Article Text

Abstract
Background Anti-tumour necrosis factor (TNF) therapy may be associated with opportunistic infections (OIs).
Objective To describe the spectrum of non-tuberculosis OIs associated with anti-TNF therapy and identify their risk factors.
Methods A 3-year national French registry (RATIO) collected all cases of OI in patients receiving anti-TNF treatment for any indication in France. A case–control study was performed with three controls treated with anti-TNF agents per case, matched for gender and underlying inflammatory disease.
Results 45 cases were collected of non-TB OIs in 43 patients receiving infliximab (n=29), adalimumab (n=10) or etanercept (n=4) for rheumatoid arthritis (n=26), spondyloarthritides (n=3), inflammatory colitis (n=8), psoriasis (n=1) or other conditions (n=5). One-third (33%) of OIs were bacterial (4 listeriosis, 4 nocardiosis, 4 atypical mycobacteriosis, 3 non-typhoid salmonellosis), 40% were viral (8 severe herpes zoster, 3 varicella, 3 extensive herpes simplex, 4 disseminated cytomegalovirus infections), 22% were fungal (5 pneumocystosis, 3 invasive aspergillosis, 2 cryptococcosis) and 4% were parasitic (2 leishmaniasis). Ten patients (23%) required admission to the intensive care unit, and four patients (9%) died. Risk factors for OIs were treatment with infliximab (OR=17.6 (95% CI 4.3 - 72.9); p<0.0001)or adalimumab (OR=10.0 (2.3 to 44.4); p=0.002) versus etanercept, and oral steroid use >10 mg/day or intravenous boluses during the previous year (OR=6.3 (2.0 to 20.0); p=0.002).
Conclusion Various and severe OIs, especially those with intracellular micro-organisms, may develop in patients receiving anti-TNF treatment. Monoclonal anti-TNF antibody rather than soluble TNF receptor therapy and steroid use >10 mg/day are independently associated with OI.
Statistics from Altmetric.com
Introduction
Treatment with tumour necrosis factor (TNF) antagonists has represented a major breakthrough in the treatment of several inflammatory diseases, such as rheumatoid arthritis (RA), ankylosing spondylitis, Crohn's disease, psoriatic arthritis and psoriasis, with anti-TNFα inhibitors playing a major role.1
Because TNF plays a major role in defence against infection and in the formation and maintenance of granulomas, TNF antagonists are recognised as a risk factor for reactivation of latent tuberculosis (TB).2,–,4 Other opportunistic infections (OIs) such as listeriosis, non-typhoid salmonellosis, histoplasmosis, pneumocystosis and other fungal or viral infections have been described in patients receiving these agents.5,–,13
We created in 2004 a national registry in France, named RATIO (Research Axed on Tolerance of bIOtherapies), to collect all cases of OI occurring during 3 years in French patients receiving anti-TNF treatment for any indication. Occurrence of an OI is a severe life-threatening adverse event and it is essential to know whether anti-TNF might increase this risk. However, the incidence of OIs is rare and the incidence of these events is not easily determined from classic registries where the patient enters when anti-TNF therapy has already been started. The large power of the RATIO registry, which includes more than 50 000 patient-years, and in which the patient enters when an OI has occurred, is therefore ideal to provide us with information on these very rare adverse events, which are difficult to obtain from other registries.
This original strategy allowed us to determine that the risk of Legionella pneumophila pneumonia was increased in patients receiving anti-TNF treatment and that TB remained the most common OI occurring in such patients despite recommendations for screening and treatment of latent TB.4 ,14 We reported that this risk of TB was higher with treatment with monoclonal anti-TNF antibody than with the TNF soluble receptor analogue.4 The aim of this large study was to describe cases of other OIs associated with anti-TNF therapy and their outcome and to identify risk factors for their occurrence, particularly the potential influence of each of the three anti-TNF drugs licensed in France during the time of the study. Moreover, the follow-up of each case from the date of the diagnosis of the disease to 3 years' follow-up allowed us to obtain information on the rate of cure and the risk of relapse.
