Article Text

Abstract
Objectives To develop and validate a paediatric-targeted MRI scoring system for the assessment of disease activity and damage in juvenile idiopathic arthritis (JIA). To compare the paediatric MRI score with the adult-designed. Outcome Measures in Rheumatology Clinical Trials—Rheumatoid Arthritis MRI Score (RAMRIS), whose suitability for assessing growing joints was tested.
Methods In 66 patients with JIA the clinically more affected wrist was studied. Thirty-nine patients had a 1-year MRI follow-up. Two readers independently assigned the paediatric score and the RAMRIS to all studies. Validation procedures included analysis of reliability, construct validity and responsiveness to change. A reduced version of the bone erosion score was also developed and tested.
Results The paediatric score showed an excellent reproducibility (interclass correlation coefficient >0.9). The interobserver agreement of RAMRIS was moderate for bone erosions and excellent for bone marrow oedema (BMO). The paediatric score and RAMRIS provided similar results for construct validity. The responsiveness to change of the paediatric score was moderate for synovitis and bone erosion, and poor for BMO and did not improve when RAMRIS was applied. The reduced version of the bone erosion was valuable for the assessment of joint damage, and provided time-saving advantages.
Conclusion The results demonstrate that the paediatric MRI score is a reliable and valid method for assessing disease activity and damage in JIA. Unexpectedly, the RAMRIS provides acceptable suitability for use in the paediatric age group. Further work, especially in a longitudinal setting, is required before defining the most suitable MRI scale for assessing growing joints.
Statistics from Altmetric.com
Introduction
The availability of new effective drugs for the treatment of juvenile idiopathic arthritis (JIA),1,–,4 has increased the need for imaging tools to monitor changes in inflammatory activity, identify pre-erosive features and detect early bony changes. MRI, by enabling evaluation of soft tissue inflammatory changes and osteochondral damage, has proved useful in the assessment of rheumatoid arthritis (RA).5,–,10 In the past decade there has been a great deal of effort by the Outcome Measures in Rheumatology Clinical Trials (OMERACT) RA-MRI working group aiming to quantify the large amount of information produced by MRI, and culminating in the development of a semiquantitative scoring system (Rheumatoid Arthritis MRI Score (RAMRIS)) for the assessment of inflammatory and damage abnormalities in RA.11 Owing to the peculiarities of the growing skeleton, it is commonly believed that scoring methods designed for patients with RA, may not be suitable for the evaluation of patients with JIA. However, to date the adult-designed RAMRIS system has never been tested in the paediatric age group. We recently devised an MRI scale for the assessment of bone erosion in JIA, that was highly reproducible in a small sample of patients.12
The aims of this study are (1) to set up a paediatric-targeted MRI scoring system that includes the evaluation of synovitis and bone marrow oedema (BMO), besides bone erosions, and provide preliminary evidence of its reliability and validity in a large group of patients with JIA; (2) to compare the paediatric MRI scoring system with the adult-designed RAMRIS, and to test the suitability of RAMRIS when applied to a paediatric populations.
Patients and methods
Sixty-six patients with JIA, diagnosed according to the International League of Associations for Rheumatology revised criteria,13 and with wrist arthritis were consecutively recruited from the study unit between June 2006 and June 2008. All the patients willingly agreed to participate. Patients requiring sedation to perform MRI, or patients with contraindication to MRI were not included. The clinically more affected wrist was studied with MRI and radiography, coupled with standard clinical assessment. Clinical and radiological examinations were performed on the same day. Thirty-nine patients, enrolled during the first year of the study, had a follow-up MRI a median of 1.2 years (first to third quartile: 1.0–1.4 years) after the baseline. The Gaslini Institutional review board approved the study, and informed written consent was obtained from a parent of each child.
