Article Text

Abstract
Purpose To evaluate the potential of etanercept versus sulfasalazine to reduce active inflammatory lesions on whole-body MRI in active axial spondyloarthritis with a symptom duration of less than 5 years.
Methods Patients were randomly assigned to etanercept (n=40) or sulfasalazine (n=36) treatment over 48 weeks. All patients showed active inflammatory lesions (bone marrow oedema) on MRI in either the sacroiliac joints or the spine. MRI was performed at weeks 0, 24 and 48 and was scored for active inflammatory lesions in sacroiliac joints and the spine including posterior segments and peripheral enthesitis by two radiologists, blinded for treatment arm and MRI time point.
Results In the etanercept group, the reduction of the sacroiliac joint score from 7.7 at baseline to 2.0 at week 48 was significantly (p=0.02) larger compared with the sulfasalazine group from 5.4 at baseline to 3.5 at week 48. A similar difference in the reduction of inflammation was found in the spine from 2.2 to 1.0 in the etanercept group versus from 1.4 to 1.3 in the sulfasalazine group between baseline and week 48, respectively (p=0.01). The number of enthesitic sites also improved significantly from 26 to 11 in the etanercept group versus 24 to 26 in the sulfasalazine group (p=0.04 for difference). 50% of patients reached clinical remission in the etanercept group versus 19% in the sulfasalazine group at week 48.
Conclusion In patients with early axial spondyloarthritis active inflammatory lesions detected by whole-body MRI improved significantly more in etanercept versus sulfasalazine-treated patients. This effect correlated with a good clinical response in the etanercept group.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
The treatment of ankylosing spondylitis (AS) with tumour necrosis factor (TNF) alpha blocking agents has been shown to be highly effective.1,–,4 Shorter disease duration, together with young age, were among the best predictors for a major treatment response in several analyses.5,–,7 The new Assessment of SpondyloArthritis International Society (ASAS) criteria for axial spondyloarthritis were published recently covering both patients with and without radiographic sacroiliitis.8 Active inflammation of the sacroiliac joints as shown by MRI is an important part of these new criteria.9
Until now two clinical studies with TNF blockers have been performed in patients with non-radiographic axial spondyloarthritis showing a very good response in a high percentage of patients with a disease duration of less than 3 years.7 ,10
MRI is currently the best imaging method for the detection of active inflammation in the sacroiliac joints and the spine and an impressive reduction of such active inflammation could be demonstrated in the past in several trials treating AS patients with TNF blockers,10 ,11 but the treatment effect on other parts of the skeleton were not investigated by MRI.
Whole-body MRI may be an ideal tool to study not only the spine and sacroiliac joints but also the enthesial areas.12,–,14 Two previous studies demonstrated that whole-body MRI and conventional MRI showed a high correlation of active inflammation both in the investigation of the sacroiliac joints15 and spine.16
In the current prospective randomised trial we investigated the effect of treatment with the TNF blocker etanercept in comparison with treatment with sulfasalazine on active bony inflammation in the whole skeleton by whole-body MRI as the primary outcome parameter over 12 months in patients with early axial spondyloarthritis with a symptom duration of less than 5 years.
Patients and methods
Study design
In this 48-week, randomised multicentre open-label trial (ClinicalTrials.gov identifier NCT00844142), 76 patients with non-steroidal anti-inflammatory drug (NSAID)-refractory axial spondyloarthritis were prospectively randomly assigned17 to etanercept 25 mg given twice weekly subcutaneously (n=40) or sulfasalazine 2–3 g per day given orally according to the local rheumatologist's decision (n=36) for treatment over 48 weeks. In the case of intolerance to sulfasalazine patients could be switched to methotrexate (15–20 mg weekly by mouth). The study was approved by an independent ethics committee.
Inclusion and exclusion criteria
Patients had to be 18–50 years of age and had to have a diagnosis of axial spondyloarthritis with a symptom duration of less than 5 years. The diagnosis was made based on the presence of chronic low back pain with a duration of at least 3 months and onset at less than 45 years of age. All patients had to have active inflammatory lesions (osteitis/bone marrow oedema) on whole-body MRI in either the sacroiliac joints or the spine plus three out of the following criteria: (1) inflammatory back pain;18 (2) good or very good response to NSAID; (3) one or more of the extraspinal manifestations such as uveitis, peripheral arthritis, enthesitis; (4) HLA-B27 positivity; (5) a positive family history for spondyloarthritis.8 ,9 ,19 ,20 Retrospectively, all patients fulfilled the recently published ASAS classification criteria for axial spondyloarthritis.8 All patients had to have a Bath ankylosing spondylitis disease activity index (BASDAI) of 4 or greater21 and a back pain score (BASDAI question 2) of 4 or greater, despite treatment with NSAID and had undergone investigation with the same whole-body MRI at weeks 0, 24 and 48. Treatment with disease-modifying antirheumatic drugs or 7.5 mg/day or more of prednisone (or equivalent) had to be discontinued at least 4 weeks before initiation of the study.
