Article Text

Abstract
Background Studies examining the relationship between serological status (rheumatoid factor and/or anticitrullinated antibody) and rituximab treatment outcome in rheumatoid arthritis (RA) have been hampered by limited numbers of seronegative patients.
Objective To carry out a meta-analysis of trials from the rituximab RA clinical programme to investigate this relationship further.
Methods This was a meta-analysis of four placebo-controlled, phase II or III clinical trials. The efficacy end point in all analyses was change from baseline in Disease Activity Score in 28 joints-erythrocyte sedimentation rate (DAS28-ESR) at 24 weeks. Assay of serotype and missing data imputation methods were consistent across all studies.
Results The population analysed comprised 2177 patients (rituximab, n=1416; placebo, n=761). Demographics and baseline disease characteristics were well balanced. When a fixed-effects meta-analysis approach was used, the overall-effect model indicated evidence of additional treatment benefit with rituximab in seropositive patients: reduction in DAS28-ESR at week 24 was on average 0.35 units (95% CI 0.12 to 0.84; n=1394) greater than in seronegative patients; this effect was not seen in placebo patients. Heterogeneity indices indicated significant uncertainty in the overall-effect model (Q=8.8, I=0.77; p=0.03 (χ2 test)). Baseline Health Assessment Questionnaire score, pain visual analogue scale, swollen joint counts of 28 joints and race were significant contributors to this heterogeneity, with additional analysis indicating that these effects may predominate in early RA (methotrexate-naïve) populations. A dominant effect was seen in patients for whom one or more tumour necrosis factor inhibitors had failed.
Conclusion Although the difference was modest, the overall-effect model indicates that seropositive patients respond better to rituximab than seronegative patients.
Statistics from Altmetric.com
Introduction
Although biological disease-modifying antirheumatic drugs (DMARDs) have revolutionised the treatment of patients with rheumatoid arthritis (RA), an inadequate response to these agents is achieved in a substantial proportion of patients. The identification of biomarkers capable of predicting responsiveness to different classes of biological DMARD in individual patients is therefore the focus of a great deal of research. A wide range of candidate biomarkers have been investigated.1,–,3 A number of studies have investigated the association between rheumatoid factor (RF) and/or anticitrullinated peptide antibody (ACPA) status and clinical response to biological DMARDs.4,–,8 In the case of rituximab, data from double-blind, placebo-controlled, multicentre trials have so far provided some evidence that, while clinical benefit is seen in patients seronegative for both RF and ACPA, there is an improved probability of clinical benefit in patients positive for one or both of these factors.4 ,5 ,9,–,12 These findings are supported by results from a recent multicentre study conducted in France,13 from smaller, observational studies14 and from the CERERRA collaboration.15
Analysis of the REFLEX trial, conducted in patients with an inadequate response to tumour necrosis factor (TNF) inhibitors (TNF-IR), supported the premise that seropositive patients had an improved probability of achieving American College of Rheumatology (ACR) responses to rituximab treatment in comparison with seronegative patients.4 ,5 ,10 However, formal testing did not provide evidence that the treatment effect was dependent upon baseline RF status. In the SERENE trial (methotrexate (MTX)-inadequate responder (MTX-IR) patients), the reductions in Disease Activity Score in 28 joints-erythrocyte sedimentation rate (DAS28-ESR) seen with rituximab over time were generally greater in seropositive than in seronegative patients,12 whereas in DANCER (TNF-IR and DMARD-IR patients), results were inconclusive.11 Most recently, analysis of MTX-naïve patients with active RA in the IMAGE trial showed numerically increased response rates in categorical end points, and improved disease activity with rituximab plus MTX in seropositive relative to seronegative patients.9
Common to REFLEX, SERENE, DANCER and IMAGE are the relatively low numbers of seronegative patients included in the trials, a feature that has so far challenged a formal statistical interpretation of treatment effect in seropositive compared with seronegative patients. Pooling strategies across trials can be employed to generate improved statistical power and therefore better estimate effect size, although characteristics of individual studies may drive ‘cross-trial’ heterogeneity. A previous retrospective pooled analysis of DMARD-IR patient populations from MIRROR16 and SERENE12 showed that, after completion of the first rituximab treatment course at 24 weeks, significantly more seropositive than seronegative patients achieved ACR20 and ACR50 responses; seropositive patients were also significantly more likely to achieve ACR20/50/70 responses and DAS low disease activity after the second course of treatment at 48 weeks.17 However, the MIRROR study was not placebo controlled and, as a result, it was not possible to exclude a prognostic behaviour of serotype in this analysis.
Our study is a retrospective meta-analysis of four double-blind, placebo-controlled, multicentre trials from the rituximab development programme. The aim was to estimate formally a global index across trials of the effect of serotype on treatment outcome to rituximab and to compare this with placebo. Further, an individual patient data (IPD) meta-analysis was employed to identify potential sources of variability among baseline clinical variables that might explain any heterogeneity in this relationship.
