Article Text

Abstract
Objective To assess the epidemiology of gout and hyperuricaemia in the Italian general population during the years 2005–2009.
Methods Using the Italian primary care database (Health Search/CSD Longitudinal Patient Database), the prevalence, incidence and recurrence rates of gout and/or hyperuricaemia (serum urate level >360 mmol/l (6 mg/dl)) in outpatients aged ≥18 years during the years 2005–2009 were estimated. Rates together with 95% CI were measured overall and stratified by age, gender and calendar year. The characteristics of patients with newly diagnosed gout and hyperuricaemia were investigated and compared with the general population.
Results The prevalence of gout increased from 6.7 per 1000 inhabitants in 2005 to 9.1 per 1000 inhabitants in 2009. It increased with advancing age and was fourfold higher in men. A similar trend was observed for asymptomatic hyperuricaemia (85.4 per 1000 inhabitants in 2005 vs 119.3 per 1000 inhabitants in 2009). The incidence of gout remained stable during the observation years (0.93 per 1000 person years in 2005 vs 0.95 in 2009). Recurrent episode rate was 19.1% during the first year following the first gout attack and 31.6% during the following 5 years. Advanced age, increased levels of uric acid, nephrolithiasis and concomitant use of ciclosporin were the main predictors of recurrence of gout attacks.
Conclusion The prevalence of gout and hyperuricaemia increased in Italy from 2005 to 2009. A high recurrence rate for gout attack was observed during the first year following the first episode. Early management of hyperuricaemia in patients at higher risk of recurrent gout attack should be considered in primary care.
Statistics from Altmetric.com
Background
Gout is a very common type of painful inflammatory arthritis resulting from the deposition of monosodium urate (MSU) crystals within the joints and severely impairing patients' quality of life.1 ,2 Clinically, gout is characterised by an acute onset, an intercritical phase of well-being between two consecutive arthritis episodes and finally by the onset of a chronic form of arthritis. Independent of the clinical phases, a raised level of serum uric acid (sUA), or hyperuricaemia, is the main pathogenic factor in the disease development.3 Hyperuricaemia is commonly defined as sUA >360 mmol/l (6 mg/dl) and may be the result of either urate overproduction or, more frequently, inefficient renal excretion. When the blood urate level reaches its physiological limit of solubility it may crystallise into MSU in the tissue, leading to a gout attack. Although hyperuricaemia is essential for gout occurrence, only about 10% of patients with hyperuricaemia progress to clinical gout during follow-up.4,–,6 Genetic variations7,–,11 and some comorbidities (eg, hypertension, obesity, diabetes mellitus type 2, heart failure) may influence the onset of disease.1 ,12,–,14 Despite the impact of the disease on patients' quality of life, epidemiology data on gout and hyperuricaemia have been lacking until very recently, as evidenced by some authors.15 The latest epidemiological investigations found an increasing trend in the prevalence of gout and hyperuricaemia in several Western countries.1 ,3 ,15,–,19 Using interview-based data, Zhu et al estimated a prevalence of 4% for gout and 21% for hyperuricaemia during the years 2007–2008 in the US general population.20 Another population-based study documented a prevalence of gout of 1.4% in the UK and Germany during the years 2000–2005.21 Moreover, this trend has also been observed in Asian countries, as suggested by two different surveys undertaken in the city of Qingdao in China where the prevalence of gout increased from 3.6/1000 in 2002 to 5.3/1000 in 2004.1 ,22 ,23
Unlike the prevalence, the incidence of gout has been shown to decline slightly in recent years in the UK general population (from 2.67 per 1000 person years (PYs) in 2000 to 2.52 in 2007).1 ,2
To date, no nationwide studies have been conducted in Italy to assess the epidemiology of gout and hyperuricaemia. The aims of this nationwide population-based study are: (1) to assess the prevalence, incidence and recurrence of gout and hyperuricaemia in the Italian general population during the years 2005–2009; and (2) to characterise patients with gout and/or hyperuricaemia in the same setting.
Methods
Data source
Data were extracted from the Health Search/CSD Longitudinal Patient Database (HSD). HSD is a longitudinal observational database that is representative of the general Italian population. It was established in 1998 by the Italian College of General Practitioners and, at the time the study was conducted, it contained data from computer-based patient records from more than 650 general practitioners (GPs) throughout Italy, covering a total population of around one million patients. The database includes information about patient demographics and medical data such as clinical events and diagnoses (as free text or coded using International Classification of Diseases, 9th Revision, Clinical Modification-ICD9-CM), hospital admissions, laboratory test values, prescriptions of drugs (coded using Anatomical Therapeutic Chemical (ATC) classification system) used in treating gout or drugs related to increased sUA levels and death. HSD complies with European Union guidelines on the use of medical data for research and has been previously demonstrated to be a valid data source for scientific research.24 ,25
Study population
For this analysis we selected from HSD all subjects aged ≥18 years who were alive, registered in the lists of participating GPs at the beginning of the study period (1 January 2005 to 31 December 2009) and with at least 2 years of recorded history prior to the start of the study.