Clinical assessment included count of active joints, joints with swelling, pain on motion/tenderness and limitation on motion14; physician's global assessment of disease activity; functional ability assessment through the Childhood Health Assessment Questionnaire15 16; parent's global assessment of the child's wellbeing; parent's rating of the child's intensity of pain; erythrocyte sedimentation rate (Westergren method); C-reactive protein (nephelometry). The Juvenile Arthritis Damage Index Articular score (JADI-A) was used to assess the articular damage,17 and the Juvenile Arthritis Disease Activity Score for 71 joints (JADAS-71)18 for disease activity assessment. A detailed scoring of the imaged wrist was performed: swelling and tenderness were graded from 0 to 3, while limitation of motion was graded from 0 to 4.14 Clinical measures were assessed by paediatric rheumatologists (SV, AB), who were blinded to the results of imaging. Patients with the 1-year follow-up visit were classified as improved or not improved according to the American College of Rheumatology Paediatric 30 criteria.19
Imaging assessment
Computed radiographs of the wrists were scored according to the adapted version Sharp/van der Heijde score20 and to the Poznanski's score.21
MRI was performed on a 1.5 T MRI scanner (Achieva Intera; Philips Medical Systems, Best, The Netherlands) using a Sense Flex Small Coil, with a field of view covering from distal radioulnar joint to the metacarpal bases. Details of the sequences are given in figure 1.
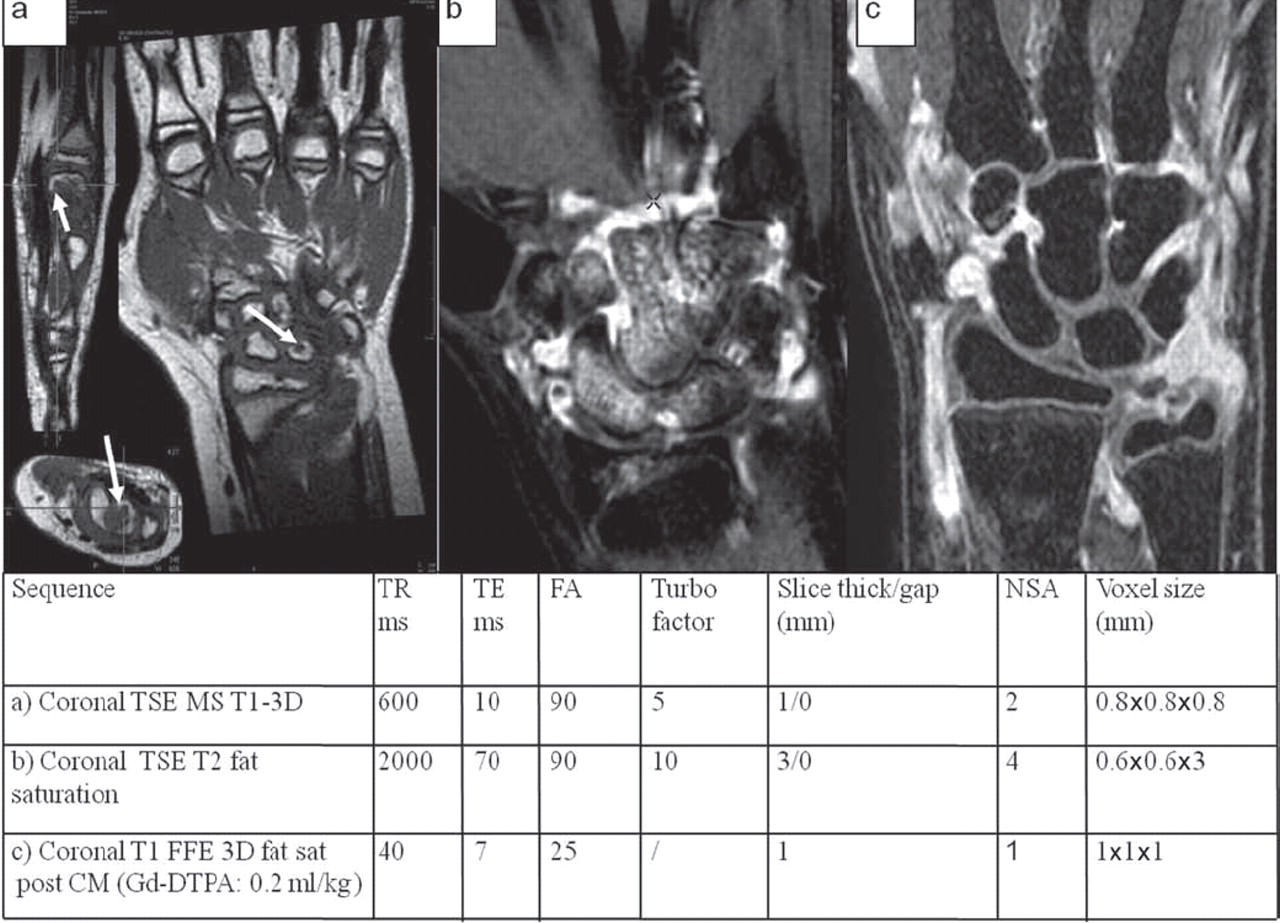
Wrist MR images and parameters of the MRI sequences of different patients with juvenile idiopathic arthritis (JIA) and wrist involvement. (A) Coronal TSE MS T1-weighted MRI with multiplanar reconstruction of the carpus in a patient with JIA. The bone erosion, visible in the lunate in the coronal plane (arrow), is confirmed in the multiplanar reconstruction (arrow in the axial and saggital planes). (B) Coronal TSE fat-saturated T2-weighted image in a second patient with JIA: bone marrow oedema involving the scaphoid, the capitate, the hamate, the trapezoid and the lunate is clearly evident. (C) Contrast-enhanced