Methods
Trial selection
This was a retrospective analysis of four double-blind, placebo-controlled randomised trials (IMAGE, DANCER, SERENE and REFLEX) from the rituximab RA clinical trial programme. Full details of the individual study methodologies have been published previously.9,–,12 In brief, the four trials used similar inclusion criteria: a diagnosis of RA according to the 1987 ACR criteria for the classification of RA; disease duration ≥6 months (≥8 weeks in IMAGE); swollen joint count (SJC)≥8 (66-joint count) and tender joint count≥8 (68-joint count) at screening and baseline; ESR≥28 mm/h or C-reactive protein≥0.6 mg/dl (SERENE), ≥1.0 mg/dl (IMAGE) or ≥1.5 mg/dl (DANCER and REFLEX). With the exception of IMAGE, all patients were receiving MTX 10–25 mg/week at a stable dose. In addition, patients in IMAGE who were seronegative for RF required radiographic evidence of erosive damage attributable to RA. Prior treatment history was used to stratify eligibility for the individual trials. IMAGE required patients to be MTX-naïve,9 while SERENE was conducted in MTX-IR patients who had no prior biological treatment for RA.12 REFLEX recruited TNF-IR patients,10 and DANCER permitted a mixed population of patients who had a lack or loss of response to treatment with DMARDs and/or biological agents.11
In all studies, patients received rituximab or placebo by intravenous infusion on days 1 and 15 at doses of 2×500 mg or 2×1000 mg. All infusions of rituximab were premedicated using 100 mg intravenously methylprednisolone and all subjects received rituximab or placebo in combination with MTX, with patients in IMAGE initiating MTX during the study. All studies were conducted in accordance with the ethical principles of the Declaration of Helsinki.
Serological status for RF (positive >20 IU/ml) and ACPA (positive >5 U/ml, Diastat, Axis-Shield) was determined at baseline in all studies. As patients who were positive for only RF or ACPA comprised a relatively small proportion of the total seropositive population, results are presented for a pooled seropositive population (RF+ and/or ACPA+).
Statistical analysis
Efficacy end point and covariates
Change from baseline in DAS28-ESR at week 24 was used as the efficacy end point in all analyses presented. Baseline DAS and geographical region (USA vs non-USA) were included as covariates in all analyses. A consistent data imputation method was used across all studies. Missing joint counts were imputed using the last observation carried forward method. The DAS score was set to missing if the other components were missing. Analyses using DAS in patients with only complete observations yielded similar results. Other end points, such as ACR20 and ACR50, were also analysed using logistic regression but these results are not presented. Overall, the effects were found to be in the same direction but with larger uncertainty, owing to the reduced sensitivity of the binary compared with the continuous end points. In all meta-analyses, data from the two rituximab doses (2×500 mg and 2×1000 mg) were pooled as the efficacy results were comparable between the doses.
Analysis by treatment group
In the overall interpretation of the results, it was necessary to compare the rituximab and placebo groups in order to understand whether serotype was predictive of treatment benefit (with a larger effect seen in the rituximab group) or prognostic (with similar effects in both groups). However, the single-effect size measure for treatment–biomarker interaction is not transparent, and not intuitive to interpretation. In addition, the test for interaction has lower power. Therefore, summary data and IPD meta-analyses were conducted within both treatment groups in order to provide a clear interpretation of the predictive versus the prognostic effect.
Summary level meta-analysis
The effect of serotype, with CI, was obtained for each study using a linear regression model conducted separately in the rituximab and placebo groups. Serotype effects were expressed as least square means, adjusting for the covariates. A meta-analysis of summary data was performed using a fixed-effect model. Each study was weighted using the inverse of the variance of the serotype effect. Cochran's Q and I2 were obtained as measures of heterogeneity. Overall serotype effects for the rituximab and placebo groups were obtained. Analyses were performed using R (version 2.10.1).
Analysis of heterogeneity
The contribution of specific variables, including demographic variables, baseline disease characteristics and baseline biomarker values (see online supplementary table 1) to the heterogeneity of the serotype effect was investigated using two methods: (1) weighted regression of the study level serotype effect against the mean value for the covariates for that study. Each study was weighted by the inverse of the variance of the serotype effect size estimate. R2 and p values were obtained. (2) IPD fixed-effect meta-regression of change in DAS from baseline DAS, region, study and serotype, covariate, and serotype and covariate interaction. Separate residual variance for each study was allowed. Restricted maximum likelihood estimates were obtained using SAS Proc Mixed procedures (SAS-STAT version 9.2).
Demographics of patients with known serological status in the REFLEX, DANCER, SERENE and IMAGE trials Data are means (standard deviation) unless stated.
For continuous variables and categorical variables with more than two categories, appropriate transformation or binning of the variables was assessed. For example, if a continuous variable had a highly skewed distribution, log transformation might have been required in order to reduce the effect of the tail and far outliers.
