Article Text

Abstract
Objective Undifferentiated arthritis (UA) is a diagnosis ‘per exclusionem’. Therefore this patient population may change since the development of the ACR/EULAR 2010-criteria for RA. This study evaluated characteristics and outcomes of UA in its new shape. Second, it was evaluated whether the 2010-criteria and the Leiden prediction rule were congruent in categorizing UA-patients.
Methods 2,472 early arthritis patients were studied. RA was classified according to either the 1987 or the 2010-criteria. UA was defined as not fulfilling existing classification criteria. UA-patients were compared for baseline characteristics and outcomes. In 1987-UA-patients both the 2010-criteria and the Leiden prediction rule were applied and categorization compared.
Results 2010-UA-patients (n=776) had milder baseline characteristics than 1987-UA-patients (n=1,166). During follow-up, still 24% of the 2010-UA-patients fulfilled the 1987 RA-criteria compared to 32% of the 1987-UA-patients. The 2010-UA-patients started less frequent DMARD-therapy and reached more frequent sustained DMARD-free remission. 30% of 2010-criteria-positive patients were predicted to have a low risk on RA; these patients achieved more frequent DMARD-free sustained remission than other 2010-criteria-positive patients.
Conclusion UA in the era of the 2010-criteria is less prevalent and milder at presentation and in outcome. This implies that UA-patients with unfavorable characteristics are now more often classified as RA.
Statistics from Altmetric.com
A considerable proportion of the patients presenting with synovitis of recent onset have undifferentiated arthritis. Undifferentiated arthritis is identified when none of the existing classification criteria for definitive diagnoses are fulfilled and arthritis is not septic or caused by crystals. The 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for rheumatoid arthritis (RA) were recently developed.1 Recent studies have indicated that these criteria are fulfilled earlier in the disease and more frequently than with the 1987 ACR criteria.2 3 Since undifferentiated arthritis is a disease ‘per exclusionem’, we questioned how this disease entity is characterised when applying the 2010 criteria. Therefore, the first aim of this study was to explore the characteristics and the outcome of undifferentiated arthritis in its new form.
Before the 2010 criteria were formulated, a prediction rule was developed that aimed to determine individual undifferentiated arthritis patients chances of developing RA (according to the 1987 criteria).4 Both methods are particularly applicable to patients who could not be diagnosed otherwise, thus to former undifferentiated arthritis patients. We also evaluated whether the 2010 criteria and the prediction rule were congruent in categorising early undifferentiated arthritis patients.
Patients and methods
Patients
Two thousand four hundred and seventy-two early arthritis patients, included in the Leiden Early Arthritis Clinic (EAC) between 1993 and February 2010 and who had a follow-up of at least 1 year, were studied. The EAC is a population-based prospective cohort that includes patients with confirmed arthritis and symptoms for less than 2 years.5 At baseline, patients and rheumatologists completed questionnaires, physical examinations (including 68 tender and 66 swollen joint counts) were performed, radiographs were taken, and blood was obtained for determination of the C-reactive protein level, erythrocyte sedimentation level, IgM rheumatoid factor and anticitrullinated protein antibodies. After 2 weeks, when blood and radiographic results were known, a rheumatologist diagnosed the patients as having RA, undifferentiated arthritis, or another diagnosis; this was done using the 1987 criteria for RA. This resulted in 1166 patients with undifferentiated arthritis (the so-called 1987 undifferentiated arthritis patients). We applied the 2010 criteria to the same patients and subsequently identified the so-called 2010 undifferentiated arthritis patients (n=776). Written informed consent was obtained from all participants. The study was approved by the local medical ethics committee.
Outcome
Follow-up visits were performed annually. After 1 year it was evaluated whether the 1987 criteria were fulfilled and whether disease-modifying antirheumatic drugs (DMARD) were initiated. Patients treated according to a randomised trial were not studied (n=145) for this outcome. The prescribed DMARD in RA patients differed in time; hydroxychoroquine, penicillamine, or sulfasalazine were the initial DMARD in the 1990s, and methotrexate was the initial DMARD since 1999. During a follow-up of 7 years, it was evaluated whether a patient achieved sustained remission. Sustained remission was defined as the absence of synovitis for at least 1 year after the cessation of eventual DMARD therapy.6 Furthermore, the functional ability was measured annually by the health assessment questionnaire (HAQ) score. The difference in the HAQ score over 7 years was also evaluated.