coronal FFE 3D fat-saturated T1-weighted image in a third patient with JIA and active wrist involvement: the presence of synovitis in the radioulnar, radiocarpal and intercarpal joint recesses is evident. CM, contrast medium; FFE, fast field echo; NSA, number of sample averages; TE, echo time; TR, repetition time; TSE, turbo spin echo.
MRI scoring
A paediatric-targeted MRI scoring system was devised by a consensus between paediatric rheumatologists (CM, AR, NR, AM) and radiologists (MBD, MV, GMM, PT) with 3 to >20 years' expertise in musculoskeletal MRI, following the OMERACT RAMRIS recommendations and the OMERACT MRI definitions of pathological features in RA joints.11 22 23 The RAMRIS scales for bone erosion (range 0–10) and BMO (range 0–3) were considered unsuitable for the assessment of children with JIA owing to the small size of the carpal bones and their significant changes during skeletal development. Bone erosions were scored at 15 sites within the carpus (carpal bones, distal radius, distal ulna and metacarpal bases) using a recently devised 0–4 scale (0=no erosion; 1=1–25% of the bone eroded; 2=26–50% of the bone eroded; 3=51–75% of the bone eroded; 4=76–100% of the bone eroded).12 Scoring bone erosion can take an average of 12 min per scan, ranging from 5 to 22 min, based on the degree of damage. Aiming to increase the feasibility of the erosion scale, a reduced version of MRI erosion score was developed. BMO was evaluated using a 0–2 scale (0, no oedema; 1, <50% of the bone involved; 2, ≥50% of the bone involved) on the same site as for bone erosions. The degree and extent of synovitis were assessed using the RAMRIS synovitis score.11
Reading strategy
Two readers (MBD and CM), blinded to patient's identity and clinical status, independently assigned the paediatric-targeted MRI score and the RAMRIS system to all studies. All images were read on large-screen (21”) radiological workstation monitors using a standard PACS software program, after training and calibration sessions. The 1-year follow-up MRI scans were scored without reference to baseline, as the readers were blinded to the chronological order of the examinations.