Patients and methods
The French RATIO registry was designed by a multidisciplinary expert group to prospectively collect all cases of OI occurring from 1 February 2004 to 1 February 2007, in patients who were receiving or had received anti-TNF treatment before the occurrence of the OI. This registry involved cases from clinicians of all concerned medical specialties and the French drug agency (Agence Française de Sécurité Sanitaire des Produits de Santé (AFSSAPS)) and its network of 31 regional pharmacovigilance centres. The methodology of RATIO has been described in detail elsewhere.4
We conducted an incidence study and performed a case–control analysis to investigate the risk factors for newly diagnosed non-TB OIs in patients receiving anti-TNF agents.
Identification and validation of OI cases
To enhance the exhaustiveness of the collection of cases, different sources were used. All cases reported to the 31 French pharmacovigilance regional centres were collected (reporting of severe drug-related adverse events for clinicians is mandatory in France), as were cases reported directly to the pharmaceutical companies producing anti-TNF drugs. In addition, doctors from all French hospital centres involved in the prescription of TNF antagonists (ie, from rheumatology, internal medicine, gastroenterology and dermatology departments) and/or in the management of OI (ie, from infectious diseases centres, intensive care units, chest medicine units) were required to report each newly diagnosed case. A direct mail reminder was sent four times a year, and several communications at congresses or in local specialised media encouraged the reporting of cases.
A detailed standardised case report form was completed for each reported case of OI whatever the source of notification, and additional documents were collected (hospitalisation summary, histological and microbiological results, and other data if necessary) for the validation process.
Validation of cases
All cases (from all sources) were included in the RATIO registry, with a validated OI diagnosis. OI definition was based on the list of OIs used to identify C and B stages of HIV infection.15 We adapted the definition used for HIV infection, and added to the list other severe infections usually considered as opportunistic in immunosuppressed patients (online supplementary table 1). We excluded TB because it represented most of the collected cases of OI, as well as legionellosis, which were the subject of specific analyses.4 ,14 An expert committee consisting of three infectious disease specialists (DSC, OL, SB) carried out a consensus-based validation process for all OI cases. Cases for which diagnosis was uncertain or possible (as opposed to definite) were excluded. An OI was considered cured when all signs of infection had disappeared (general signs, like fever, and organ-specific signs). Relapse was validated by the expert committee with the same criteria used as for the initial infection.
Assessment of exposure to anti-TNF therapy
The three anti-TNF agents were available for use for the duration of this 3-year study. Infliximab has been available since 1999, etanercept since 2002 and adalimumab since 2004. For these anti-TNF agents, French regulations require the first prescription to be obtained from hospital doctors. For patients who had received more than one anti-TNF agent, we considered three ways of examining the exposure: first anti-TNF agent, last anti-TNF agent, and any use of the anti-TNF agent.
Incidence study
Incidence rate of OIs
We estimated the annual incidence rate of OIs in patients receiving anti-TNF treatment, adjusted for age and sex, with the French population used as reference (direct standardisation).
The numerator consisted of the validated cases of OI from the RATIO registry.
For the denominator, as described elsewhere,4 we estimated the number of patient-years of receipt of anti-TNF agents in France during the 3-year period of the study (2004, 2005 and 2006) from different sources: the national French agency of drugs (AFSSAPS), the three pharmaceutical firms (Abbott, Schering-Plough and Wyeth) and the Régime Social des Indépendants (RSI) (the French health insurance fund for self-employed workers). Each group provided their estimation of the number of patient-years for the three anti-TNF agents. We used the mean of these different estimates (which were consistent) to derive an estimation of the number of patients receiving each anti-TNF agent, which we used in the main analysis.
Risk of OI in patients receiving anti-TNF treatment
A case–control study was performed with cases from the RATIO registry.
Cases
Cases were all validated cases of OI in the registry with a labelling indication for use of anti-TNF treatment: RA, spondyloarthritis (ankylosing spondylitis or psoriatic arthritis), ulcerative colitis or Crohn's disease, or psoriasis. For patients with two OIs, only the first was included in the case–control analysis. Patients were included in the case–control analysis if they were being treated with an anti-TNF agent at the time of first symptoms of OI or if the anti-TNF treatment had been stopped <24 months before the first symptoms.