Outcome assessments
The primary endpoint of this study was the change of active inflammatory lesions in the sacroiliac joints and spine as detected by MRI at 48 weeks. Secondary endpoints were the reduction of active inflammatory lesions on the posterior elements of the spine and a reduction of peripheral enthesitis on MRI, and the following clinical endpoints: BASDAI50, ASAS20 and 40 and ASAS partial remission.22 ,23
Other clinical and laboratory outcome assessments24 included BASDAI, Bath ankylosing spondylitis functional index (BASFI),25 Bath ankylosing spondylitis metrology index (BASMI) on an 11-point answer scale,26 a modified enthesitis Maastricht ankylosing spondylitis enthesitis score27 with an additional two sites at each knee (17 sites), a swollen joints count with 64 joints,28 patient's and physician's global assessments of disease activity and C-reactive protein (CRP).24 ,29,–,31
Whole-body MRI
Whole-body MRI was performed on a 1.5 T scanner (Avanto TIM, Siemens, Germany) according to a previously described protocol.12 ,14 Due to the configuration of the coils, elbow, wrist, finger and toe joints could not be depicted.
Scoring of whole-body MRI
MRI were scored for active inflammatory lesions by two radiologists, blinded for treatment arm and MRI time point.
Active inflammatory lesions of the sacroiliac joints were scored according to a slightly modified previously described scoring method,32 with each sacroiliac joint divided into four quadrants. Each quadrant was scored for osteitis/bone marrow oedema as follows: 0, absent (no osteitis); 1, less than 33% of quadrant area; 2, 33% or more to less than 66% of quadrant area; 3, 66% or more of quadrant area with a maximum score of 24. For the entire spine with 23 vertebral units, a recently described33,–,35 scoring system was used to score active inflammation, resulting in a score between 0 and 69, grade 0–3 per vertebral unit. The sacroiliac joint and the spine MRI scores were calculated by using the mean values of both scorers. Scoring of the posterior elements included assessment for active inflammatory lesions of the facet joints, the costovertebral joints and the spinous processes in each vertebral unit. Posterior segments and peripheral enthesitis (active osteitis) were scored in consensus between both scorers with a ‘yes’ or ‘no’ answer for altogether 27 enthesitic sites of the non-axial skeleton (for further details see Althoff et al, manuscript in preparation).
The intraclass correlation coefficient (ICC) at baseline was 0.93 for assessing active inflammatory lesions of the spine and 0.96 for the sacroiliac joints. The ICC for change scores were 0.86 (spine) and 0.94 (sacroiliac joints), respectively.
Statistical analysis
Statistical analysis was performed as an intention-to-treat, last observation carried forward analysis. The non-parametric Mann–Whitney test was used to compare treatment groups at baseline. To compare changes in the sacroiliac joint and spine MRI scores between the treatment groups by taking the baseline status into account a non-parametric analysis of covariance (non-parametric ANCOVA) was used.36 In a sensitivity analysis the possible influence of the diagnosis at baseline (non-radiographic axial spondyloarthritis vs AS), HLA-B27 positivity, elevated CRP, clinical arthritis status on the primary outcome was examined by including those parameters as co-variables into the non-parametric ANCOVA model. One sulfasalazine patient with missing MRI data was excluded from the primary analysis. In 10 other patients (etanercept five, sulfasalazine five) with missing MRI data at week 48 the last observation carried forward method was applied to complete the data for the primary analysis. The non-parametric ANCOVA or, if appropriate, the usual parametric ANCOVA with the baseline value as a co-variable was applied to analyse secondary outcomes.
