Article Text

Abstract
Objectives To examine how rituximab may result in the inhibition of joint destruction in rheumatoid arthritis (RA) patients.
Methods Twenty-eight patients with active RA were treated with rituximab. Radiographs of hands and feet before and 1 year after therapy were assessed using the Sharp–van der Heijde score (SHS). Expression of bone destruction markers was evaluated by immunohistochemistry and immunofluorescence of synovial biopsies obtained before and 16 weeks after the initiation of treatment. Serum levels of osteoprotegerin, receptor activator of nuclear factor κB ligand (RANKL), osteocalcin and cross-linked N-telopeptides of type I collagen (NTx) were measured by ELISA before and 16 weeks post-treatment.
Results After 1 year, the mean (SD) change in total SHS was 1.4 (10.0). Sixteen weeks after treatment there was a decrease of 99% in receptor activator of nuclear factor κB-positive osteoclast precursors (p=0.02) and a decrease of 37% (p=0.016) in RANKL expression in the synovium and a trend towards reduced synovial osteoprotegerin expression (25%, p=0.07). In serum, both osteoprotegerin (20%, p=0.001) and RANKL (40%, p<0.0001) levels were significantly reduced 16 weeks after treatment, but the osteoprotegerin/RANKL ratio increased (157%, p=0.006). A trend was found towards an increase of osteocalcin levels (p=0.053), while NTx concentrations did not change.
Conclusions Rituximab treatment is associated with a decrease in synovial osteoclast precursors and RANKL expression and an increase in the osteoprotegerin/RANKL ratio in serum. These observations may partly explain the protective effect of rituximab on the progression of joint destruction in RA.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterised by inflammation of the synovial tissue and destruction of the underlying cartilage and bone, both resulting in functional impairment. The goal of antirheumatic treatment is not only to attenuate the clinical symptoms of joint inflammation, but also to inhibit the progression of joint destruction.1
The presence of rheumatoid factors and/or anticitrullinated protein antibodies, produced by B lineage cells, is a predictor of radiological damage.2,–,5 Rituximab, an anti-CD20-directed B-cell depletive therapy, is an effective treatment for RA patients, especially for those positive for rheumatoid factor and/or anticitrullinated protein antibodies.6,–,10 Importantly, rituximab treatment also reduces the progression of joint destruction in RA patients, even in the absence of a clear-cut clinical response.11 12 Taken together, these data suggest an association between B cells and the development of joint destruction.
Insight into the interplay between immune cells and cells involved in bone remodelling in RA is evolving. In chronic arthritis, resorption of mineralised cartilage and subchondral bone is mediated by osteoclasts, which are present in inflamed synovial tissue of RA patients at the area of bone erosions.13 Arthritis can be induced in mice lacking osteoclasts, but these mice do not develop bone erosions,14 15 illustrating the critical role of osteoclasts in arthritic bone loss. Receptor activator of nuclear factor κB (RANK), a member of the tumour necrosis factor (TNF) receptor family, and its ligand (RANKL) are important stimulators of osteoclast differentiation and activation, and inhibitors of osteoclast apoptosis. The RANK–RANKL interaction is inhibited by osteoprotegerin, a naturally occurring, soluble decoy receptor for RANKL.16
Proinflammatory cytokines important in RA pathogenesis, such as TNFα, interleukin (IL) 1β and IL-6, not only stimulate the production of both RANKL and osteoprotegerin, but also act directly on osteoclasts and their precursors.17 Furthermore, matrix metalloproteinases, expressed by fibroblast-like synoviocytes (FLS), macrophages, neutrophils and chondrocytes, play a key role in the degradation of unmineralised cartilage and their production is also augmented by these cytokines.18
The cellular and molecular mechanisms involved in the effect of rituximab on joint erosions are as yet unknown. Exploration of the ongoing processes in serum and synovium, the target tissue of RA, before and after B-cell depletion, could teach us more about the cross-talk between the immune system and the cells involved in bone resorption in RA. Therefore, we examined the effects of B-cell depletion on the RANK/RANKL/osteoprotegerin system.