Outcome definition
Outcomes of the study were gout and hyperuricaemia. Gout was identified using specific ICD 9-CM codes and related key words for free text search (274.0: gouty arthritis; 274.1: gouty nephropathy; 274.8: gout with other unspecified manifestations; 274.9: gout). Hyperuricaemia was identified using both diagnostic codes and related key words (274.9: hyperuricaemia) as well as considering annual average levels of sUA >360 mmol/l (6 mg/dl) in both genders. Analysis of the recurrence of episodes of gout and the estimated time between the diagnosis of hyperuricaemia and the onset of the first attack of gout was done only for newly diagnosed patients in the years 2005–2008. The first attack of gout was identified as the first ever registered diagnosis of gout (identified using the abovementioned criteria) in the database.
Starting from the first diagnosis of gout, the average annual number of acute attacks and the cumulative risk of occurrence of acute attacks during the first year and the entire follow-up period were calculated.
Data analysis
The prevalence and incidence of gout and hyperuricaemia during the years 2005–2009 were calculated. Regarding the yearly prevalence, for each observation year the number of patients with old and new diagnoses of gout/hyperuricaemia, alive and present in the GPs' lists up to 31 December of the year (numerator) was divided by the total number of patients alive and active in the same year (denominator). Regarding the yearly incidence, the number of new cases in each year of observation (numerator) was divided by the person-time at risk of developing gout/hyperuricaemia (denominator) at 1 January of each year of observation. For calculation of the incidence rate, person-time of follow-up was censored upon the first occurrence of one of the following events: occurrence of gout/hyperuricaemia, transferring out of general practice or death.
The incidence and prevalence were expressed as rates per 1000 PYs and 1000 inhabitants, respectively, together with 95% CI.
To characterise the patients with a new diagnosis of gout/hyperuricaemia, the presence of the following covariates was evaluated at the date of first diagnosis of gout/hyperuricaemia (ie, index date): (1) demographic data (age, sex, geographical area of residence); (2) comorbidities (hypertension, dyslipidaemia, type 2 diabetes mellitus, coronary artery disease, cerebrovascular disease, congestive heart failure, renal and ureteral calculi, renal colic); (3) concomitant use (6 months before the index date) of drugs that can either directly increase the sUA level (ie, diuretics, salicylates, broad-spectrum penicillins) or interfere with urate-lowering therapy with allopurinol (ie, oral anticoagulants, imidazole derivatives, ciclosporin and levodopa)12 ,13 ,26,–,29; (4) laboratory test values (uric acid, creatinine, glycaemia, total/low density lipoprotein and high density lipoprotein cholesterol) and body mass index (BMI; underweight <18.5 kg/m2; normal weight 18.5–24.9 kg/m2; overweight 25–29.9 kg/m2; obesity ≥30 kg/m2) as the last value recorded within 5 years prior to the index date.
Results
During the observation period there was an increase in the prevalence of gout from 6.7/1000 inhabitants in 2005 to 9.1/1000 inhabitants in 2009 (figure 1). With regard to hyperuricaemia, a much higher overall prevalence was found than for gout. A significantly increasing trend in prevalence over the years was also found for hyperuricaemia (85.4/1000 inhabitants in 2005 vs 119.3/1000 inhabitants in 2009), as shown in figure 2. Considering 7 mg/dl as the cut-off value, the average prevalence of hyperuricaemia would be reduced by more than 40% (68.9/1000 inhabitants in 2009).

Prevalence of gout per 1000 inhabitants by gender and calendar year.

Prevalence of hyperuricaemia (serum uric acid >6 mg/dl) per 1000 inhabitants by gender and calendar year.
The prevalence of gout and hyperuricaemia was higher in men than in women (4/1 for gout and 2/1 for hyperuricaemia) and increased with advancing age (figure 3). During the study period the prevalence of gout and hyperuricaemia appeared to be always slightly higher in northern Italy than in central and southern Italy—for example, in 2009 the prevalence of gout was 9.3 vs 8.6 vs 9.0 per 1000 inhabitants in northern, central and southern Italy, respectively, and the prevalence of hyperuricaemia was 125.5 vs 120.3 vs 111.1 per 1000 inhabitants, respectively, considering 6 mg/dl as the cut-off value (data not shown).