Statistical analysis
Comparison between groups was performed using the Mann–Whitney U test (two groups) or the Kruskal–Wallis test (three groups). Comparison of paired quantitative data at baseline with respect to 1-year follow-up was made by the Wilcoxon test.
In order to develop a reduced version of the MRI erosion score we performed (1) an internal consistency analysis with the computation of Cronbach's α24 for the complete set of carpal bones versus Cronbach's α after removing one bone in turn; (2) the correlation between the erosion score assigned to each carpal bone and the total erosion score of the scale calculated excluding the single bone in turn from the total (‘adjusted item-total correlation’ or ‘correlation corrected for overlap’)25; (3) the inter-reader agreement for each carpal bone by computing Cohen's k coefficient.26
Interobserver reliability was assessed for the 66 MRIs scored by the two observers. All the 66 MRIs were re-scored a second time, in a blinded manner 24 weeks after the previous review, in order to assess the intraobserver reliability. Inter- and intraobserver agreement were analysed by computing the intraclass correlation coefficient (ICC)27 and the agreement was classified as follows: ICC<0.4=poor, ≥0.4–0.80=moderate and ≥0.80=good agreement. Construct validity examines whether the construct in question is related to other measures in a manner consistent with a priori prediction. Given that the MRI erosion score is a measure of damage, it was predicted that the correlation of its value with standardised measures of damage would be in the moderate-to-high range. Correlations with disease activity parameters were predicted to be poor. Given that the MRI synovitis score is a measure of disease activity, it was predicted that the correlation of its value with disease activity parameters would be in the moderate-to-high range. No predictions were made for correlation with the BMO score. All correlations were assessed using Spearman's rank order correlation coefficient (rs).28 Responsiveness was evaluated by the standardised response mean (SRM), which is calculated by dividing the absolute mean change in score by the SD of an individual's change in score. The threshold levels for SRM were defined as follows: ≥0.20=small, ≥0.50=moderate, ≥0.80=strong.29 Statistical analysis was performed with Statistica (StatSoft, Tulsa, Oklahoma, USA) and the internal consistency analysis was conducted with XLStat software.
Results
Sixty-six patients with JIA (15 boys, 51 girls) were included. Twenty-three patients had systemic arthritis, 22 had polyarthritis (seven were rheumatoid factor positive), 17 had extended and four persistent oligoarthritis. Table 1 summarises the results of the baseline clinical and imaging assessment. At baseline, 55/66 (83.3%) patients had erosions detected by MRI. By contrast conventional radiography identified erosions in 23/66 (34.8%) patients. BMO was visualised on 55/66 (83.3%) MRI scans, with a distribution within the carpus similar to that of bone erosions (figure 2). Synovitis was detected in 60/66 (90.9%) patients. The degree of synovitis, BMO and bone erosion was not significantly different among the JIA subtypes.

Distribution of erosive changes and bone marrow oedema within the carpus. Bone marrow oedema lesions were found in the same subarticular locations as erosions within the carpus. MC, metacarpal.
Baseline clinical features, medication details and radiological findings of the 66 patients enrolled
A reduced version of the paediatric erosion score was devised on the basis of the internal consistency analysis of the original score. Cronbach's α (0.894) remained substantially stable after removing I, IV and V metacarpal bases, pisiform and distal ulna (α10 bones=0.887). Adjusted item-total correlations were very poor for the I (rs=0.396), IV (rs=0.323) and V (rs=0.398) metacarpal bases, pisiform (rs=0.197) and distal ulna (rs=0.251). Cohen's k coefficient, calculated for each carpal bone, showed a lower inter-reader agreement for the IV (kCohen: 0.56), V metacarpal bases (kCohen: 0.25) and distal ulna (kCohen: 0.56) than for the other bones. The correlation between the 15-bones erosion score versus the 10-bones reduced erosion score was extremely high (rs=0.99), demonstrating that the reduced version is almost superimposable on the original score. By applying the reduced version, the scoring of bone erosions is, on average, reduced by 5 min per scan.