Patients and methods
Patients
Twenty-eight RA patients were included from an open-label study on the synovial tissue response to rituximab treatment that was previously reported.19 All patients were diagnosed according to the 1987 American College of Rheumatology classification criteria for RA20 and had active disease despite methotrexate treatment. Active RA was defined as having four of more tender joints and four of more swollen joints of 28 joints assessed, and at least one of the following: erythrocyte sedimentation rate of 28 mm/h or greater, serum C-reactive protein levels of 15 mg/l or greater or morning stiffness for 45 min or longer. The study was performed according to the Declaration of Helsinki and approved by the Medical Ethics Committee of the Academic Medical Center/University of Amsterdam; all patients gave written informed consent.
Study design
All patients were treated with two intravenous infusions of 1000 mg rituximab (days 1 and 15), as previously described.19 Premedication with methylprednisolone was omitted to study the specific effect of rituximab. The disease activity score in 28 joints was measured before and every month after treatment. Serum and synovial tissue were obtained before (ie, baseline) and 16 weeks after the initiation of treatment.
Serum ELISA
Serum levels of osteoprotegerin were measured before and 16 weeks after treatment as part of a multiplex ELISA, as previously described.21 Serum levels of total soluble RANKL (sRANKL; Immundiagnostik, Bensheim, Germany), osteocalcin (Immunodiagnostic Systems, Liege, Belgium) and cross-linked N-telopeptides of type I collagen (NTx) (Osteomark; Inverness Medical, Princeton, New Jersey, USA) were measured by ELISA before and after the initiation of treatment.
Synovial biopsy, immunohistochemical analysis and quantification of stained tissue sections
At baseline and week 16, serial synovial biopsies were collected by needle arthroscopy of the same actively inflamed joint, as previously described.22 Frozen sections (5 μm) were stained with the following mouse monoclonal antibodies: anti-osteoprotegerin (clone 98A1071; Imgenex, San Diego, California, USA), anti-RANK (clone 80707; R&D Systems, Minneapolis, Minnesota, USA) to detect osteoclast precursors and anti-tartrate-resistant acid phosphatise-1 (TRAcP-1; clone ZY-9C5; Invitrogen, Breda, The Netherlands) to detect mature osteoclasts. The staining of TRAcP-1 was performed using a three-step immunoperoxidase method, as previously described.23 For the staining of RANK, osteoprotegerin and all other cellular markers, bound antibody was detected with a polymer-horseradish peroxidase anti-mouse antibody (Envision+ System; Dako, Glostrup, Denmark) and aminoethylcarbazole (AEC; Dako) was used as dye. For the TRAcP staining, sections from an osteoblastoma containing numerous mature osteoclasts (obtained from the pathology department of the Academic Medical Center) were used as a positive control. As a negative control, irrelevant/isotype-matched immunoglobulins were applied to the sections instead of the primary antibody or the primary antibody was omitted.
The expression of synovial markers was quantified using digital image analysis, as previously described.24 The expression level of RANK-positive cells was presented as cell counts/mm2; osteoprotegerin was presented as integrated optical density/mm2, an arbitrary unit representing the intensity of staining per mm2.25
Immunofluorescence to detect RANKL in synovial tissue
Rabbit-anti-human RANKL (AbCam, Cambridge, UK) was developed with donkey anti-rabbit rhodamine (Jackson ImmunoResearch, Suffolk, United Kingdom). Sections were first adsorbed with phosphate-buffered saline supplemented with 2% bovine serum albumin for 10 min. Primary and secondary antibodies diluted in phosphate-buffered saline supplemented with 2% bovine serum albumin were incubated at room temperature in the dark for 1 h or 30 min, respectively. Sections were immersed in Hoechst 33258 (Sigma, Gillingham, United kingdom) at 20 µg/ml for 2 min for nuclear counterstaining, then mounted and kept in the dark at −20°C. A Zeiss LSM 780 Zen confocal microscope was used to visualise staining and Zeiss LSM image examiner software was used for pixel quantification. The expression level of RANKL was presented as pixels/μm2.