Variables that demonstrated significant interaction with serotype (R2>0.6 in the first analysis or p<0.05 in the second analysis) were further investigated using subgroup analysis, where the subgroups were defined based on stratification around the median of the variable. No threshold tuning was undertaken.
Results
A total of 2177 patients (rituximab, n=1416; placebo, n=761) from the four trials had known RF and ACPA status. The proportion of patients who were seropositive was similar in the placebo (89.5% (681/761)) and rituximab (88.5% (1253/1416)) groups and across the four trials (85.3–90.9%) (table 1). Overall, 2139 patients (rituximab, n=1394; placebo, n=745) had the requisite clinical outcome data at 24 weeks and were included in the meta-analysis. Population demographics and baseline disease characteristics were well balanced between seropositive (RF- and/or ACPA-positive) and seronegative (RF- and ACPA-negative) groups within each trial (table 1).
Meta-analysis of the overall effect of serotype on rituximab and placebo DAS28-ESR outcome
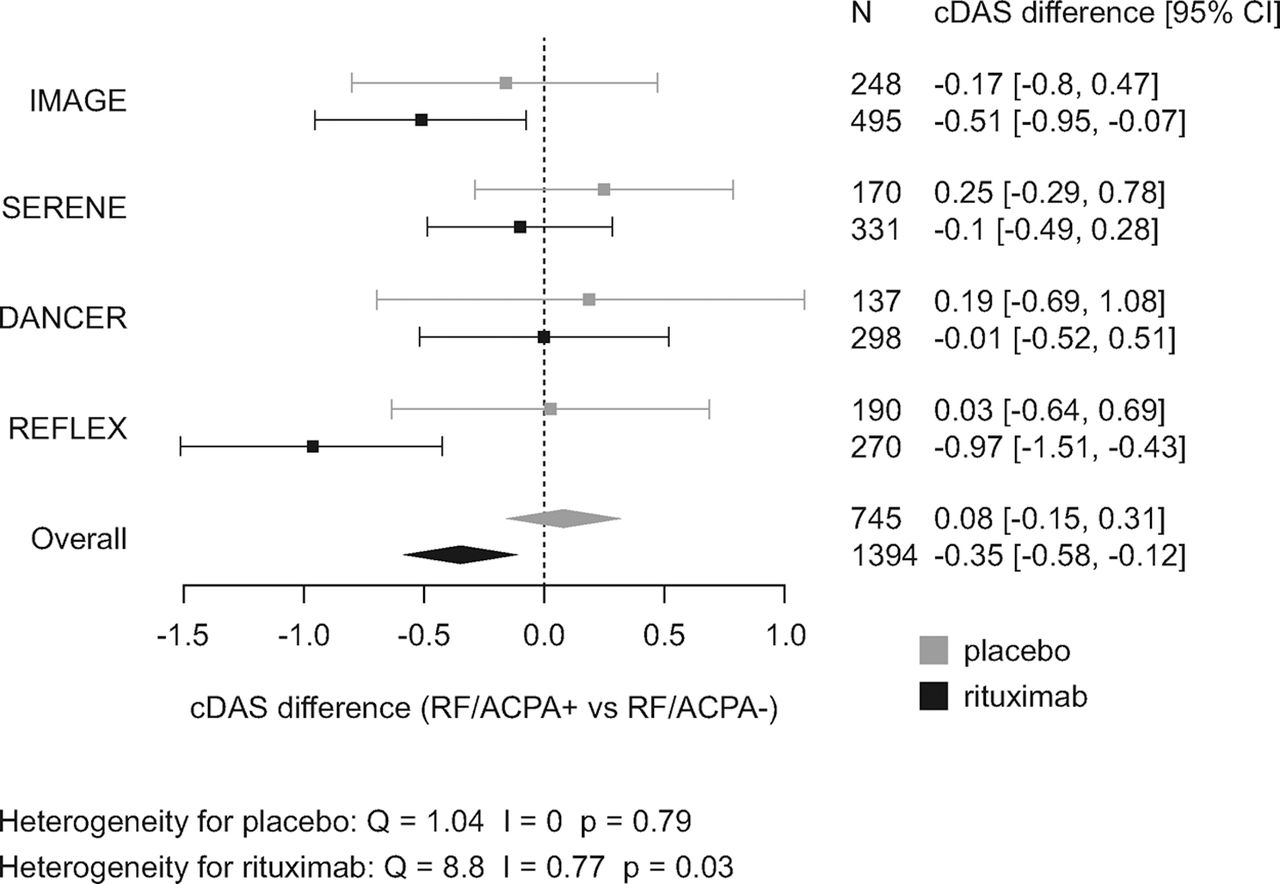
After applying common definitions of serotype and methods of data imputation for clinical outcome, the overall effect of serotype on DAS28-ESR was significant in the rituximab but not the placebo group (figure 1). In the rituximab group, seropositive patients experienced an additional mean reduction in DAS28-ESR of 0.35 units (95% CI 0.12 to 0.58) at week 24 compared with seronegative patients. This effect was not seen in placebo patients. There was no evidence of a relationship between titre of RF or ACPA and the magnitude of the reduction in DAS28-ESR (supplementary figure 1). Furthermore, we could not demonstrate a dominant influence of either RF or ACPA individually on treatment response. RF-positive patients experienced an additional mean reduction in DAS28-ESR over 24 weeks of 0.32 units (95% CI 0.13 to 0.50) compared with RF-negative patients while the corresponding improvement in ACPA-positive patients was 0.24 units (95% CI 0.04 to 0.45) (see supplementary figure 2). When other end points, including ACR20 and ACR50, were analysed, the overall results were similar (supplementary figure 3). In general, dichotomised response end points capture less information than continuous end points. As a result, the CI remained large despite the meta-analysis approach.