Controls
Controls were patients treated with anti-TNF agents (current treatment or stopped for <24 months), for a labelled indication, in whom no OI had ever developed. These controls were included from centres involved in the RATIO registry, during the same inclusion period as the cases, and gathered into a global pool of controls. From that pool, we randomly selected patients for a database of controls reflecting the proportion of patients receiving each of the three anti-TNF drugs available in France during the study period. Three controls for each case were randomly selected from that database, matched to cases by sex and underlying inflammatory disease.
Statistical analysis
Annual incidence of OI
The age- and sex-adjusted incidence rates of OI were calculated for anti-TNF agent use as a whole (all anti-TNF) and for each agent individually, with the French population as a reference. For that determination, age and sex distribution of the treated patients were issued from the pool of controls, reflecting the proportion of patients receiving each of the three anti-TNF drugs available in France during the study period. Crude incidence rates were also calculated for each of the principal micro-organisms involved to enable comparison with data from the general population.
Case–control study
We identified the risk factors of OI by both univariate and multivariate analysis (conditional logistic regression model). The predefined factors potentially predictive of the occurrence of an OI considered were age, lymphopenia, neutropenia, diabetes, haemopathy, duration of the underlying inflammatory disease, first and last anti-TNF agent received, time from onset of anti-TNF treatment and from onset of last anti-TNF treatment, use of a potentially immunosuppressive disease-modifying antirheumatic drug during the previous year, use of steroids during the previous year and oral steroid therapy >10 mg/day or intravenous bolus during the previous year.
Factors included in the stepwise multivariate model were those associated with the status (case or control) on univariate analysis with a significance level of p<0.20. We used the bootstrap method to examine the stability of our final model (1000 replicated bootstrap samples to find candidate variables that were retained; the final model included variables retained in more than 20% of the multivariate models). A p<0.05 was considered statistically significant.
Sensitivity analyses
To better assess the drug-specific risk, we performed sensitivity analyses of the incidence of OI and the ORs for the risk with adalimumab or infliximab versus etanercept therapy, varying the definition of exposure (all anti-TNF agents, by anti-TNF agent, receiving only one anti-TNF agent, receiving anti-TNF therapy for at least 6 weeks, and currently receiving anti-TNF therapy) and denominator estimates (from each of the three pharmaceutical firms and the RSI).
Statistical analysis was carried out using SAS release 9.1 (SAS Inst, Cary, North Carolina, USA).
Compliance with research ethics standards
This study was authorised by the ethics committee of AP-HP, GHU Nord (Institutional Review Board of Paris North Hospitals, Paris 7 University, AP-HP; authorisation number 162-08). The registry was reported at clinicaltrials.gov (identifier: NCT00224562).
Results
Description of the OI cases
We collected data on 67 cases of OI, and 45 cases in 43 patients were validated by the validation committee. The other 22 cases were excluded because of lack of microbiological/histological confirmation (n=17) or because they were not considered to be an OI (n=5). The diagnosis of the 45 infections was as follows: 15 bacterial infections (four listeriosis, four nocardiosis, four atypical mycobacteriosis, three non-typhoid bacteraemic salmonellosis), 18 severe viral infections (eight severe herpes zoster, three varicella with visceral involvement, three extensive herpes simplex infection, four disseminated cytomegalovirus (CMV) infection), 10 fungal infections (five pneumocystosis, three invasive aspergillosis, two cryptococcosis), and two parasitic infections (two leishmaniasis). Characteristics of the patients are shown in table 1. OI occurrence by anti TNF agent is reported in supplementary table 2.