Radiographic assessments
Radiographs of hands and feet were obtained at baseline and at different time points after the initiation of rituximab treatment. The same observer, who was blinded to radiograph sequence, evaluated paired radiographs using the Sharp–van der Heijde scoring method (SHS), which consists of the joint space narrowing score and erosion score (range 0–448).26 Using an assumption of linear progression, the change in SHS after 1 year was calculated.
Statistical analysis
Continuous data were described as mean and SD, if normally distributed, and as median and range, if not normally distributed. Correlations were calculated using Spearman's ρ. The Wilcoxon signed-rank test for paired data was used to analyse the change after treatment of the different parameters analysed in synovial tissue and serum. All statistical analyses were performed with SPSS 17.0 software. A p value of 0.05 or less was considered statistically significant.
Results
Clinical characteristics
The demographic and clinical features of the cohort are shown in table 1. Of note, this population had a long disease duration and had failed previous treatment with several disease-modifying antirheumatic drugs and biological agents. Sixteen weeks post-treatment there was a mean (SD) decrease in the disease activity score of 1.6 (1.1), and two patients (7%) had a good response, 18 (64%) a moderate response and eight (29%) no response according to the European League Against Rheumatism (EULAR) response criteria.27
Baseline characteristics of patients
Radiographic outcomes
First, we analysed the progression in joint destruction after 1 year. From 25 of the 28 patients paired radiographs of hands and feet were available from before and after rituximab treatment. The median (range) of the total SHS score was 36 (0–247) at baseline and 39 (0–246) 1 year post-rituximab. After 1 year, the mean (SD) change in total SHS was 1.4 (10.0), change in the joint space narrowing score was 0.6 (5.0) and change in the erosion score was 0.8 (5.0) (figure 1A). Of the 25 patients analysed, seven patients (28%) showed progression of joint destruction of more than one point in the total SHS and only four patients (16%) increased more than three points in 1 year (figure 1B). The three patients without any erosion at baseline stayed non-erosive after 1 year. Of note, these data are comparable with the mean changes in radiological scores that were seen in a large clinical trial evaluating the effect of rituximab in RA patients with a disease duration of more than 10 years.11 Although in that clinical trial a different scoring system for erosive destruction was used (total Genant-modified Sharp score), it supports the notion that our cohort is representative.
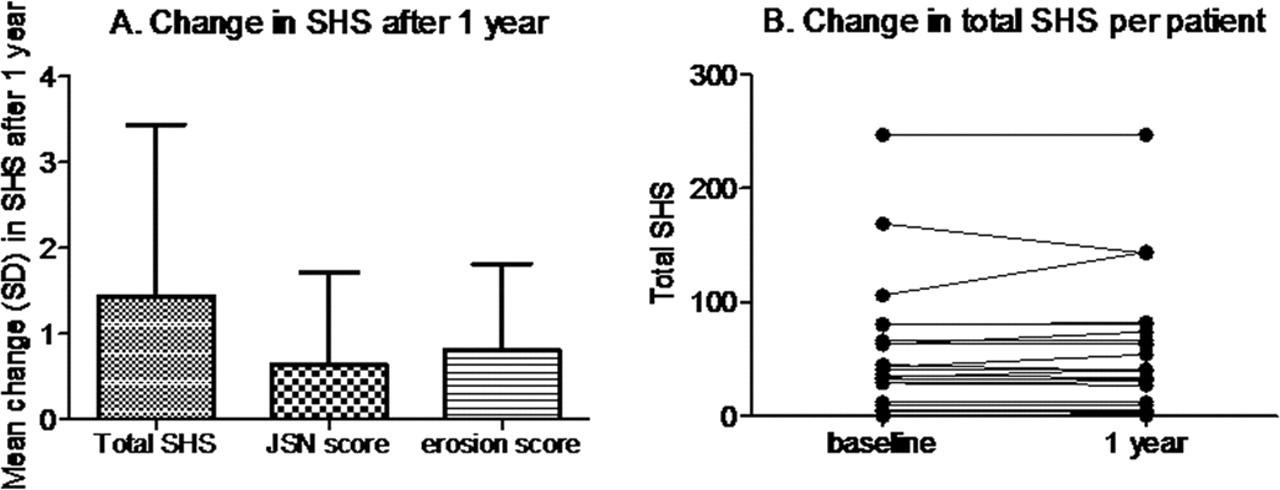
Radiographic outcomes 1 year after treatment with rituximab. Mean (SD) changes after 1 year of the total Sharp–van der Heijde score (SHS), joint space narrowing (JSN) score and erosion score of 25 rheumatoid arthritis patients (A). Individual changes of the total SHS after 1 year (B).