Effect of serotype and treatment on change in DAS28-ESR. The plot displays the numerical difference between the change in DAS28-ESR for ACPA and/or RF seropositive patients compared with seronegative patients treated with rituximab or placebo for 24 weeks. Data are presented for rituximab individual double-blind, placebo-controlled trials and an overall meta-analysis model as least-square means ± 95% CI. Meta-analysis of summary data was performed using a fixed-effect model and the study weighted by inverse of the variance. Measure of heterogeneity is Cochran's Q, I2 and test of heterogeneity is Cochran's χ2 test. ACPA, anticitrullinated peptide antibody; cDAS, difference in the change in disease activity in 28-joint score between seronegative and seropositive patients; DAS28, disease activity in 28 joints; ESR, erythrocyte sedimentation rate; RF, rheumatoid factor.

Interaction of baseline HAQ status, serotype and treatment on change in DAS28-ESR. The plot displays the numerical difference between the change in DAS28-ESR for ACPA and/or RF seropositive patients compared with seronegative patients treated with rituximab or placebo for 24 weeks. Patient populations were stratified by median baseline HAQ status (high >1.75; low ≤1.75). Data are presented for rituximab individual double-blind, placebo-controlled trials and an overall meta-analysis model as least-square means ± 95% CI. Meta-analysis of summary data was performed using a fixed-effect model and the study weighted by inverse of the variance. ACPA, anticitrullinated peptide antibody; cDAS, difference in the change in disease activity in 28-joint score between seronegative and seropositive patients; DAS28, disease activity in 28 joints; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire; RF, rheumatoid factor.
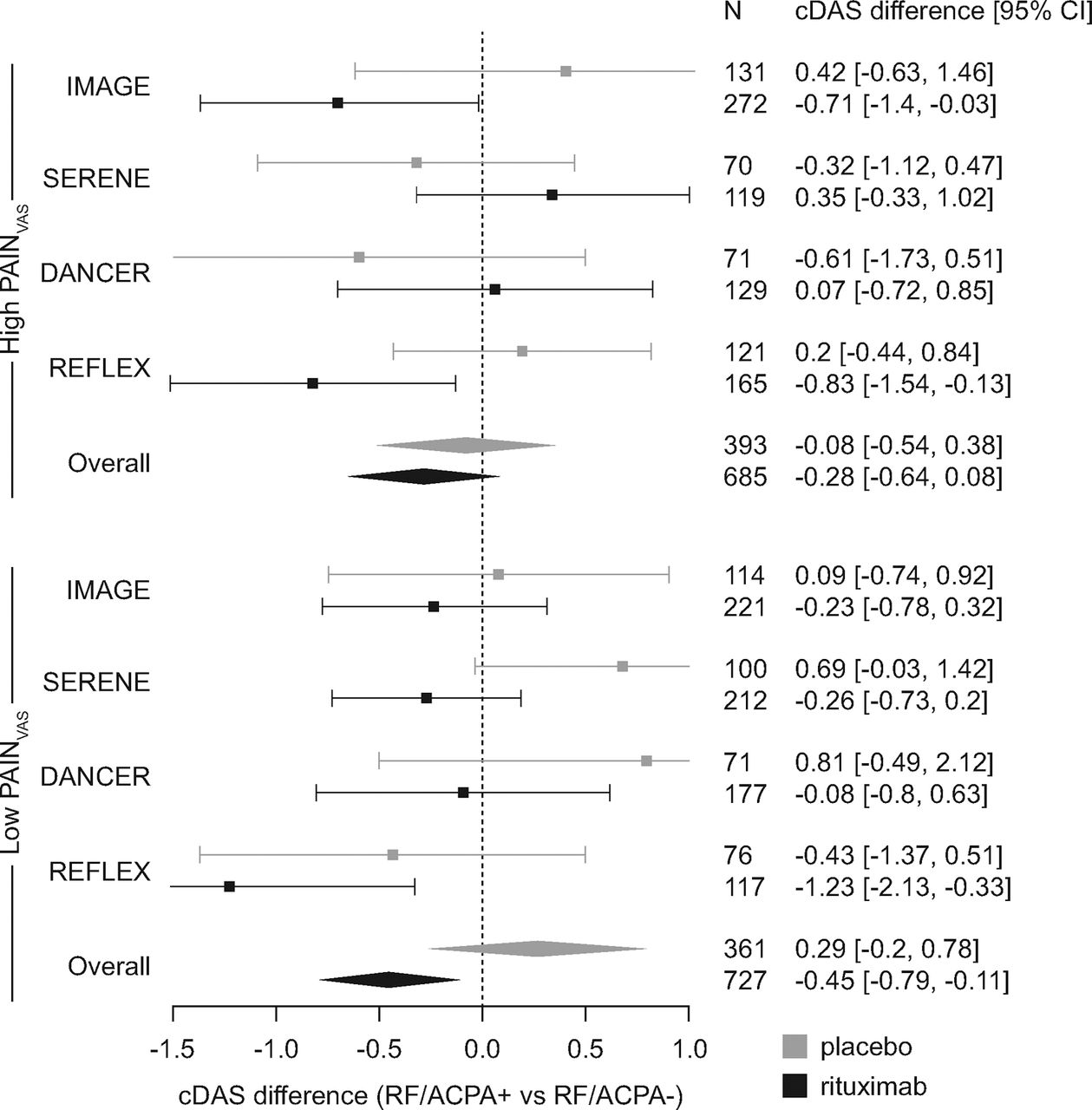