Reliability
The inter- and intraobserver agreement (as assessed by ICC) for bone erosions, BMO and synovitis scores, as well as the interobserver agreement for the score changes between baseline and follow up MRI are reported in table 2.
Interobserver and intraobserver agreement of the bone erosion, bone marrow oedema and synovitis scores
Construct validity
As the inter-reader agreement was excellent, the independent scores of the two observers for each MRI were averaged, and this average was used for the analyses of the construct validity. The paediatric MRI erosion score was significantly higher in patients with higher wrist limited range of motion score (p=0.0002), and showed a significant correlation with the radiographic damage, and with clinical indicators of damage, such as JADI-A. As summarised in table 3, similar correlations were found using both the reduced version of the MRI erosion score, and the RAMRIS scale. As predicted, MRI erosion scores correlated poorly with disease activity measures. MRI BMO score (range 0–2) correlated significantly with the MRI erosion score (rs=0.63), with the Sharp/van der Hejde and the Poznanski scores, and with the JADI-A; also RAMRIS BMO score was highly correlated with radiographic damage, and moderately correlated with JADI-A. The MRI synovitis score was significantly higher in patients with higher wrist swelling score (p<0.0001), and, as predicted, was moderately correlated with clinical measures of disease activity, such as the total count of swollen joints, the JADAS-71 and the physician's global assessment of overall disease activity; no correlation were found between the synovitis score and the clinical indicators of damage.
Spearman's correlation between synovitis, bone marrow oedema, bone erosion scores and JIA clinical measurements of disease activity and damage
Sensitivity to change
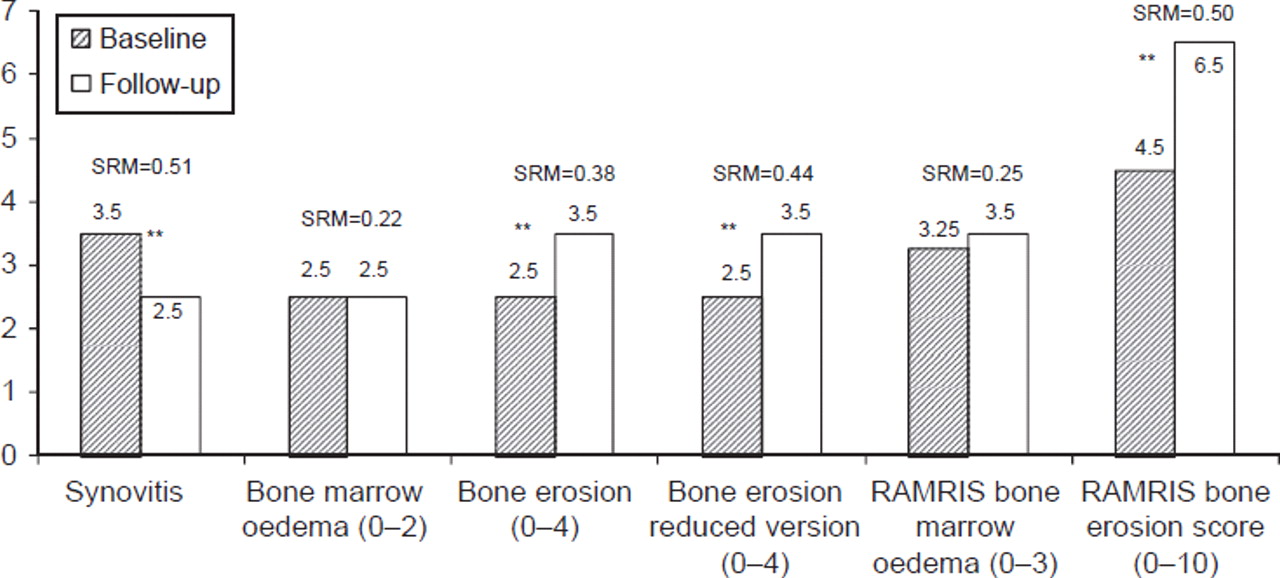
Sensitivity to change was assessed by calculating the SRM in the 39 patients who had a 1-year follow-up MRI (figure 3). The average between the independent MRI scores of the two observers were used for the analyses. Notably, patients who met the clinical definition of improvement according to the American College of Rheumatology Paediatric 30 criteria (N=22),19 showed a significant decrease in 0–2 BMO score (p=0.04; SRM=0.44), a decrease in RAMRIS 0–3 BMO scores, without reaching statistical significance (p=0.30; SRM=0.35) and a statistically significant decrease in MRI synovitis score (p=0.01; SRM=0.62). Conversely, patients who did not improve clinically (N=17), showed a significant increase in paediatric erosion scale (p=0.03; SRM=0.57), in reduced version bone erosion (p=0.03; SRM=0.58) and in RAMRIS erosion scores (p=0.03; SRM=0.58). Surprisingly, a significant increase in erosion score (p=0.01; SRM=0.6) was also found in clinically improved patients, when the RAMRIS erosions scale was applied.

{kind=link}
{kind=link}
{kind=link}
Baseline and follow up median values of each component of MRI scores and results of responsiveness (SRM) of the 39 patients who had a 1-year follow-up MRI. A significant decrease in synovitis score (p=0.005; SRM=0.51) and a significant increase in bone erosion scores (version 0–4; p=0.007; SRM=0.38 and Rheumatoid Arthritis MRI Score (RAMRIS) 0–10 score, p=0.004; SRM=0.5) was observed from baseline to the follow-up observation time; the change in bone marrow oedema scores did not reach statistical significance either in the version 0–2 (p=0.48; SRM=0.22) or in the RAMRIS 0–3 version (p=0.35; SRM=0.25). SRM, standardised response mean.