Comparison of categorisation
In order to determine whether classification according to the 2010 criteria was congruent with risk estimation by the prediction rule, both methods were applied to 1162 1987 undifferentiated arthritis patients. The congruency of classification was evaluated, as well as the disease outcome. The primary outcome here was having persistent disease (absence of sustained DMARD-free remission).
Analysis
Patient characteristics were compared using the χ2 test for nominal variables, the Student's t test for continuous variables and the Mann–Whitney U-test for non-parametric testing. Analyses of sustained DMARD-free remission were performed using univariate Cox regression analyses. The difference in HAQ score between 1987 undifferentiated arthritis patients and 2010 undifferentiated arthritis patients was compared using a multivariate normal regression analysis. As the HAQ changed over time, the interaction of the undifferentiated arthritis groups with time was entered into the model as categorical variables. p Values ≤0.05 were considered significant. Analyses were done using SPSS, version 17.0.
Results
Characteristics at presentation
Among all 2472 early arthritis patients, 772 (31.2%) patients were diagnosed other than undifferentiated arthritis or RA. Using the 1987 criteria for RA, 534 (21.6%) patients had RA and 1166 (47.2%) patients had undifferentiated arthritis. In four patients only one serological test and one acute-phase response measure was obtained and therefore they could not be classified according to the 2010 criteria.1 Subsequently, the 2010 criteria were applied to 1696 undifferentiated arthritis and RA patients. Now 920 (54.2%) patients were classified as having RA; therefore 776 (45.8%) 2010 undifferentiated arthritis patients were identified.