Interaction of baseline pain, serotype and treatment on change in DAS28-ESR. The plot displays the numerical difference between the change in DAS28-ESR for ACPA and/or RF seropositive patients compared with seronegative patients treated with rituximab or placebo for 24 weeks. Patient populations were stratified by median baseline pain score (VAS) (high >63 mm; low ≤63 mm). Data are presented for rituximab individual double-blind, placebo-controlled trials and an overall meta-analysis model as least-square means ± 95% CI. Meta-analysis of summary data was performed using a fixed-effect model and the study weighted by inverse of the variance. ACPA, anticitrullinated peptide antibody; cDAS, difference in the change in disease activity in 28-joint score between seronegative and seropositive patients; DAS28, disease activity in 28 joints; ESR, erythrocyte sedimentation rate; RF, rheumatoid factor; VAS, visual analogue scale.
There was evidence of heterogeneity in the serotype effect in rituximab-treated subjects across studies (figure 1). For rituximab, the dominant effect of serotype was seen in TNF-IR patients from the REFLEX trial, with a mean difference in change in DAS28-ESR between seropositive and seronegative patients of 0.97 DAS units. In contrast, there was a smaller effect of serotype on rituximab treatment outcome in IMAGE, and no effect in DANCER and SERENE based on the current analysis of change in DAS28-ESR. Of note, a previous exploratory analysis of serotype on treatment outcome in DANCER found a numerically higher ACR20 response rate for placebo versus rituximab in seronegative patients, although this analysis was confounded by an unusually high placebo response (52% vs 48% in the rituximab group) and a relatively small sample size (21 and 63 patients, respectively). As outlined in the ‘Introduction’, the limited number of seronegative patients (particularly in the placebo groups) underpins the wide CI observed for the individual trials.
Calculation of heterogeneity indices indicated that there was significant uncertainty in the overall-effect model for rituximab (Q=8.8, I=0.77; p=0.03 (χ2 test)) (figure 1).
Meta-regression of serotype on rituximab DAS28-ESR outcome
In order to better understand the source of heterogeneity in the overall-effect model, meta-regression analyses were conducted using the covariates listed in supplementary table 1. Only covariates with data available for all trials were included in these analyses.