Furthermore, the parametric ANCOVA was used to investigate the correlation between changes in clinical parameters (BASDAI, BASFI, CRP, enthesitis count at week 48) and changes in MRI score (spine, sacroiliac joints, enthesitis) after adjustment for treatment and the baseline status in the corresponding clinical and MRI parameter. p Values less than 0.05 were considered statistically significant. The Holm procedure was applied to adjust for repeated significance testing of the primary outcome.37
Results
Baseline characteristics
Of the 76 patients fulfilling the inclusion criteria, 40 were randomly assigned to receive etanercept and 36 sulfasalazine. The mean dose of sulfasalazine was 1688 mg (n=32) at week 24 and 1650 mg (n=30) at week 48; four patients were switched to methotrexate (15.0 mg weekly for each patient) because of intolerance to sulfasalazine. Patients' characteristics were similar, with no statistical difference between the etanercept and the sulfasalazine group (table 1–3).
Baseline characteristics of study patients by treatment group
MRI scores of sacroiliac joints, spine, enthesitis and posterior segments of the spine at baseline, week 24 and at week 48 in the etanercept versus sulfasalazine treatment group
Efficacy data at baseline, week 24 and at week 48 in the etanercept versus sulfasalazine treatment group
All patients were active as shown by clinical parameters and positive MRI (table 2). At baseline, 94.6% of the patients showed active inflammatory lesions in the sacroiliac joints, 47.3% in the spine, but only 5.4% in the spine but not in the sacroiliac joints.
Primary and secondary MRI outcome parameters
In the etanercept group, there was a clear reduction of the mean sacroiliac joint score from 7.8 at baseline to 2.4 at week 48 (table 2). After adjusting for the non-significantly different baseline MRI score, this reduction remained significantly (p=0.02) larger compared with the sulfasalazine group: 5.4 and 3.5, respectively (table 2). Inflammation was thus reduced after 1 year of treatment by 69.2% in the etanercept group in comparison to 35.2% in the sulfasalazine group. The same was true when the reduction of inflammation in the spine was compared between the two groups (p=0.01) (table 2). The results of the primary outcome remained significant after taking the presence of two co-primary endpoints (MRI sacroiliac joint and spine scores) into account. In the sensitivity analysis similar significant results were found for the primary endpoints. Figure 1 shows MRI examples for the reduction of active inflammatory lesions in the sacroiliac joints, the spine and enthesitis. The improvement on the patient level is shown in the probability plots in figure 2.

Examples for MRI before and after 48 weeks of treatment with etanercept: (a) sacroiliac joints: baseline MRI, sacroiliac joint score 15.5 (A), week 48 MRI, sacroiliac joint score 0 (B); (b) spine, baseline MRI spine score 11.5 (C), week 48 MRI spine score 1 (D); (c) enthesitis of lateral condyle of femur of right knee (dorsal view), MRI baseline with enthesitis (E), week 48 without enthesitis (F).