The baseline characteristics of the 2010 undifferentiated arthritis patients and 1987 undifferentiated arthritis patients were compared (table 1). Overall, 2010 undifferentiated arthritis patients had milder disease characteristics than the 1987 undifferentiated arthritis patients.
Patient characteristics of 1987 undifferentiated arthritis patients and 2010 undifferentiated arthritis patients, at first presentation
Outcome
After 1 year of follow-up, 23.8% of the 2010 undifferentiated arthritis patients fulfilled the 1987 criteria, compared with 32.2% of the 1987 undifferentiated arthritis patients (p=0.001). Likewise, in 32.7% of the 2010 undifferentiated arthritis patients a DMARD was initiated during the first year compared with 45.0% of the 1987 undifferentiated arthritis patients (p<0.001).
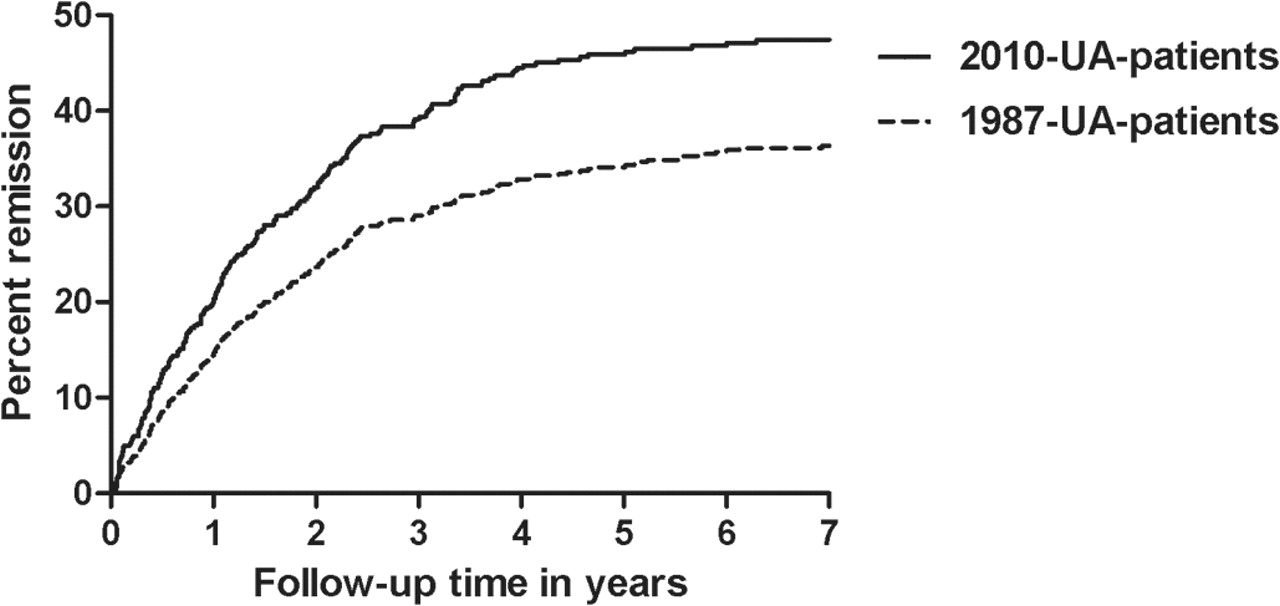
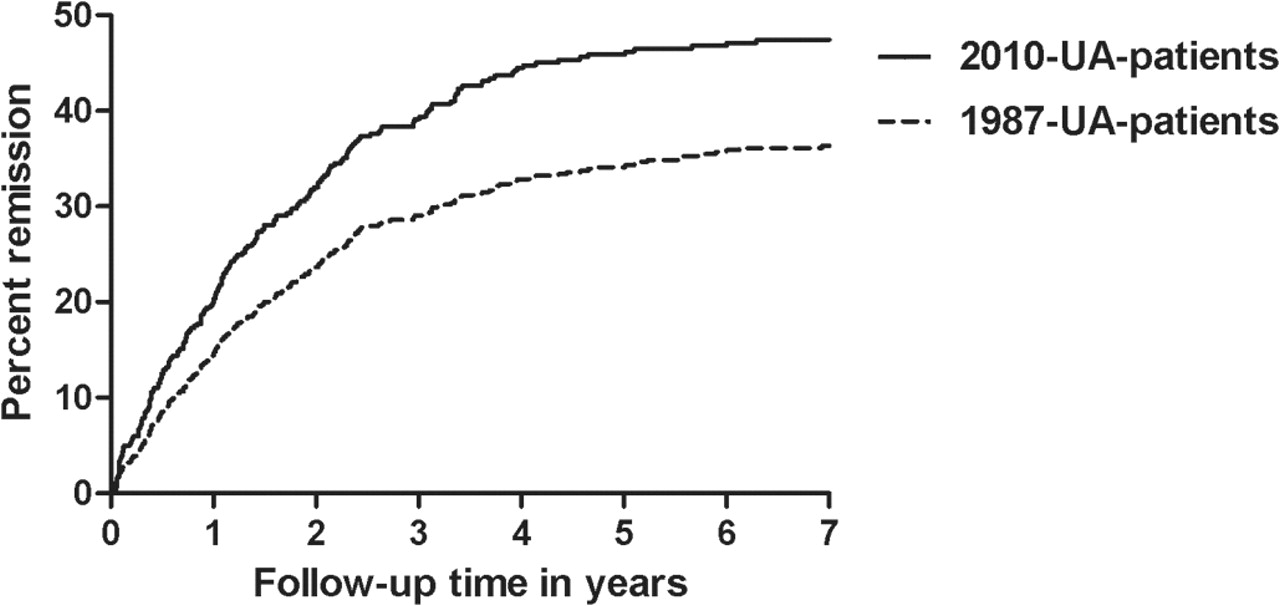
During 7 years of follow-up, the 2010 undifferentiated arthritis patients achieved sustained remission more often (45.9%) than the 1987 undifferentiated arthritis patients (34.2%) (HR 1.45, 95% CI 1.20 to 1.75; figure 1). This implies that more than half of the 2010 undifferentiated arthritis patients have persistent disease. The baseline characteristics of these patients are presented in supplementary table S1, available online only. The HAQ scores were not significantly different between the two undifferentiated arthritis groups during 7 years of follow-up (p=0.92).
{kind=link}
Kaplan–Meier curve of the percentage of patients with sustained disease-modifying antirheumatic drug-free remission in 1987 undifferentiated arthritis (UA) patients compared with 2010 undifferentiated arthritis patients.