Characteristics of 43 patients with OI (for patients with two OIs, characteristics at the first OI are presented)
For the 34 patients who had received only one anti-TNF agent, 25 had received infliximab, seven adalimumab and two etanercept. For the two patients with two OIs, one received infliximab for RA and presented aspergillosis, then infliximab was resumed and the patient secondarily developed listeriosis. The second received infliximab for inflammatory colitis and presented concomitantly a disseminated CMV infection and a pneumocystosis (HIV-positive patient). Six patients had another cause of immunosupression than anti-TNF (one diabetes mellitus, one history of cancer, one AIDS, three chronic obstructive pulmonary disease).
Clinical features of OI and outcome
Among the 43 patients, eleven patients (25.6%) required hospitalisation in an intensive care unit and four patients died after a median 1.2 (IQR=0.8–14.2) months after OI diagnosis (table 2). After a median follow-up of 32.8 (24.3–36.0) months, 33 were considered cured and three had at least one relapse. The outcome was missing for three cases.
Clinical presentation of cases of OI that occurred between February 2004 and January 2007 in patients receiving, or who had received, treatment with anti-TNF agents in France
At OI diagnosis, anti-TNF therapy was stopped in all patients except for one with pneumocystosis receiving infliximab, who recovered. Moreover, anti-TNF therapy was resumed in 17 patients (40%) after a median OI treatment duration of 1.7 (IQR=1.3–5.0) months (treatment with the same anti-TNF agent was resumed in all patients except three (one patient switched from infliximab to adalimumab, two patients switched from infliximab to etanercept). Two relapses occurred in these 17 patients (one with aspergillosis and one herpes zoster despite prophylaxis). In the 26 patients who did not resume anti-TNF therapy, one relapse occurred (one with nocardiosis).
Time occurrence of OI with anti-TNF therapy
The median time to occurrence of an OI from the start of anti-TNF therapy was 16.2 (6.0–26.0) months. The median time from the start of the last anti-TNF treatment was 8.7 (3.1–20.4) months. Only three had stopped anti-TNF for more than 4 months before occurrence of an OI (6.5 and 11 months for two cases of pneumocystosis, and 4.3 months for a CMV infection)
Incidence of OI for patients receiving anti-TNF therapy
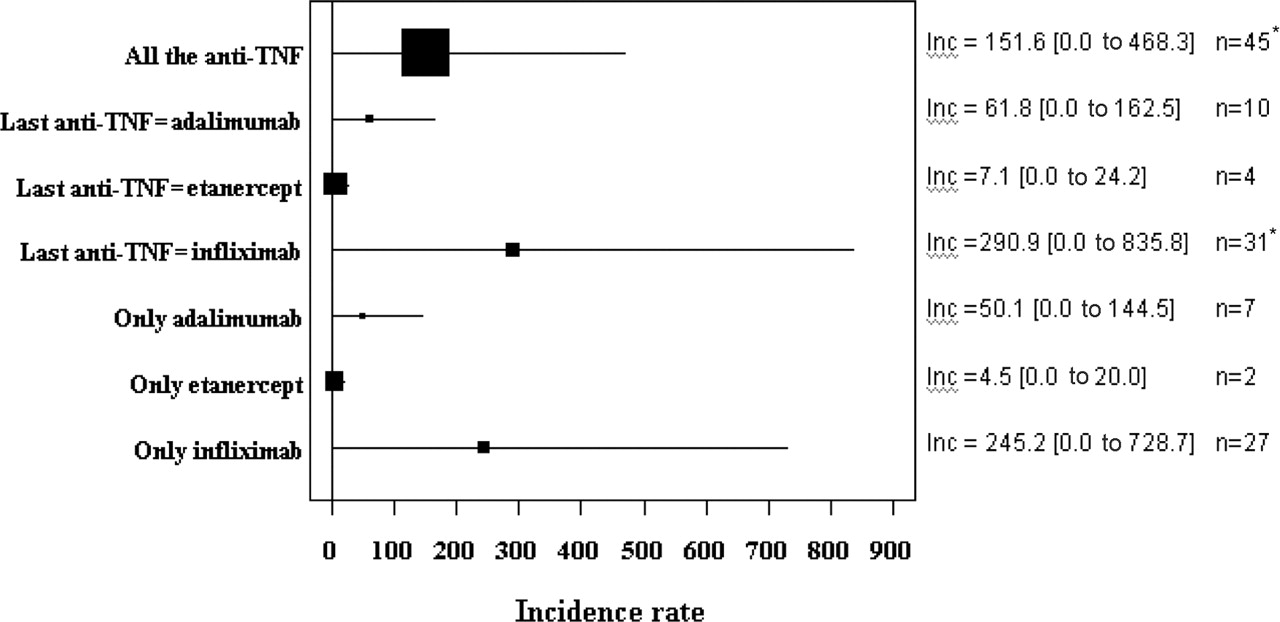
The main analysis relied on a total number of 57 711 patient-years of use of anti-TNF therapy in France during the 2004–6 study period, with 18% receiving adalimumab, 51% etanercept and 31% infliximab as the denominator of the incidence rate. The annual incidence rate of OI adjusted for age and sex for patients receiving anti-TNF treatment, with the French population as a reference, was 151.6 (95% CI 0.0 to 468.3) per 100 000 patient-years. Crude incidence rates for each of the principal micro-organisms involved in RATIO and in the French general population are given in supplementary table 3.