Effect of rituximab on synovial osteoclast precursors, osteoprotegerin, RANKL expression and osteoclasts
For the synovial tissue analysis of RANK and osteoprotegerin expression, we included paired biopsies of 20 patients, based on availability and the fulfilment of quality control criteria. Consistent with previous observations from our group,28 only seven patients (35%) showed RANK expression and nine patients (45%) showed osteoprotegerin expression at baseline. There was no correlation between the baseline expression of RANK or osteoprotegerin on the one hand, and total SHS on the other (r=−0.22, p=0.39 and r=−0.18, p=0.49, respectively). After treatment with rituximab, there was a significant reduction of 99% in RANK-positive osteoclast precursors at week 16 (p=0.02), whereas osteoprotegerin expression showed a non-significant decrease (25%, p=0.07; figure 2). To detect the expression of RANKL, we used immunofluorescence and included paired biopsy samples of 11 patients, for whom sufficient material was present to perform this analysis. All patients expressed RANKL at baseline and the expression tended to correlate with the total SHS score (r=0.60, p=0.05) at baseline. After treatment with rituximab, we observed a significant decrease of 37% of RANKL expression (p=0.016; figure 2). No TRAcP-positive mature osteoclasts could be detected in any of the synovial tissue samples (data not shown). Separate analyses showed that changes in synovial bone and cartilage destruction markers were not related to changes in SHS or disease activity (data not shown).

Expression of receptor activator of nuclear factor κB (RANK), osteoprotegerin (OPG) and receptor activator of nuclear factor κB ligand (RANKL) in synovium before and 16 weeks after treatment with rituximab. Individual changes in synovial osteoprotegerin (A), RANK (B) expression and RANKL (C) of 20 (A and B) or 11 (C) rheumatoid arthritis patients. The treatment effect was compared using a Wilcoxon signed-rank test; *p<0.05. Representative examples of immunohistochemical and immunofluorescence staining of the synovium for osteoprotegerin before (A1) and after (A2) treatment, for RANK before (B1) and after (B2) treatment and for RANKL before (C1) and after (C2) treatment with rituximab. Magnification 20× (A and B) and 10× (C).
Changes in serum levels of osteoprotegerin, sRANKL and the osteoprotegerin/sRANKL ratio after rituximab treatment
As we saw a strong effect of rituximab on the RANK/RANKL/osteoprotegerin system in the synovial tissue, we also analysed osteoprotegerin and sRANKL levels in the serum of 28 patients. Sixteen weeks after the initiation of rituximab treatment, we found a statistically significant decrease in serum levels of both osteoprotegerin and sRANKL (from 3253 (median) to 2796 pg/ml, 20%, p=0.001, and from 30.2 to 16.5 ng/ml, 40%, p<0.0001, respectively). Of importance, the osteoprotegerin/sRANKL ratio increased (from 0.06 (median) to 0.09, 157%, p=0.006; figure 3). Separate analyses showed that changes in serum bone and cartilage destruction markers were not related to changes in the SHS or disease activity (data not shown).