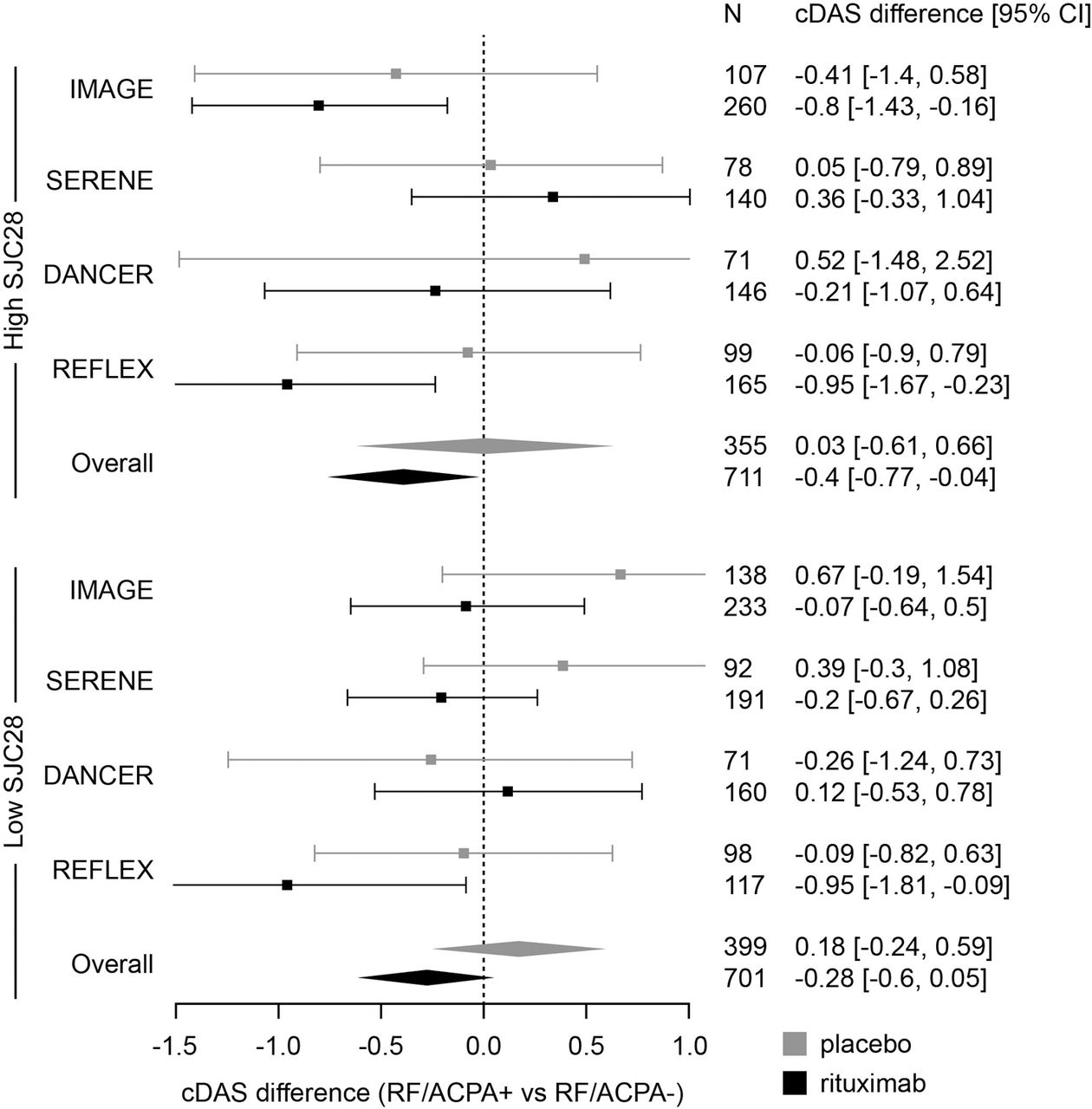
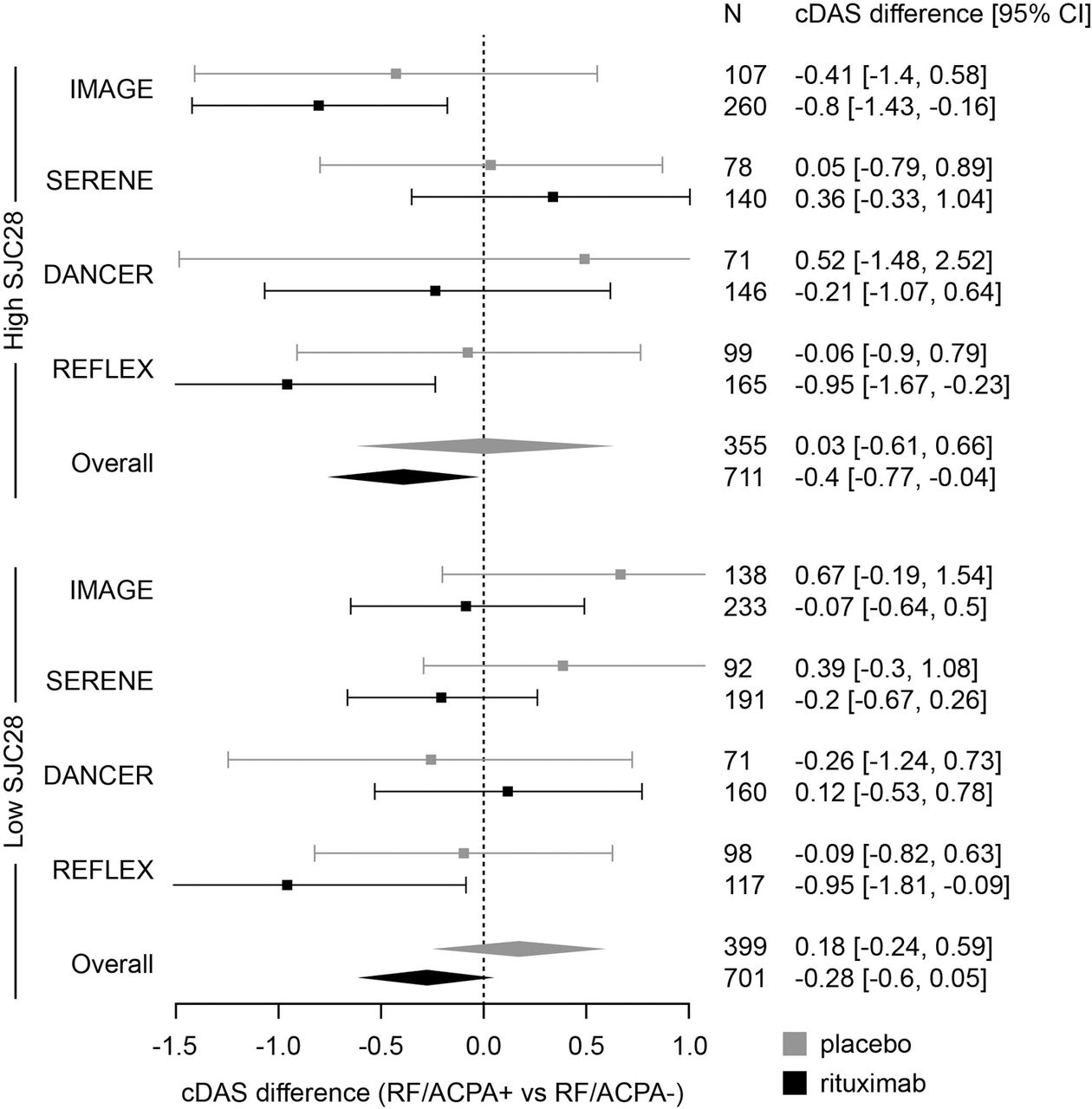
Results indicated that baseline scores for Health Assessment Questionnaire (HAQ), pain visual analogue scale and SJC, and race might interact with the serotype effect among rituximab-treated patients. To investigate these interactions further, patients were stratified according to the median of each variable. The results of these analyses with respect to HAQ, pain and SJC are shown in Forest plots (figures 2–4, respectively). In some individual studies, the variable may modify the effect of serotype. For example, seropositive patients in the early RA study (IMAGE) with high baseline HAQ score (>1.75), pain visual analogue scale or SJC experience improved benefit with rituximab treatment, whereas seropositive patients with low baseline levels of these parameters do not (figures 2–4). These observations are not replicated in the DMARD-IR studies (SERENE or DANCER). Examining the meta-analysis result and the trends across the individual studies, it is clear that heterogeneity was not improved in either the low or high baseline HAQ, pain or SJC subgroups (figures 2–4). Further analysis within the Caucasian subgroup yielded similar results to that of the whole treatment population, indicating that the heterogeneity could not be explained by race (data not shown).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interaction of baseline swollen joint count, serotype and treatment on change in DAS28-ESR. The plot displays the numerical difference between the change in DAS28-ESR for ACPA and/or RF seropositive patients compared with seronegative patients treated with rituximab or placebo for 24 weeks. Patient populations were stratified by median 28-swollen joint count (high >13; low ≤13). Data are presented for rituximab individual double-blind, placebo-controlled trials and an overall meta-analysis model as least-square means ± 95% CI. Meta-analysis of summary data was performed using a fixed-effect model and the study weighted by inverse of the variance. ACPA, anticitrullinated peptide antibody; cDAS, difference in the change in disease activity in 28-joint score between seronegative and seropositive patients; DAS28, disease activity in 28 joints; ESR, erythrocyte sedimentation rate; RF, rheumatoid factor; SJC, swollen joint count.