The incidence of OI for patients receiving anti-TNF treatment differed depending on the agent used without reaching statistical significance. The annual adjusted incidence rate of OI was 7.1 (0.0 to 24.2) per 100 000 patient-years with etanercept, 290.9 (0.0 to 835.8) with infliximab and 61.8 (0.0 to 162.5) with adalimumab.
We observed the same pattern in the main analysis and in the different sensitivity analyses (figure 1), even with separate analyses using different estimates of the denominator of the incidence rate from independent sources, which gave consistent adjusted incidence rates (supplementary figure 1).

Age and sex adjusted incidence rate of opportunistic infections (OIs; per 100 000 patient-years) with 95% confidence interval, for all the anti-tumour necrosis factor (anti-TNF) agents, according to the last anti-TNF agent received and according to each drug in patients having received only one anti-TNF. Inc, incidence rate; n, number of cases of OI seen in each category. The plot size relates to the number of patients treated included in the calculation (denominator of the incidence rate) *Two patients treated with infliximab are counted twice since they presented with two successive OIs.
Risk factors of OI for patients receiving anti-TNF therapy
The case–control study involved 38 cases (only cases treated for approved indication) and 114 controls. Among them, only two had stopped anti-TNF for more than 4 months (4.33 and 11 months). The results of the univariate case–control analysis are shown in table 3. In the final model of the multivariate analysis (table 4), the following factors were predictive of OI: treatment with infliximab versus etanercept (OR=17.6 (95% CI 4.3 to 72.9); p<0.0001); treatment with adalimumab versus etanercept (OR=10.28 (95% CI 2.35 to 44.94); p=0.002), and treatment with steroids >10 mg/day or intravenous boluses during the previous year (OR=10.0 (95% CI 2.3 to 44.4); p=0.002). Description of the bootstrap process to assess the stability of the model is described in supplementary figure 2.
Risk factors of OI for patients receiving anti-TNF therapy (univariate analysis)
Risk factors of OI for patients receiving anti-TNF therapy (multivariate analysis, final model)
Sensitivity analysis (figure 2) including the analysis performed in patients with current anti-TNF treatment, gave similar results. Another sensitivity analysis including in addition to the 38 validated OI cases the 17 others excluded because of lack of microbiological/histological confirmation gave similar results (data not shown).

{kind=link}
{kind=link}
Sensitivity analysis of the results of the case–control analysis: odds ratios (ORs) from multivariate analysis for the risk of opportunistic infection (OI) with adalimumab (in black) or infliximab (in grey) treatment rather than etanercept treatment. n, number of cases included in the case–control model (three controls for each case are included in the model). The plot size relates to the number of cases included in the case–control analysis (n).