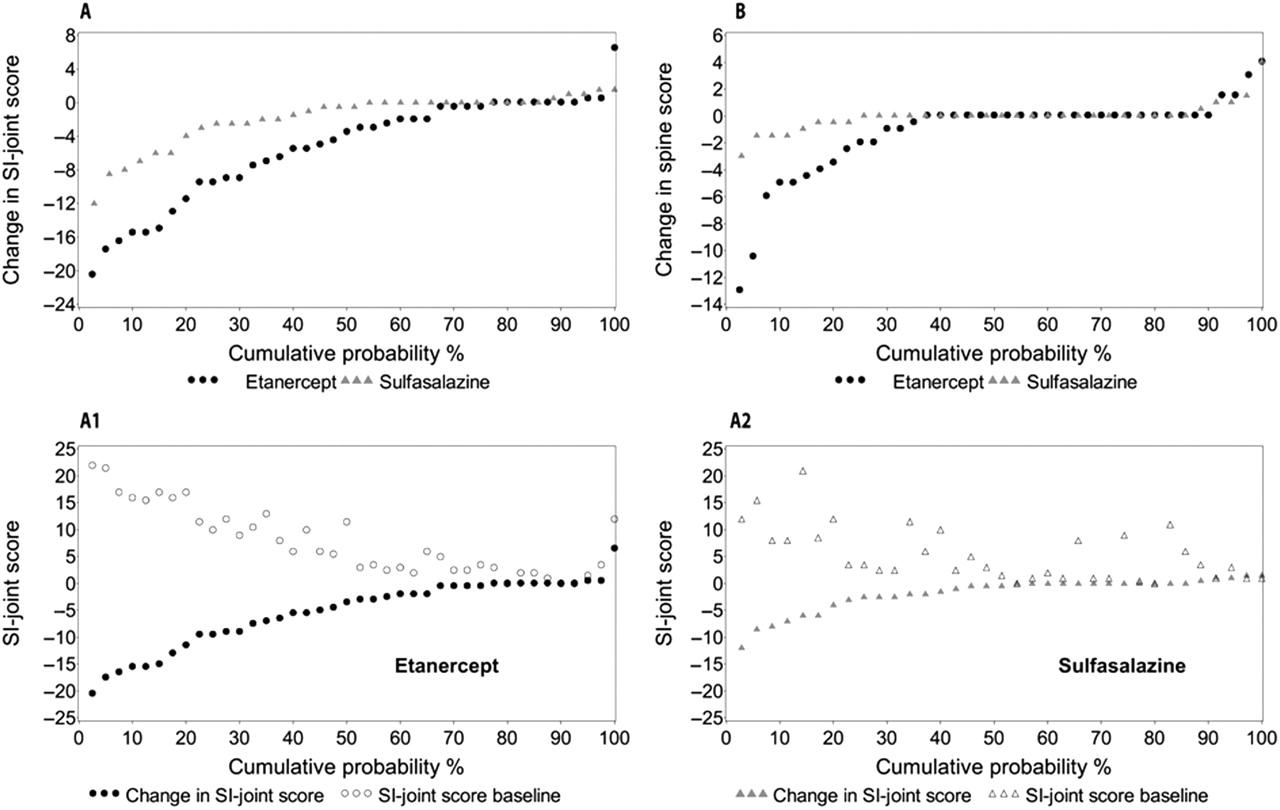
Cumulative probability of changes in MRI activity scores of the sacroiliac (SI) joints (A) and the spine (B) from baseline to week 48 in the etanercept and sulfasalazine treatment groups. Each data point in A and B represents an individual patient. For sacroiliac joint scores, double probability plots for the etanercept group (A1) and the sulfasalazine group (A2) are shown, with the baseline MRI activity score for each patient plotted above the corresponding change scores from baseline to week 48.
When analysing only patients with at least one active spinal lesion (n=35), the difference in the improvement of the MRI spine score was even more remarkable (etanercept baseline 4.2, week 48 1.9; sulfasalazine baseline 3.7, week 48 3.2), resulting in a reduction of 55% in the etanercept group versus 14% in the sulfasalazine group (p=0.03).
At week 48 six patients from the etanercept compared with two patients from the sulfasalazine treatment group became free of any active inflammatory lesions on MRI at any site in the skeleton including the spine, sacroiliac joints, entheses and posterior elements.
As shown in table 2, active inflammation in the posterior segments of the spine was present in 13 patients (17.1%). There was a reduction from 37 to 26 sites in the etanercept group between baseline and week 48 versus from 18 to 13 sites in the sulfasalazine group; however, this difference was not significant (table 2). Enthesitis was present in 31 patients (40.8%) at baseline. The number of enthesitic sites was reduced significantly by 58% at week 48 in the etanercept group, whereas there was no reduction in the sulfasalazine group (p=0.04 for the difference between the two groups; table 2).
Secondary clinical outcome parameters
The analysis of the clinical efficacy data showed a statistically significant reduction of all analysed variables in the etanercept in comparison with the sulfasalazine treatment group, except for the BASMI, swollen joints, clinical enthesitis and CRP (table 3 and figure 3).

{kind=link}
{kind=link}
{kind=link}
Response of the Assessment of SpondyloArthritis International Society (ASAS) criteria for 20% improvement in disease activity (ASAS20), the ASAS40, the ASAS criteria for partial remission (Pr), and the Bath ankylosing spondylitis disease activity index criteria for 50% improvement (BASDAI50) in week 48 after treatment with etanercept (n=40) or sulfasalazine (n=36) in patients with active axial spondyloarthritis. Significantly more patients from the etanercept group compared with the sulfasalazine group reached ASAS20 (85%, 95% CI 70.7% to 93.3% vs 42%, 95% CI 25.5% to 59.2%; p=0.001), ASAS 40 (70%, 95% CI 54.2% to 83.4% vs 31%, 95% CI 17.7% to 46.6%; p=0.001), ASAS partial remission (50%, 95% CI 34.4% to 65.6% vs 19%, 95% CI 8.5% to 35.5%; p=0.006) and BASDAI50 (65%, 95% CI 48.3% to 78.8% vs 28%, 95% CI 14.2% to 43.6%; p=0.001).
