenging task due to the physical disability and pain that accompanies this disease. However, given the multiple benefits of exercise in RA and that CVD comorbidities often remain unnoticed, it seems that exercise should be an integral part of clinical practice in this population.19 ,20
The current design allowed for matching important factors that may have impacted on the studied variables. However, we acknowledge that the optimal approach would be a randomised design and that the original power calculations were not conducted on vascular function but VO2max, which is a more meaningful parameter in relation to CVD. Finally, vascular function assessments may provide mechanistic insights into nitric oxide activity, but their predictive value with regards to CVD risk development is still questionable in RA. As such, our results should be treated with caution.
We conclude that endothelial function in different vascular beds significantly improves as a result of individualised resistance and aerobic exercise training in RA. Further research is required to determine the exact mechanisms behind these phenomena, particularly if exercise-induced reductions in inflammatory markers are indeed responsible for improvements in vascular function.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
-
Contributors All authors included on the paper as coauthors fulfil the criteria of authorship.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Dudley Group NHS Foundation Trust Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.