Comparison of categorisation
All 1162 1987 undifferentiated arthritis patients were classified according to the 2010 criteria and the prediction rule (table 2). Only 0.6% of all undifferentiated arthritis patients were classified as 2010 criteria-negative but were predicted to have a high risk of RA. In contrast, 30.3% (148/489) of the 2010 criteria-positive patients were in the low risk of RA group. During follow-up 62.9% of these latter patients had persistent disease, which is a bit lower than the other 2010 criteria-positive patients (table 2).
Comparison of categorisation, according to the prediction model and the 2010 criteria, applied to 1987 undifferentiated arthritis patients and outcome of these patients over time
Discussion
This study aimed to characterise undifferentiated arthritis in its recent form, after new classification criteria for RA have been developed. It was observed that undifferentiated arthritis is still prevalent but less frequent compared with when the 1987 ACR criteria for RA are applied. In addition, we observed that both characteristics at disease presentation and the disease outcome of 2010 undifferentiated arthritis patients were milder than those of the 1987 undifferentiated arthritis patients.
With regard to the implication of the changing concept of undifferentiated arthritis, differences in disease outcome are more essential than differences at disease onset. Importantly, 2010 undifferentiated arthritis patients more often achieved sustained DMARD-free remission than 1987 undifferentiated arthritis patients. This implies that undifferentiated arthritis patients with unfavourable characteristics are now more often classified as having RA. The finding that 23.8% of the 2010 undifferentiated arthritis patients fulfilled the 1987 criteria for RA within 1 year of follow-up suggests that although the 2010 criteria classify RA earlier than the 1987 criteria,3 the 2010 criteria do not recognise approximately a quarter of the RA patients already at baseline.
We also evaluated whether the 2010 criteria and a previously derived prediction rule were congruent in categorising 1987 undifferentiated arthritis patients as having (a high probability of) RA. It was observed that the majority who did not fulfil the 2010 criteria were also in the low-risk group of the prediction rule. However, one-third of the 2010 criteria-positive patients were predicted to have a low risk of RA. During the course of the disease, these latter 2010 criteria-positive patients less frequently had persistent arthritis than the other 2010 criteria-positive patients.
Interpretation of the outcome initiation of a DMARD within the first year should be done with some caution. In the 2000s DMARD were prescribed more frequently in undifferentiated arthritis than in the 1990s. Consequently, the frequency of DMARD initiation was higher in the second compared to the first time period. Nevertheless, patients belonging to the different inclusion years were equally distributed among the categories depicted in table 2, allowing comparisons between groups. In addition, a stratified analysis in patients included before and after 2000 yielded comparable results (data not shown).
A second argument that DMARD use or fulfilling the 1987 criteria are not optimal outcome measures for the present comparison is that the first was the outcome measure used when deriving the prediction rule and the latter the outcome measure used when deriving the 2010 criteria. This might result in circle effects. Disease persistence was not used while deriving either tool, and is therefore the most neutral outcome for the purpose of this comparison. Another consideration is that 213 of the presently studied patients were also used in the data-driven phase of the derivation of the 2010 criteria and 570 of the 1166 undifferentiated arthritis patients were used for the derivation of the prediction rule.
Evaluation of congruency of both methods is formally not correct, as the 2010 criteria were meant for classification and the prediction rule was derived to estimate individual patients' probability of fulfilling the 1987 criteria at an early stage. On the other hand, the 2010 criteria will most likely also be used for individual patients in the clinic. Although a comparison of the disease outcomes of the concordantly and discordantly classified patients should be considered reluctantly, an evaluation as to whether both the classification criteria and the prediction rule identify patients with RA early is clinically relevant.
In conclusion, the present data revealed that undifferentiated arthritis when applying the 2010 criteria is less prevalent and milder at presentation and in outcome. In addition, it was observed that 24% of 2010 criteria-negative patients fulfilled the 1987 criteria within 1 year. This implies that although undifferentiated arthritis patients with unfavourable characteristics are now more often classified as having RA, careful clinical observation of 2010 undifferentiated arthritis patients is indicated.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Funding The work of AK is supported by a grant from the Dutch Arthritis Foundation. The work of AHMvdHvM is supported by a grant from the Dutch organisation of Health Research and Development. The research has been funded by the European Community Seventh Framework Program FP7 Health-F2-2008–223404 (Masterswitch) and by a core grant from the Dutch Arthritis Foundation.
Competing interests None.
Patient consent Obtained.
Ethics approval The study was approved by the local medical ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.