Discussion
Common bacterial infections such as pulmonary and soft-tissue infections are the most common severe infections occurring in patients receiving anti-TNF drugs (4–6/100 patient-years in patients with long-term RA), but OIs are also a concern.5,–,7 ,16 ,17
From the RATIO registry, we previously reported 69 cases of TB, which were the most common OIs occurring in patients receiving anti-TNF drugs in France during the same period (2004–6).4 In this paper, we focused on non-TB OIs because we wanted to exclude the weight of TB, which represented more than half of the observed OIs. We observed a diverse spectrum of non-TB OIs, although each occurred far less frequently than TB. Crude incidences for the main micro-organisms involved were around ten times higher than those of the general population in France or in developed countries as shown for listeriosis (6.9 (0.00 to 18.70) vs 0.5/100 000), as well as for nocardiosis (6.9 (0.00 to18.70) vs 0.87/100 000) (see supplementary table 3). However, taking into account the rarity of the events, the CIs of the incidences were very large. The spectrum of those infections differs somewhat from that seen in AIDS, although several infections are seen in both situations. For example, we did not observe any OIs occurring at a late stage of immunodeficiency in AIDS, such as progressive multifocal leucoencephalopathy, or parasitic digestive infections, such as cryptosporidiosis and microsporidiosis. Conversely, we observed in almost all cases, infections due to intracellular multiplying micro-organisms, with a severe course: 26% of our patients required hospitalisation in an intensive care unit and 9% died from the OI.
This study demonstrated a higher risk of OI for patients receiving monoclonal antibody treatment (infliximab or adalimumab) than for those receiving soluble TNF receptor treatment (etanercept), with a 10- to 17-fold difference in risk in the case–control analysis, a fact we also recently highlighted for TB.4 This difference in risk did not reach statistical significance in the incidence study. A difference between infliximab and etanercept in risk of OI was previously suggested in the literature. Wallis and Ehlers reported on the spontaneous declaration of granulomatous infections to the US Food and Drug Administration (FDA) for patients treated with anti-TNF agents in the United States up to 2002.18 As in our study, TB was the most common OI. Among non-TB OIs, the risk was suggested to be higher with infliximab than etanercept.18 In 2003, 15 cases of Listeria infection were reported by the Adverse Event Reporting System of the FDA, 14 with infliximab use and one with etanercept.12 The Spanish BIODASER registry reported six cases of Listeria infection, five with infliximab use and one with adalimumab.11 Twenty-two cases of histoplasmosis were described from endemic areas, 19 with infliximab use and three with etanercept.19 Likewise, 13 cases of coccidioidomycosis were described within endemic areas, 12 with infliximab use and one with etanercept.20 In a review of published cases of fungal infections,13 of 281 cases, 226 (80%) were associated with use of infliximab, 44 (16%) with etanercept and 11 (4%) with adalimumab. Histoplasmosis (n=84), candidiasis (n=64) and aspergillosis (n=64) were the most common fungal infections.13 Pneumocystis jiroveci infection was reported in 21 Japanese patients receiving infliximab.9 Finally, a difference between treatment with monoclonal anti-TNF and the soluble receptor analogue in risk of severe herpes zoster infection was recently described.21 The possible mechanisms underlying this differential risk of OI, probably the same as those explaining the differential risk of TB, have been reviewed elsewhere22 ,23 and are based on differences of affinity or avidity for binding TNF on the cell membrane, thus resulting in differences in reverse signalling.
In our study, we confirmed the association of other classic risk factors of OI (ie, lymphopenia, diabetes, treatment with immunosuppressive disease-modifying antirheumatic drugs during the previous year and steroid therapy > 10 mg/day or in intravenous boluses during the previous year), with only high-dose steroids remaining associated with OI on multivariate analysis. This finding agrees with results of analysis of risk factors of severe infections in patients with RA or with systemic lupus erythematosus24 ,25 and strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents.
This study has some limitations First, the denominator of the incidence rate and the repartition between the three anti-TNF agents used for the choice of the controls were estimated only. However, each pharmaceutical company providing TNF blockers evaluated the number of patient-years during the same period for each anti-TNF agent thus, the difference in risk between agents we observed cannot be explained by different methodologies used for the different agents. Furthermore, in the sensitivity analyses, the estimates from independent sources gave consistent adjusted incidence rates.