Serum levels of soluble receptor activator of nuclear factor κB ligand (sRANKL) and osteoprotegerin (OPG), and the osteoprotegerin/sRANKL ratio before and 16 weeks after treatment with rituximab. Individual changes in soluble receptor activator of nuclear factor-κB ligand (sRANKL; A) and serum osteoprotegerin (B) expression, and the osteoprotegerin/sRANKL ratio (C) of 28 rheumatoid arthritis patients. The treatment effect was compared using a Wilcoxon signed-rank test; **p<0.01.
Change in soluble markers of bone turnover
Finally, we studied the effect of rituximab on systemic biomarkers of bone turnover. We measured serum osteocalcin levels as a marker of bone formation and levels of NTx as a biomarker of bone resorption before and 16 weeks after the initiation of rituximab treatment. We found a strong trend towards an increase of osteocalcin levels (from (median) 12 to 12.5, p=0.053), while NTx concentrations did not change (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serum levels of osteocalcin and cross-linked N-telopeptides of type I collagen (NTx) before and 16 weeks after the initiation of treatment with rituximab. Individual changes in osteocalcin (A) and NTx (B) of 28 rheumatoid arthritis patients. The treatment effect was compared using a Wilcoxon signed-rank test. nM BCE, nmol bone collagen equivalents per litre.
Discussion
These results show that rituximab treatment strongly affects the RANK/RANKL/osteoprotegerin system in the synovium and peripheral blood of patients with active RA. The number of RANK-positive osteoclast precursors in synovial tissue was decreased by 99% and RANKL expression was decreased by 37%, whereas synovial osteoprotegerin showed a non-significant reduction. In serum, however, both sRANKL and osteoprotegerin decreased, whereas the osteoprotegerin/sRANKL ratio was elevated. These alterations in the RANK/RANKL/osteoprotegerin system were not related to radiological progression, as assessed by the SHS. However, joint destruction was stabilised in a large majority of patients, indicating that rituximab's interference with the mediators of osteoclastogenesis resulted in the inhibition of further bone loss. This is in line with a large, randomised clinical trial in which rituximab inhibited the progression of joint destruction in the majority of patients with RA, including those who did not experience an American College of Rheumatology response.11 Taken together, these data at least partly provide an explanation for the effective inhibition of joint destruction observed in clinical trials after B-cell depletive therapy.
What could be the exact role of B cells in rheumatic joint destruction? It is generally known that RANKL is produced by FLS29 and T cells30 in a membranous or soluble (sRANKL) form after stimulation by IL-1, TNFα and IL-17, a product of T-helper 17 cells.31 32 However, B cells are also able to secrete RANKL.33 34 Of importance, a recent study using cytokine messenger RNA profiling identified B cells as major producers of RANKL in the synovial fluid of RA patients.35 Proinflammatory cytokines also stimulate the secretion of osteoprotegerin by FLS and dendritic cells in synovium, as well as CD40L on T cells. T-cell activation is an important function of B cells in the synovium of RA patients.36 Therefore, B cells may also upregulate both RANKL and osteoprotegerin production by stimulating T cells. We have previously shown in the same cohort that rituximab induces a significant albeit variable decrease in synovial B cells and an indirect decrease in T cells, plasma cells, macrophages and lymphoid neogenesis 16 weeks after the initiation of rituximab treatment.19 The observed changes in the RANK/RANKL/osteoprotegerin system may thus be explained at least partly by decreased cell infiltration.
RANK is primarily expressed on mononuclear macrophage-lineage cells, including preosteoclastic cells, dendritic cells, fibroblasts and B and T cells,37 which are abundantly present in inflamed synovial tissue. RANKL interacts with RANK by direct cell–cell contact and thereby promotes the differentiation of osteoclast precursors into mature osteoclasts.31 RANK-positive osteoclast precursors were seen in 35% of our patients, but TracP-positive mature osteoclasts could not be detected in the synovium. This is in contrast with several other studies, which showed osteoclasts to be present at the interface of inflamed synovial tissue and the periosteal surface.38 These differences might be explained by the use of synovial tissue obtained during joint replacement surgery in these previous investigations versus arthroscopy-guided synovial biopsies in the present study. Direct physical contact with the skeletal matrix is required for the differentiation into mature osteoclasts,39 but arthroscopic synovial biopsies do not include the junction between this periosteal surface and the synovium. Nevertheless, we were able to analyse changes in the interaction between immune cells and bone resorptive precursor cells at the site of inflammation, as described above.