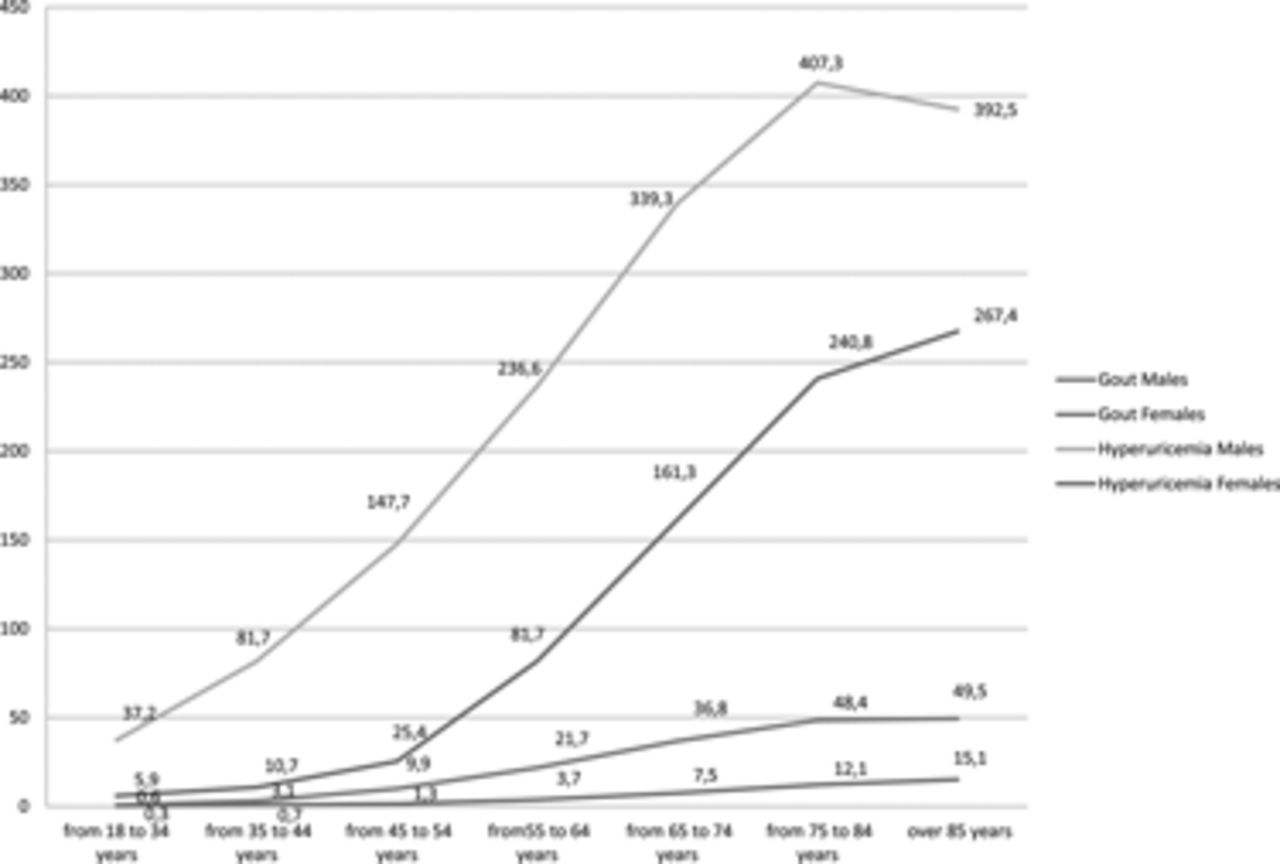
Prevalence of gout and hyperuricaemia (serum uric acid >6 mg/dl) per 1000 inhabitants by gender and age groups in 2009.
The incidence of gout appeared to be fairly stable from 2005 to 2009, ranging from 0.93 per 1000 PYs in 2005 to 0.95 per 1000 PYs in 2009 (figure 4). The incidence of gout was higher in men and in older people. On the other hand, the incidence of hyperuricaemia declined from 16.4 per 1000 PYs in 2005 to 15.1 per 1000 PYs in 2009 (figure 4). Considering 7 mg/dl as the cut-off point, the average value of the incidence of hyperuricaemia would be reduced by more than 40% compared with the estimate using 6 mg/dl as the cut-off value, similar to that observed for the prevalence (8.8 per 1000 PYs vs 15.1 per 1000 PYs in 2009; data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
One-year incidence of gout and hyperuricaemia (serum uric acid >6 mg/dl) per 1000 person years by gender and calendar year.