Discussion
This study represents the largest, placebo-controlled evaluation of the effect of serotype on clinical effectiveness of rituximab in RA. A total of 2177 patients were available for the analyses, a similar number to a recently published observational study of the clinical effectiveness of rituximab in seropositive patients from the CERERRA collaboration.15
Our study employed a fixed-effect model of meta-analysis to estimate the influence of RF and ACPA serotype on treatment outcomes to placebo or rituximab across multiple lines of treatment (MTX-naïve, DMARD-IR and TNF-IR). Furthermore, using regression analysis, the study explored how additional patient covariates might explain any heterogeneity in the interaction between serotype and clinical outcome to rituximab at both the overall effect level and also in individual studies.
Although the effects are modest, the key findings from our study indicate that in the overall model of serotype effect on treatment outcome, seropositive patients respond better to rituximab than seronegative patients. The serotype effect is not uniform across different populations. The largest effect was seen in patients for whom at least one TNF inhibitor had failed. Although exploration of additional patient baseline covariates yielded no insight to explain the overall heterogeneity of the data, there was an indication that in MTX-naïve patients with higher baseline pain, HAQ or SJC scores, seropositive patients experienced improved responses to rituximab in comparison with seronegative patients. As HAQ is driven by inflammation rather than damage in early disease, these data may suggest that, in early RA, patients with high levels of inflammation are more likely to respond to rituximab if they are seropositive. By contrast, previous studies have shown that high baseline HAQ scores predict poorer clinical responses to TNF inhibitors.8 ,18 ,19 Of note, the titre of RF or ACPA did not affect the degree of change in DAS. Some studies have suggested that RF may be a stronger predictor of rituximab responsiveness than ACPA,20 whereas others have shown the opposite.15 Our analysis found no evidence for any significant difference between RF and ACPA as indicators of improved benefit from rituximab.