A recently published, small study investigated whether rituximab treatment had a systemic effect on bone remodelling in 13 active RA patients resistant to TNFα antagonist therapy; synovial tissue was not assessed. There was a trend towards reduced sRANKL levels in the serum, which did not reach statistical significance, perhaps due to the small number of patients. Of interest, levels of the bone resorption marker, desoxypyridinoline, were significantly reduced after rituximab treatment.40
Other antirheumatic therapies have been reported to have various effects on the RANK/RANKL/osteoprotegerin system in the synovium.41,–,43 Treatment with TNFα antagonists, which has a clear inhibitory effect on the progression of joint destruction even in the absence of a clinical response,44 for 12 weeks induced an increase in synovial osteoprotegerin expression without affecting RANKL, resulting in an increased osteoprotegerin/RANKL ratio.41 Similarly, successful treatment with different disease-modifying antirheumatic drugs other than TNFα inhibitors led to increased osteoprotegerin and decreased RANKL expression and an increased osteoprotegerin/RANKL ratio.42 In contrast, clinical responders to anakinra (IL-1 receptor antagonist), administered as monotherapy or in combination with pegsunercept (PEGylated soluble TNF receptor type I, an TNFα antagonist), showed a reduction in osteoprotegerin expression after 1 year, but RANKL and the osteoprotegerin/RANKL ratio remained unchanged.43 The decreased expression of systemic, but not synovial, osteoprotegerin that we observed after B-cell depletion may be related to effects on a variety of cells. This soluble receptor is produced for instance by bone marrow stromal cells, dendritic cells, endothelial cells, fibroblasts, monocytes, B cells and T cells under the influence of proinflammatory cytokines.37 The reduction of sRANKL in our patients led to an elevated osteoprotegerin/sRANKL ratio, as seen in several of the aforementioned clinical studies. The relative expression levels of osteoprotegerin and RANKL are critical for the regulation of osteoclastic activity and bone resorption, and this ratio seems to be the most important predictor of later joint destruction in chronic, destructive arthritis.45
We found markedly increased osteocalcin levels 16 weeks after treatment at a borderline level of statistical significance, suggesting an increase in bone formation activity. Consistent with our results, previous studies have shown that serum levels of osteocalcin are negatively correlated with disease activity in RA patients.46 47 Of note, one other study in 46 RA patients did not demonstrate a change in osteocalcin 6 months after rituximab treatment;48 the reason for this discrepancy is at present unclear. The fact that serum NTx did not change can perhaps be explained by the long disease duration of our cohort, as previous studies have shown that carboxy terminal telopeptide (a comparable bone resorption marker) levels are decreased in RA patients with a disease duration of more than 10 years. When baseline levels are already low, it is more difficult to demonstrate a decrease.49 In addition, we cannot exclude the possibility that changes in NTx levels might have been detectable if this biomarker had been tested in urine, but urine samples were unfortunately not available in our study.
In conclusion, the results presented here support a link between B cells and the RANK/RANKL/osteoprotegerin system at the site of inflammation and destruction. Depletion of B cells may ultimately interfere with this mechanism, protecting the joints against progressive destruction.
Acknowledgments
The authors would like to thank Alian Bakker for support with the immunohistochemical stainings, Dr BM Lodde for editorial assistance and Professor DMFM van der Heijde for providing the SHS scores.
References
Footnotes
-
Funding This research was funded by the Dutch Arthritis Association.
-
Competing interests PPT has served as a consultant to Genentech and Roche.
-
Patient consent Obtained.
-
Ethics approval The study was performed according to the Declaration of Helsinki and approved by the Medical Ethics Committee of the Academic Medical Center/University of Amsterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.