Age-standardised and gender-stratified prevalence and incidence of gout and hyperuricaemia are reported in annexes S1–S4 in the online supplement.
The demographic and clinical characteristics of patients with a new diagnosis of gout are shown in table 1. Patients with gout were compared with a non-gout control group matched for age, gender and practice/geographical region in the ratio of one case to three controls to analyse the prevalence of comorbidity and identify the risk factors of gout.
Demographic and clinical characteristics of patients with a new diagnosis of gout and non-gout control group
Patients with incident gout are more likely to be men and aged >65 years. A larger proportion of these patients also have cardiovascular diseases (eg, 64.2% had hypertension) and other metabolic disorders (eg, 25.3% had dyslipidaemia, 17.1% had type 2 diabetes mellitus, 7.2% had obesity). Interestingly, 24.3% of the patients with gout were treated with diuretics within 6 months prior to the date of the first diagnosis. This proportion did not change within 6 months after the diagnosis. At the time of incident diagnosis of gout, 19.2% of patients had serum urate levels ≥9 mg/dl.
The characteristics of patients with a new diagnosis of hyperuricaemia were comparable (data not shown).
On average, the first gout attack occurred 13.7±14.1 months after the incident diagnosis of hyperuricaemia, and even earlier in women (11.4±13.2 months) or in the presence of a serum urate level >9 mg/dl (8.9±11.9 months).
Among 3069 patients with incident gout, 19.1% (n=576) experienced a recurrent gout attack within 1 year of the first gout diagnosis (table 2). This proportion increased up to 31.6% when the entire follow-up period (average of 5 years) was considered. On average, a mean (SD) of 1.5 (0.9) and 2.4 (1.8) episodes of recurrent gout attacks were reported in patients with newly diagnosed gout during the first year and in the entire follow-up period, respectively. Women and patients aged <45 years were less likely to have a recurrent gout attack both during the first year after incident gout diagnosis (table 2) and the entire follow-up period (p<0.05).
Analysis of gout recurrences in first year of follow-up in patients with an incident diagnosis of gout
The highest rate of recurrent gout attack was documented for patients with renal colic, nephrolithiasis and obesity, and those treated with ciclosporin. Moreover, the risk of recurrent gout attack increases linearly with higher serum urate levels. As shown in table 2, more than 20% of patients with newly diagnosed gout had a recurrence of gout within 1 year after the diagnosis despite receiving at least one allopurinol prescription.
Discussion
To our knowledge, this is the first nationwide epidemiological investigation of gout and hyperuricaemia in the Italian general population.
We found that the prevalence of gout increased during the study years from 0.7% in 2005 to 0.9% in 2009, with a male/female ratio of 4:1. In general our results are substantially in line with previous investigations that observed an increased trend of gout prevalence over time as well as a higher prevalence in men and older people.1 ,30 ,31 In particular, in our study we observed a yearly increase in the prevalence of gout by, on average, 6 per 10 000 inhabitants in Italy compared with an average yearly increase of about 9 per 10 000 inhabitants from 1999 to 2005 in the US general population.20 No increase was documented in the UK from 1999 to 2005.21 ,32
The gradual increase in the prevalence of gout/hyperuricaemia, as observed in this study and others, may be related to the increased prevalence of overweight and obesity33 as well as the increased consumption of foods rich in purines,34 ,35 alcoholic consumption (eg, liquors and beer) and soft drinks sweetened with fructose.36,–,38 Higher adiposity and weight gain are strong risk factors for gout, while weight loss is protective. It is likely that a higher level of BMI increases the risk of gout by increasing sUA levels. Hyperuricaemia has been associated with obesity via both increased production and decreased renal excretion of urate. In our study we found that the risk of gout increased with increasing BMI. In particular, among patients with a BMI ≥25 kg/m2, an incidence of gout of about 70% was found.