Discussion
MRI, providing information on all joint structures, is being increasingly used in RA for diagnosis, prognostication and monitoring responses to treatment.10 30 31 Since the MRI system designed for adults with RA may not be suitable in children (growing joints change anatomically over time, especially those of the wrist), we devised a paediatric-targeted MRI scoring system for the assessment of disease activity and damage in children, and compared its performance with the widely accepted adult-designed RAMRIS in a group of patients with JIA. Confirming our previous findings,12 the paediatric MRI erosion score (range 0–4) showed an excellent intra- and inter-reader reliability, correlated significantly with conventional measures of damage, and correlated poorly with active disease parameters, providing supportive preliminary evidence for the construct validity of the proposed score. The lack of a significant correlation with the Childhood Health Assessment Questionnaire score might be because this measure was found to reflect both disease activity and damage.32
MRI bone erosions progressed significantly at 1-year follow-up scans, but the responsiveness to change of the paediatric erosion score was poor. A major limitation of the proposed scale, is the lack of grading of erosive changes affecting <25% of the bone, which may hamper responsiveness to change over time. Surprisingly, the RAMRIS erosion scale, with its wider range of score, which potentially allows a more detailed description of even minute changes in erosion size, did not increase the sensitivity of the score for detecting erosive progression, while the inter-reader agreement for interpretation of erosive changes decreased. Notably, the levels of reliability of the RAMRIS obtained in this study were comparable, and even higher, than those published in studies on patients with RA.6 33
Several factors may have contributed to the less than satisfactory responsiveness to change of both the paediatric and RAMRIS erosion scores. In this study the images were read without reference to baseline and blind to the chronological order of the scans. Van der Heijde et al34 found that the method of reading images paired and in chronological sequence is the most sensitive to change in radiographic studies. Again, patients with either early or established disease were analysed. Rossi et al35 found that the progression of radiographic damage in patients with JIA tended to decrease after the first year of the disease. Finally, the addition of radiographic assessment to obtain better accuracy in identifying patients with disease progression, might improve the potential of the MRI erosion scores to detect longitudinal structural changes, and be helpful in interpreting the unexpected increase of erosion score that we found in clinically improved patients by using the RAMRIS. However, only longitudinal imaging follow-up will allow us to establish whether the RAMRIS scale has a better potential to detect progressive erosive disease than the 0–4 score, or leads to more false positive results, when used for the assessment of growing joints
Since the MRI erosion score is quite extensive and its application time consuming, we developed a reduced version in order to increase its clinical applicability. This study showed that the exclusion of some carpal bones did not modify the final judgement on joint damage, hence providing time-saving advantages.