There was a significant correlation between changes in BASDAI and BASFI and changes in the MRI sacroiliac joint scores (p values were 0.04 and 0.0069, respectively), but not for CRP. However, there was no significant correlation between MRI enthesitis and MRI spine scores and clinical parameters.
Of the six patients who became completely free of inflammation both in the sacroiliac joints and spine in the etanercept group, all patients were also in clinical remission according to the ASAS criteria (15.4% of the whole etanercept-group). In contrast, none of the two patients reaching remission in the sulfasalazine group (0%) was free of inflammation as shown by whole-body MRI, a significant difference between the groups (p=0.03).
When the whole group was separated into patients with AS and patients with non-radiographic axial spondyloarthritis there were no clear differences for the reduction in MRI scores and clinical parameters (data not shown).
Dropouts
Seven dropouts were noted before week 24, another three before week 48, among them five each in the etanercept group (two wishes for pregnancy, three lost to follow-up), and the sulfasalazine group (two lost to follow-up, one discontinuation because of side-effects and lack of efficacy and one patient because of new lymphoma).
Safety
Three hundred and twenty-one adverse events (AE) occurring in 71 patients were reported (167 AE in 39 etanercept patients and 154 AE in 32 sulfasalazine patients). Infections of the respiratory tract were the most frequently reported AE. In total, there were three serious AE in the etanercept group and seven in the sulfasalazine group. Among the serious AE only three were regarded as potentially treatment related (one etanercept and two sulfasalazine patients).
Discussion
In the present study we performed the most comprehensive analysis so far of the response of active inflammation, as shown by MRI, to treatment with a TNF blocker in comparison with sulfasalazine treatment over 1 year in patients with axial spondyloarthritis. In these patients with a symptom duration of less than 5 years most inflammation was found in the sacroiliac joints in comparison with the spine or other extraspinal sites. Accordingly, a larger improvement in sacroiliac joint inflammation was observed compared with spinal inflammation when patients were treated with etanercept (table 2), but the differences compared with the sulfasalazine group were clearly significant both for the sacroiliac joint and spine at week 24 and at week 48.
The current study can best be compared with an infliximab trial in axial spondyloarthritis patients with a symptom duration of less than 3 years, which also showed a good reduction of active inflammation on MRI.10
In the study mentioned above,10 an improvement in the spinal inflammation was also reported, but only the presence or absence of inflammation per spinal area was scored without further quantification and without differentiation of inflammation found in the vertebral body and the posterior segment.
There was no clear difference between the two treatment groups in the reduction of inflammation present in the posterior segments of the spine (table 2) in the present study, which may be due to the small percentage of patients in whom the posterior segment was involved. The 17% positive patients at baseline in our study are different from previous reports, which found inflammation at this site in a higher percentage of patients.38 ,39
So far only one whole-body MRI study has tried to score inflammatory sites other than spine and sacroiliac joints in patients with axial spondyloarthritis.40 In that study only the shoulder and pelvic girdles and the anterior chest wall were included, whereas the lower extremities were left out, although they are frequently affected in spondyloarthritis. Therefore, again the current study is the first one to include these sites and, even more importantly, to investigate inflammation in a blinded controlled fashion over 1 year of treatment with etanercept compared with sulfasalazine.