Second, despite the different strategies used to identify all cases in the whole country of France, we cannot exclude the possibility that we missed some cases and that our incidence rate might be underestimated, although participation in this survey was encouraged by the French agency of drugs (AFSSAPS) and the French scientific societies of rheumatology, gastroenterology, dermatology and infectious diseases. Moreover, some infections, considered only possible owing to the absence of definite microbiological criteria, could not be retained in the final multivariate analysis. However, a sensitivity analysis including possible cases, confirmed the higher risk of OI with monoclonal antibody as compared with soluble receptor. In addition, the rate of potentially missing cases is unlikely to differ by anti-TNF agent used because these infections are severe and require hospitalisation, and are thus unlikely to be underdiagnosed in patients receiving subcutaneous anti-TNF agents as compared with an intravenous agent and thus with an inhospital follow-up. Moreover, there is no reason to expect a potential difference of reporting between the two subcutaneous anti-TNF agents.
Third, as OIs are rare, this study suffers from a lack of power, resulting in a wide range of 95% CIs of the OR and incidence rates (preventing statistical significance of the incidence rates being reached). Additionally, the small number of events also precludes the possibility of making adjustments for more confounders in the multivariate analysis. To deal with this limitation, we used the bootstrap method to examine the stability of our final model and reinforce the robustness of the results. The final model included variables retained in more than 20% of the multivariate models.
Although this national survey design has some limitations, even limitations of power, this design is probably the most powerful way of investigating differences in risk with the use of anti-TNF agents for rare, severe adverse events such as OIs. Cases were included in our registry when the adverse event occurred, not when the treatment began. Thus, the population on which we focused was the whole French population, which allowed us to collect in 3 years many more cases of OI than those collected by all other registries.
Contrary to the standard pharmacovigilance notifications, all files of OI patients included in the RATIO registry were reviewed and validated by an expert committee using strict definition criteria, which is a main quality issue, especially for the diagnosis of OI, which may be difficult.
In conclusion, non-TB OIs are diverse, mainly because of a wide range of intracellular pathogens. Although less common than TB, they are severe, with a 9% mortality. Our study provides clear evidence of the high risk of occurrence of non-TB OIs with monoclonal anti-TNF antibody rather than soluble TNF receptor therapy.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
Marc Lemann is deceased and this paper is dedicated to him.
DSC, FT, PR and XM contributed equally to the work.
-
Funding RATIO was supported by a research grant from INSERM (Réseau de recherche clinique 2003 and 2006) and by an unrestricted grant from Abbott, Schering Plough and Wyeth. The pharmaceutical companies Abbott, Schering Plough and Wyeth had no role in the study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all the data and had final responsibility for the decision to submit for publication.
-
Competing interests ML received consulting and/or talk honoraria from Abbott, Schering Plough and UCB (<US$10 000each), XM received consulting and/or talk honoraria from UCB and Wyeth (<US$10 000 each).
-
Ethics approval This study was conducted with the approval of the ethics committee of AP-HP, GHU Nord (Institutional Review Board of Paris North Hospitals, Paris 7 University, AP-HP); authorization number 162-08.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
The RATIO GROUP includes Bagheri Haleh; Blandin Bernadette; Breban Maxime; Bretagne Stéphane; Castot Anne; Chichmanian Rose-Marie; Chosidow Olivier; Dautzenberg Bertrand, Dellamonica Pierre; Dufeu-Demazes Nadine; Emilie Dominique; Gillet Claudine; Hugot Jean Pierre; Kreft-Jais Carmen; Lemann Marc; Leport Catherine; Lortholary Olivier; Mariette Xavier; Michelet Christian; Montastruc Jean Louis; Nicolas Nathalie; Prieur Anne Marie; Ravaud Philippe; Roux Christian; Salmon Dominique; Tubach Florence; Vittecoq Daniel.The validation-cases expert committee comprised three infectious disease specialists: Salmon Ceron Dominique, Lortholary Olivier, Bretagne Stéphane.