The RAMRIS synovitis score proved to be a valid and reliable score for the assessment of synovitis in JIA. The poor correlation of the score with the acute phase reactant values is hardly surprising,36 37 and could be related to the fact that C-reactive protein and erythrocyte sedimentation rate indicate a systemic inflammation, while MRI shows the inflammatory status in a specific area studied. On the other hand, the correlations with swollen joint count, physician's global disease activity and JADAS-71 are encouraging, supporting the utility of the wrist as a surrogate marker for total burden of disease activity. It should be recognised, however, that because in this study we assessed only the wrists joint, our findings are of value only for patients with wrist disease. In this study the responsiveness to synovial change was lower than the results obtained in studies on adults with RA receiving anti-tumour necrosis factor α therapy.38 39 A lower responsiveness, however, should be expected in a longitudinal observational study, in which patients do not receive homogeneous treatment regimen (like in this cohort), than in an intervention study, in which all the patients receive drugs targeted at suppressing inflammation, such as the new biological regimens.
One of the more intriguing aspects of MRI is the ability to visualise BMO. Longitudinal studies have demonstrated that BMO is a key predictor of erosive progression and functional outcome in patients with RA.40,–,44 Even if the real meaning of BMO in JIA remains unknown, the overall high levels of concordance between the BMO score and standardised measurement of radiographic damage, and the distribution of BMO lesions in the same subarticular locations as erosions, gave supportive, preliminary evidence for a strict link between BMO and erosive damage also in JIA. The 0–2 version of the BMO score appeared to be, overall, advantageous compared with the RAMRIS version, especially in the longitudinal setting. We observed a significant decrease in the BMO score, in clinically improved patients, only when the 0–2 version was applied. Before establishing the most suitable score for assessing BMO in JIA, these results should be corroborated in larger longitudinal studies aiming to elucidate the significance of BMO in the assessment of treatment efficacy, as well as its prognostic value.
The lack of data from age-matched healthy controls is one of the limitations of this study. Such data would have strengthened the study, reducing the possibility of scoring normal joints as pathological (ie, minimising the difficulties in discriminating bone irregularities due to the growing ossification process from irregularities caused by the disease).
We concluded that the proposed paediatric-targeted MRI scoring system is a reliable and valid method for assessing disease activity and damage in JIA, and therefore could represent a useful framework for further development of MRI assessment of JIA. Unexpectedly, overall, the RAMRIS system provided acceptable suitability for use in children. Further work, especially in a longitudinal setting, is required in order to determine the best combination of the available MRI scales, and thus define the most suitable scoring system for the assessment of JIA.
Acknowledgments
The authors wish to acknowledge the technical staff of the radiological department of the G Gaslini Institute, in particular Mrs Francesca Maiuri, Mr Paolo Del Mirto, Mr Stefano Franceschi and Mr Marco Ciccone, who supervised the MRI scans.
References
Footnotes
CM and MBD contributed equally to this article.
-
Funding This study was supported by a grant from the European Union, Health-e-Child Integrated Project (IST-2004-027749). IV and MI were recipients of the European League Against Rheumatism (EULAR) scientific training bursaries.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the local ethics committee of the Istituto G Gaslini, Genova, Italy.
-
Provenance and peer review Not commissioned; externally peer reviewed.