Another main finding of this study is that the overall prevalence of gout in Italy is remarkably lower than that reported in previous population-based investigations from the USA (3.9% in 2007–2008),1 ,20 UK and Germany (both 1.4% in 2000–2005),21 Taiwan (self-reported: 8.2% in men and 2.3% in women in 2005–2008)30 and New Zealand (2.7% in 2009),39 while it is higher than that observed in a Chinese study based on self-reported diagnosis (0.36% in 2002).23
Apart from different study years and methodology for gout identification, the discrepancy in the prevalence of gout between our study and others may be related to country-specific diet, in particular meat consumption, which is a known risk factor for hyperuricaemia.34
With regard to the prevalence of gout, meat consumption has continued to rise in the USA35 and is always much greater than in Europe. In general, the Mediterranean diet, which is largely adopted in Italy, may account for a protective effect in the risk of gout/hyperuricaemia in Italy compared with the USA and other European countries. The Mediterranean dietary pattern consists mainly of high consumption of fruits, vegetables and olive oil as the principal source of fat as well as low consumption of meat and alcohol beverages such as beer and liquors.40 Together, this diet is associated with a low level of serum urate,41 thus lowering the risk of gout. Interestingly, the prevalence of gout and, to a lesser extent, of hyperuricaemia is quite different across Italian geographical areas, with higher figures observed in northern Italy. This finding is likely to be attributed to different dietary habits as the adherence to the Mediterranean diet is higher in central and southern Italy than in northern Italy.
Differences in the use of urate-lowering agents and drugs potentially increasing sUA as well as genetic variations may contribute to the observed differences in the prevalence of gout and hyperuricaemia across countries. In particular, polymorphisms of the gene SLC2A9, encoding for the proximal tubule transporter of uric acid GLUT9, may play a major role in raising the sUA level, thus increasing the risk of prevalence of gout and hyperuricaemia.7,–,11 ,42
Our study confirms that ciclosporin is a risk factor for gout;43 particular caution should be observed in patients with hyperuricaemia requiring the use of this drug.
In addition, around 25% of patients with a new diagnosis of gout/hyperuricaemia received prescriptions for either diuretics or salicylates within the 6 months prior to the diagnosis. It is well known that these drugs may increase sUA levels.13 ,27 Physicians should therefore verify at the time of a new diagnosis of gout/hyperuricaemia whether the patient is being treated with these drugs and re-evaluate the need for such therapies.44
Regarding gout flares, in the first year following the new diagnosis of gout 19.1% of patients had relapses of articular acute attacks with a decreasing trend in the following period. Moreover, as previously reported,20 in our population sUA levels were also strongly correlated with the frequency of gout flares. This is a further demonstration that the early lowering of sUA below 6 mg/dl is recommended to prevent the recurrence of the disease.
Our results strengthen further the relationship between gout and hyperuricaemia. We observed an increasing trend of prevalence for gout and also for hyperuricaemia during the same years (8.5% in 2005 vs 11.9% in 2009). Uricaemia increased with advancing age and was higher in men than in women, but to a lower extent (2:1) than for gout. As for gout, the prevalence of hyperuricaemia in Italian people was lower than in other countries; other epidemiological data showed an estimated prevalence of hyperuricaemia of 21% in the US general population20 while population-based Chinese studies reported a prevalence ranging from 13% to 25%,1 ,22 which is higher than our estimates (9.1% in 2009). Together these data suggest that Italian dietary habits may play a primary protective role in the determinism of hyperuricaemia.
Another study finding is that the incidence of gout remained relatively stable during the observation years 2005–2008, in line with two English studies conducted throughout the 1990s and 2000s.2 ,32
Finally, we found that the most frequently reported comorbidities in patients with a diagnosis of gout/hyperuricaemia was hypertension and, to a lesser extent, metabolic diseases (eg, diabetes mellitus and obesity), which were more commonly reported in the UK (obesity) and Germany (type 2 diabetes mellitus).21
Some limitations of the study should be mentioned. First, the diagnostic criteria could represent a possible selection bias; the gold standard for diagnosing gout is the identification of MSU monohydrate crystals in synovial fluid during the acute attack.6 Although important, these data are lacking in our study as well as in all the other abovementioned epidemiological studies. Moreover, uricaemia is not routinely evaluated in all patients in clinical practice so a discrete number of hyperuricaemic and asymptomatic patients could be lost. Despite this, we think that our study may be of interest as it is the first study to try to assess the nationwide epidemiology of gout and hyperuricaemia in Italy.
With respect to gout flares, an underestimation of the rates cannot be ruled out as patients (especially those with mild symptomatology) may use self-medication without presentation to a primary care physician.
In conclusion, we found that the prevalence of gout increased in Italy from 2005 to 2009 while the incidence remained fairly stable during the same period. The trend for hyperuricaemia was similar to that of gout, confirming the close relationship between these entities. An increased serum urate level appears to influence the recurrence of gout attacks.
Early and effective management of hyperuricaemia, especially in patients found to be at higher risk, may prevent both short-term and long-term gout attacks.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.