The use of a fixed-effect model assumes that every study is evaluating a common effect. In this analysis, this simplistic assumption (rather than a random-effects model) was appropriate based on the limited number of studies analysed.21 ,22 In this analysis, the overall-effect model indicated generally improved benefit from rituximab, as measured by DAS28-ESR, in seropositive patients, an effect not seen in patients who received placebo treatment. Authors have speculated whether RF and/or ACPA seropositivity is predictive of treatment response to rituximab or is associated with a more generalised prognostic effect. The evidence from the overall meta-analysis model in this study suggests that a directionally opposite trend and the absence of improved benefit in seropositive patients from placebo would support a moderate predictive behaviour for rituximab response and seropositivity. However, measures of heterogeneity in this model indicated significant variation between studies. For this reason, there is a lack of evidence that the interaction of serotype with clinical outcomes from rituximab should be conceptualised as a general effect. Examining the possible causes of this heterogeneity by meta-regression yielded no further insight into patient baseline characteristics that might affect the interaction between serotype and clinical outcomes. It was hoped that further exploration of covariates, stratified by median value, would demonstrate a degree of alignment across the trials with a net reduction in the heterogeneity index. However, while baseline HAQ, pain, SJC and race were found to be significant contributors to the heterogeneity of the serotype effect among rituximab-treated patients, further analysis indicated that these effects may predominate in the MTX-naïve population. Indeed within the stratified groups of low baseline HAQ, pain or SJC, seropositive patients treated with rituximab achieved no additional clinical benefit compared with seronegative patients, the exception being in TNF-IR patients in the REFLEX study. This result was not due to a masking of therapeutic benefit in the ‘low’ biomarker groups as baseline DAS was included as a covariate in all analyses.
For other covariates that nominally might have been explored, informed consent for genetic and genomic analyses was only obtained for 40–60% of the overall trial populations. Thus insufficient numbers of patients were available to explore potential interactions in both seropositive and, in particular, seronegative patients. Given the molecular complexity, clinical heterogeneity and evolution over time of RA, it is perhaps unsurprising that simple monovariate descriptors do not robustly describe treatment response. Indeed, we and others have published data on the association between clinical response and combinations of serotype and other markers.15 ,20 ,23
A recent updated consensus statement on the use of rituximab in patients with RA reviewed the evidence regarding serological status and responsiveness to rituximab.24 Based on individual evidence from each of the rituximab randomised clinical trials included in the current meta-analysis, as well as on results from other single-centre and registry studies, it was concluded that efficacy with rituximab was evident primarily for seropositive patients and that alternative treatments might be more appropriate for seronegative patients. The results of our meta-analysis generally support the consensus statement, in particular for the licensed TNF-IR population. However, the modest effect of seropositivity in the overall population suggests that further studies are needed to determine the utility of rituximab in seronegative patients. It should also be noted that this meta-analysis used the widely accepted definition of seropositivity—that is, the presence of RF and/or ACPA autoantibodies. Recent studies indicate that other autoantibodies may be present in a significant proportion of individuals with RA and are predictive of clinical course.25 Therefore, patients currently defined as seronegative may in future be defined as seropositive based on the presence of these newly identified autoantibodies. As such, the predictive value of serological status, based on the current definition of seropositivity, may also need to be modified.
Whether the interaction of seropositivity with clinical outcome seen with rituximab is common to other biological agents is not yet clear. Published studies indicate a degree of inconsistency of the effect of seropositivity to RF or ACPA and the likelihood of response to TNF inhibitors,6 ,7 ,19 ,26,–,28 or interleukin 6 inhibition.29 ,30 Based on this study, a placebo-controlled approach, contextualising findings within treatment lines and the exploration of covariates that may modify the relationship are key requirements to adequately examine these complex interactions. Findings from such studies should improve clinical decision-making for the individualised treatment of patients based upon their serological status.
Acknowledgments
Support for third party writing assistance for this manuscript was provided by F Hoffmann-La Roche, Ltd.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding Roche Products Ltd.
-
Competing interests JDI has received consulting fees and speaker fees from Roche Products. SBC has acted as clinical investigator and/or has received consultancy fees from Amgen, Biogen-Idec, Bristol-Myers Squibb, Centocor, Flexxion Therapeutics, Genentech, Johnson & Johnson, Pfizer, Merck, Proctor & Gamble, and Roche Products. PE has provided expert advice and has acted as clinical investigator for Abbott, Bristol-Myers Squibb, Merck, Pfizer, and Roche Products. PPT has received consulting fees, speaker fees and honoraria from Genentech and Roche Products, and is an employee of, and owns stock or stock options in, GlaxoSmithKline. JW, GL, SW and SJR are employees of Roche Products. PL is an employee of Genentech and owns stock or stock options in Roche.
-
Provenance and peer review Not commissioned; externally peer reviewed.