Enthesitis by MRI was found in 40.8% of patients, a frequency lower than clinically evident enthesitis (table 1). Most interestingly, the number of enthesitic sites was reduced by nearly 58% (table 2) at week 48 in the etanercept group, a percentage similar to the reduction in inflammation observed in the sacroiliac joints and spine. On the other hand, there was no reduction in the sulfasalazine group, supporting the view that inflammation in sacroiliac joints, spine and enthesitic sites has a very similar immunopathology and response to treatment.41 ,42 Until now only one other controlled study showed a favourable effect of a TNF blocker, in this case also etanercept, on enthesitis as shown by MRI.43
Because only the reading of the MRI and not treatment was blinded, the clinical response was only analysed as a secondary outcome parameter. Obviously, a double-blind controlled trial would have been preferable, but was not feasible for logistic and economic reasons. Sulfasalazine was chosen because this was the only non-biological conventional drug for which there were some response signals in previous trials with active AS patients failing NSAID therapy,44,–,47 justifying a 1-year treatment phase. Despite the limitations of the interpretations of the clinical results because of the open-label design, there were some interesting results (table 3). In this cohort of early axial spondyloarthritis patients ASAS partial remission was reached in 50% of patients already after 24 weeks and maintained over 48 weeks, a result very similar to the 55.5% remission rate in the other early axial spondyloarthritis trial,10 clearly indicating that a remission rate similar to that found in early rheumatoid arthritis48 can also be achieved in early axial spondyloarthritis patients treated with a TNF blocker. In a previous adalimumab trial in those patients with non-radiographic axial spondyloarthritis7 with a disease duration less than 3 years, the remission rate was close to the figure reported here, indicating that the symptom duration may be more relevant than the presence or absence of chronic changes seen by x-rays.7
When MRI and clinical data were correlated, all six patients in the etanercept group who became free from any active MRI inflammation were also in clinical remission (out of 20), although neither of the two patients in the sulfasalazine group was in remission. Also the mean sacroiliac joint score had a greater reduction in the etanercept patients reaching remission (from 8.4 to 1.8) than in the whole etanercept group (from 5.4 to 3.5). A similar difference in correlation with the clinical response was not seen in the sulfasalazine group. It remains to be seen whether the number of patients who become free of any bony inflammation will increase if patients are treated with a TNF blocker beyond 1 year. Interestingly, a significant correlation between change in MRI sacroiliac joint scores and BASDAI and BASFI was observed for the first time.
These data indicate that the differences seen in the clinical response rate between the etanercept and the sulfasalazine groups might be real, and that there is a correlation between bony inflammation on MRI and clinical response, as nicely shown in the very good etanercept responders. A planned follow-up of those patients who are free of symptoms and of inflammation on MRI will address the question of how many of these patients will have reached drug-free remission. Furthermore, an additional analysis of structural changes as shown on the T1 sequence of the MRI will cast more light on the rather complex interaction between inflammation and structural damage in this disease.49
The observed clinical effect found in the sulfasalazine arm did not exceed the observed placebo remission response of 12.5% at week 16 in the trial of Barkham et al10 or the observed sulfasalazine remission response of 15.5% at week 16 in a recent double-blind trial in active AS patients comparing etanercept with sulfasalazine.50 The small improvement of MRI inflammation, as observed in the sacroiliac joints but not in the spine or entheses, might be by chance. Therefore, both the blinded MRI data and the unblinded clinical data support earlier evidence51 that sulfasalazine does not appear to play an important role in the treatment of AS and/or early axial spondyloarthritis.
Interestingly, although in earlier AS trials short disease duration, elevated CRP and positive MRI were predictors of a good clinical response,5,–,7 no such predictors were found in the current study, most probably because only patients with a short disease duration and positive MRI were included, which are themselves already strong predictors of a good response.
In conclusion, in this early axial spondyloarthritis trial over 1 year, etanercept, in comparison with sulfasalazine, improved bony inflammation at different sites of the skeleton considerably, in parallel to an observed clinical improvement. These results suggest that TNF blockers in axial spondyloarthritis patients are effective when patients are treated early.
Acknowledgments
The authors would like to thank Beate Buss, Gabriela Schmittat, Kirsten Karberg, Jan Brandt, Eugen Feist, Jan Zernicke, Barbara Wenzel, Carmen Herz, Corinna Beer, Angela Seifert, Rieke Alten, Svetlana D’jacenko, Christof Pohl, Marina Heese, Silke Zinke, Kristin Lunkwitz, Ulrich Prothmann, Ute Alpermann, Thilo Klopsch, Frank Mielke and Martina Stoll for performing the studies. The authors also thank Sabine Achtelstetter and Anja Weiss for data preparation and statistical analysis. They would also like to thank Torsten Diekhoff for blinding and the preparation of magnetic resonance images.
References
Footnotes
-
Funding This study was supported by an unrestricted grant from by Wyeth, which was acquired by Pfizer Inc in October 2009.
-
Competing interests IS and HH: Wyeth Pharmaceuticals, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals: consulting fees or other remuneration. GB, MR and JS: Wyeth Pharmaceuticals, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals, UCB: consulting fees or other remuneration. AK: Wyeth Pharmaceuticals, Schering Plough, Abbott Immunology Pharmaceuticals: consulting fees or other remuneration. MB: Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals: consulting fees or other remuneration. BF: Former employee of Pfizer/Wyeth. KGH, CA and JL: none.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Landesamt für Gesundheit und Soziales, Geschäftsstelle der Ethik-Kommission des Landes Berlin, Sächsische Strasse 28, 10707 Berlin, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous