Article Text

Abstract
Background Gout therapy includes xanthine oxidase inhibitors (XOI) and colchicine, which have both been associated with decreased cardiovascular risk. However, their effects on major cardiac events, such as myocardial infarction (MI), need to be investigated further.
Objectives To investigate whether XOIs and colchicine are associated with decreased risk of MI.
Methods This case-control study compared patients with first-ever MI and matched controls. Cases were recruited from the Pharmacoepidemiological General Research on MI registry. Controls were selected from a referent population (n=8444) from general practice settings.
Results The study sample consisted of 2277 MI patients and 4849 matched controls. Use of allopurinol was reported by 3.1% of cases and 3.8 of controls, and 1.1% of cases and controls used colchicine. The adjusted OR (95% CI) for MI with allopurinol use was 0.80 (0.59 to 1.09). When using less stringent matching criteria that allowed for inclusion of 2593 cases and 5185 controls, the adjusted OR was 0.73 (0.54 to 0.99). Similar results were found on analysis by sex and hypertension status. Colchicine used was not associated with a decreased risk of MI (aOR=1.17 (0.70 to 1.93)).
Conclusions Allopurinol may be associated with a reduced risk of MI. No decreased risk of MI was found in colchicine users. Besides its urate-lowering property, allopurinol might have a cardioprotective effect.
- Gout
- Cardiovascular Disease
- Treatment
Statistics from Altmetric.com
Introduction
Gout is caused by deposition of monosodium urate crystals in joints after chronic hyperuricaemia.1 Recent epidemiologic studies have shown an increased prevalence of gout2 that may be attributed to shifts in diet and lifestyle, improved medical care, and increased longevity.
The disease is strongly associated with several comorbidities and particularly traditional vascular risk factors. Indeed, recent estimates indicate that among individuals with gout, about two-thirds have hypertension, half are obese, one-half have diabetes.3 Cardiovascular diseases are the greatest threat for patients with gout. Evidence from prospective and interventional studies of various populations suggests that gout and hyperuricaemia are independent risk factors for cardiovascular diseases.2–5 Hyperuricaemia and gout are associated with increased risk of myocardial infarction (MI),6 peripheral artery disease7 and death primarily due to elevated risk of cardiovascular diseases.8–10 The mechanisms linking hyperuricaemia and gout with cardiovascular events are unclear but may include oxidative stress generated by xanthine oxidase (XO),11 the enzyme that catalyses the formation of urate. Other explanations are a direct contribution to endothelial dysfunction12 and low-grade inflammation associated with increased urate levels and tophi.13 ,14
In addition to requiring symptomatic treatment of acute gout attacks, nearly all gout require long-term urate-lowering therapy (ULT).15 ,16 Therefore, knowledge of the effects of these drugs on the cardiovascular system is of major interest. Allopurinol, and the most recent introduced drug, febuxostat, are the sole available XO inhibitors (XOI). In addition to their urate-lowering effects, XOIs may have a beneficial effect on the cardiovascular system by decreasing oxidative stress in the vasculature.11 Interestingly, colchicine use, for treating acute gout attacks,17 has been associated with decreased prevalence of MI.18 To further investigate the impact of ULT and colchicine on MI, we conducted a large case-control study to assess the association of use of these drugs and risk of MI.
Patients and methods
Ethics approval
This study was approved by the French Departmental Directorate of Health and Social Affairs and received approval from the ethics committees and CNIL (Commission nationale de l'Informatique et des Libertés), the French Data Protection Authority. It was conducted in accordance with the Declaration of Helsinki and the Guidance for Good Clinical Practice. All participants gave their written informed consent to participate in the study.
Study population
This case-control study involved data collected by the pharmacoepidemiological information system Pharmacoepidemiological General Research extension (PGRx). The PGRx design has been detailed elsewhere.19 Eligible cases and controls were aged 18–79 years, able to read French and participate in a telephone interview. Subjects were excluded if they had a history of MI, angioplasty, coronary artery bypass surgery, any other coronary artery disease or stroke.
Cases
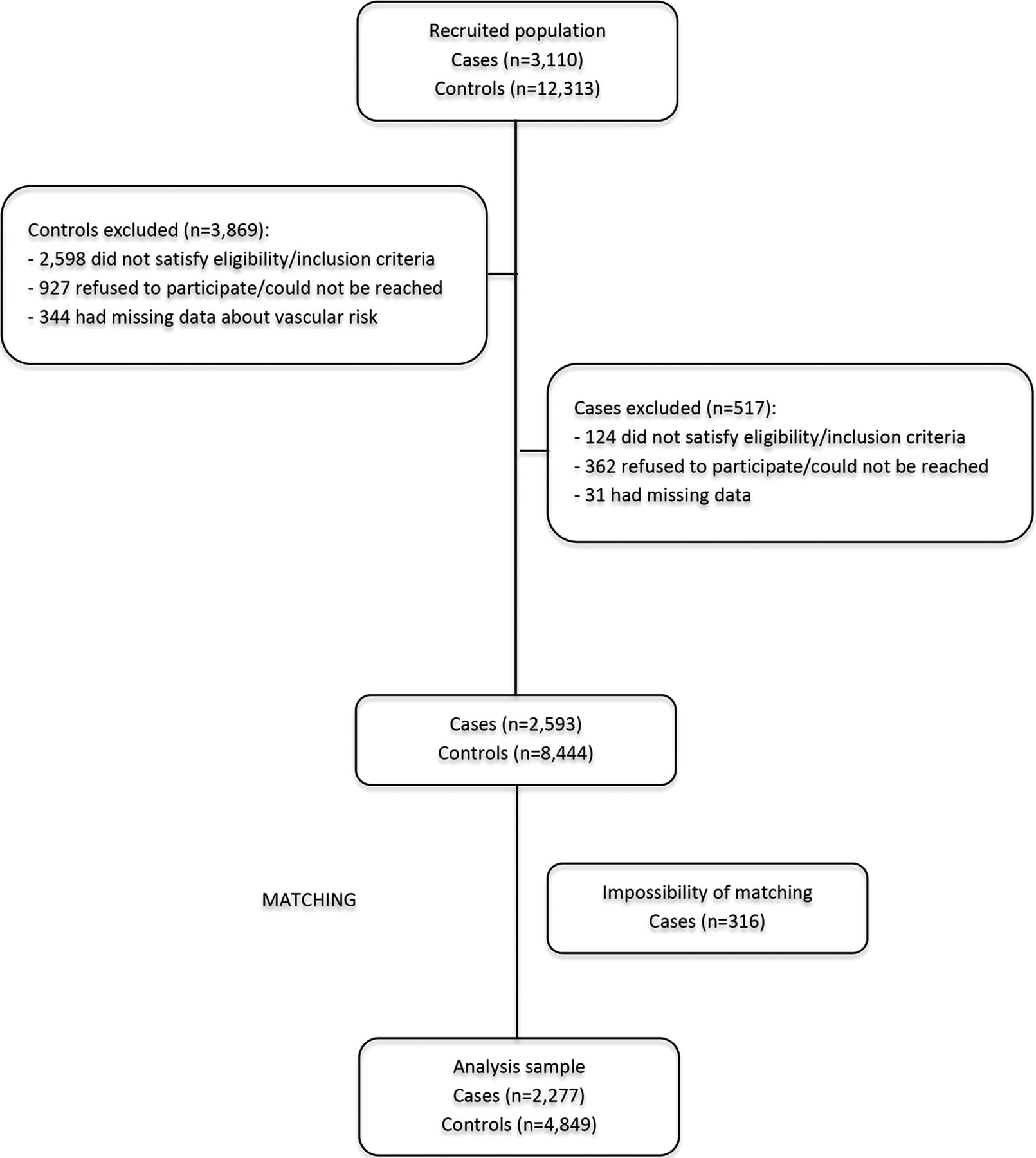
Cases were patients with a first-ever non-fatal MI successively referred to one of 63 cardiology centres throughout France between 15 March 2007 and 30 November 2010. The time between the first symptoms of MI and the date of recruitment should not exceed 1 month. The diagnosis of MI was based on the presence of at least two of the following criteria: characteristic thoracic pain, electrocardiography showing Q-wave and/or ST-segment elevation in at least two adjacent derivations, and levels of creatine phosphokinase-muscle band and/or troponin elevated by at least twice the normal values. Clinical research assistants randomly audited the centres for compliance with the study protocol. Among 3110 eligible patients, 517 (17%) were excluded because 124 did not satisfy eligibility/inclusion criteria, 362 refused to participate or could not be reached for the interview, and 31 had missing data for vascular risk factors, particularly hypertension (figure 1). Finally, 2593 cases were available for matching with controls.

Flow diagram of the selection of cases and controls.
Controls
A total of 420 general practitioners (GP) from the same regions as the cardiology centres participated in recruiting controls from the referent population. GPs were randomly selected by region from a national list of GPs in France. The referent population consisted of all eligible successive patients seen by the participating GPs from 15 March 2007 to 31 January 2011, with no restriction on reasons for consultation. Among the total referent population (n=12 313), 3869 were excluded for the following reasons: 2598 did not satisfy eligibility/inclusion criteria, 927 refused to participate or could not be reached, and 344 had missing data on vascular risk factors (figure 1). Controls were randomly chosen from the 8444 remaining referents and matched with cases by sex, age (±5 years), history of hypertension, and number of visits to the GP during the year preceding the index date (0–1, 2–12, ≥13 visits). The date of consultation should be as close as possible to the date of MI for cases (and should not exceed 365 days). The objective was to recruit, whenever possible, three controls per case using an iterative matching process with a control dropped from the pool after matching. Using these matching criteria, the study sample consisted of 4849 controls and 2277 cases, as no control was found for 316 cases. The mean number of controls per case was 2.1; 893 cases were matched with 3 controls, 786 with 2 controls, and the remaining 598 cases with 1 control. To increase the power of the study for investigating the impact of allopurinol on risk of MI, we then used the total sample of cases. For this, we excluded from the matching criteria the number of visits to the GP during the year preceding the index date. Using sex, age and hypertension as matching criteria, 2593 cases and 5185 controls were available for this analysis.
Data collection
For cases and controls, physicians had to complete an electronic medical data form that collected medical information about the patient: chronic vascular diseases or vascular risk factors (eg, hypertension, diabetes), other comorbidities including gout, biological data and current and previous (past 2 years) prescriptions. Of note, urate levels were not recorded in the registry. We obtained data on physician prescriptions for 95.6% of referents and 74.8% of cases. Hypertension was defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg or history of hypertension (as reported by the physician) associated with one of the following cardiovascular drug classes used in the previous 2 years: β-blockers, angiotensin-converting enzyme inhibitors, calcium channel blockers, angiotensin II receptor antagonist, diuretics or central antihypertensive medications. Patients with a history of diabetes (as reported by the physician) or who had used antidiabetes drugs in the previous 2 years were considered as having diabetes. Clinical, biological and ECG data about MI cases were obtained from the cardiology centres. Each participant was interviewed by telephone by trained interviewers who were blinded to case or control status. Participants were asked about their socioeconomic status, occupation, frequency of consultation with the physician during the last 12 months, smoking history (never/ever), alcohol consumption (regularly vs occasionally or never), physical activity (> 30 min/day: yes/no), and height and weight (for calculating Body Mass Index (BMI)). They answered a detailed questionnaire about past and present medical history. Before the interview, participants had been sent a guide that included a list and a visual display of packaged drugs.
Self-reported data on all drugs used (prescriptions and over-the-counter drugs) for the last 2 years were collected for three successive periods: last two preceding months, 3 months to 1 year, and 1 to 2 years. Data were collected on the dose and regularity of use (regular vs occasional) during each period. Drugs were coded by use of the Anatomical Therapeutical Chemical classification. Validation of the methodology for analysing the agreement between patients' reports and physicians’ prescriptions from the PGRx registry has been published recently.20 ,21
Statistical analysis
The distribution of vascular risk factors was computed for cases and controls, and conditional logistic regression estimates of adjusted ORs and 95% 95% CIs were used to examine the association of classical cardiovascular risk factors and MI risk. Crude and adjusted ORs and 95% CIs were computed to assess the association of ULT drug or colchicine intake and MI risk. Allopurinol use was defined by two variables: a binary variable (at least one allopurinol intake in the 2 years before index date: yes/no) and a three-class variable that took into account the daily dose (≥200 mg daily, <200 mg, no use). The low number of patients who took 300 mg allopurinol precluded analysis of this subgroup. Colchicine was defined by one variable (at least one colchicine intake in the 2 years before index date: yes/no). The following factors were included in the adjusted model: diabetes, obesity, gout, physical activity, smoking, alcohol consumption, and intake of NSAIDs, β-blockers, angiotensin-converting enzyme inhibitors, calcium channel blockers, angiotensin II receptor antagonists, diuretics, central antihypertensive medications, statins and antiplatelet drugs. Unadjusted and adjusted models were first run considering allopurinol use (binary and three-class variables), then colchicine use.
To assess the robustness of the results of the core analysis with allopurinol, data were stratified by sex and hypertension. We also examined whether the association between allopurinol and MI risk depended upon the type of MI: with ST elevation (STEMI) or without ST elevation (NSTEMI) on electrocardiography. Polytomous logistic regression was used to estimate adjusted ORs and 95% CI for each type of MI. Lastly, as fatal MI cases were not included in our study, we attempted to explore a potential survival bias by comparing allopurinol use in MI cases presented with a resuscitated cardiac arrest (‘near-deaths’) and their matched controls. The proportion of missing data never exceeded 2%. In multivariate models, missing data were imputed by mode or mean by sex and age group. Statistical analysis involved use of SAS V.9.2 (SAS, Cary, North Carolina, USA). A p value <0.05 was considered significant.
Results
Characteristics of participants
The 2277 cases with first-ever MI and their 4849 matched controls had a mean age of 59.3 years (SD: 11.6), 76.4% were men and 56.3% were hypertensive. Prevalence of gout, as reported by the physicians, was 0.9% and 0.6% in controls and cases, respectively. MI cases showed classical vascular risk profile (table 1). High BMI, diabetes, smoking (ever) and minimal physical activity were more frequent for cases than controls. On multivariate analysis, all factors were independently associated with MI (p<0.05 for all adjusted ORs).
Demographic characteristics and cardiovascular risk factors of myocardial infarction (MI) cases and matched controls
Association of allopurinol use and MI
Allopurinol was by far the most frequent ULT taken by participants. Indeed, no case and only 0.1% of controls reported use of febuxostat, and no participant took uricosurics. In all, 3.1% of cases and 3.8% of matched controls reported allopurinol use during at least one period within the two preceding years. Among allopurinol users, most (90% of cases and 92% of controls) had taken the drug regularly (at least 5 days per week) during the preceding 2 years. About two-thirds of cases and controls took a daily dose ≥200 mg, whereas 19% of cases and 25% of controls took ≥300 mg.
When adding all vascular risk factors to the conditional logistic regression model, the adjusted OR (aOR) for MI was at the limit of the significance: aOR=0.80 (0.59 to 1.09) (table 2). When the number of visits to the GP was excluded from the matching criteria in order to use the whole cases pool (n=2593) and their 5185 matched controls, the aOR was 0.73 (0.54 to 0.99). We then categorised allopurinol use by dosage (no use, <200, ≥200 mg) and found no association of allopurinol dose and MI risk (<200 mg: aOR=0.63 (0.37 to 1.09); ≥200 mg: aOR=0.74 (0.51 to 1.08)).
Association of allopurinol use and first-ever non-fatal MI
Association of allopurinol use with MI risk by subgroup
Stratified analysis showed that the adjusted ORs were similar for hypertensive and non-hypertensive patients and for both sexes (figure 2). Next, we examined whether the relation between allopurinol use and MI risk was similar by type of MI (STEMI and NSTEMI). Allopurinol use was associated with a significantly decreased risk of STEMI (aOR: 0.65 (0.44 to 0.96)) but not of NSTEMI (aOR: 1.17 (0.69 to 1.98)). Polytomous logistic regression revealed significant aORs after stratification on STEMI/NSTEMI cases (p=0.01).

{kind=link}
{kind=link}
Forest plot of adjusted ORs by type of myocardial infarction (ST-elevated (STEMI) and non-ST-elevated (NSTEMI)), sex and hypertension status (HTA− and HTA+). The number of cases who had STEMI and NSTEMI was n=1710 and n=540, respectively.
Among the 56 MI presented with a resuscitated cardiac arrest (‘near-deaths’), previous allopurinol use was 0% (95% CI (0.0% to 6.2%)), which is not statistically different from that of non-near-death MI patients (3.1%). Previous allopurinol use in the 115 matched controls to near-death patients was 3.8%, which is similar to the proportion of users in the whole control population.⇓
Association of colchicine use and first-ever non-fatal MI
Association of colchicine use and MI
Finally, we investigated the association of colchicine use and risk of MI. Cases and controls had taken colchicine in the same proportion: 1.1% (see online supplementary table S1). Colchicine use in the previous 2 years was not associated with decreased MI risk. When cases were compared with their matched controls, the aOR was 1.17 (0.70 to 1.93).
Discussion
Our study is the first to specifically assess the association of allopurinol use and risk of MI in patients without a history of coronary artery disease or stroke. Our data suggest that use of allopurinol may be associated with an approximately 20% decreased risk of first-ever non-lethal MI. Our study did not confirm that MI risk was reduced in colchicine users.
During the recent years, an increasing number of publications have supported that allopurinol might have a beneficial effect in a variety of cardiovascular diseases, and may provide a survival benefit among patients with hyperuricaemia.22 Indeed, allopurinol, a free radical scavenger, was found to improve both endothelial dysfunction and levels of some markers of oxidative stress.23 It also improved exercise capacity in patients with chronic stable angina,24 and ameliorated the morbidity and mortality of patients with congestive heart failure and a history of gout.25 Indeed, in a large observational study, the use of allopurinol was associated with an approximately 30% reduced risk of readmission after heart failure or death in patients with a history of gout.26 Furthermore, allopurinol decreased blood pressure in adolescents with newly diagnosed hypertension, and lowered plasma renin activity and peripheral resistance.27 The precise mechanism by which allopurinol exerts a beneficial effect on the cardiovascular system is poorly known. The drug is thought to act mainly through an increase in the bioavailability of endothelium-derived nitric oxide, presumably by blocking the production of reactive oxygen species generated by the XO activity.28 We found allopurinol use associated with a decreased risk of STEMI, with no association with NSTEMI. The higher proportion of STEMI is expected in incident MI cases, as opposed to secondary MI, in which NSTEMI are more frequent due to better survival compared with STEMI.19 STEMI is usually associated with total coronary occlusion by thrombus, whereas NSTEMI is more likely associated with incomplete thrombotic occlusion and more extensive atheromatous disease.19 Therefore, allopurinol might modulate the thrombotic phenomenon.
Recent data have also suggested that the cardiovascular benefit of allopurinol in patients with heart failure might be due to its urate-lowering property,26 although this point is a matter of debate. Indeed, posthoc analyses of clinical trials have suggested that the reduced vascular risk afforded by therapeutics, such as atorvastatin and losartan which are not XOIs, was due to their urate-lowering property.29 ,30 However, two randomised trials showed that the uricosuric agents probenecid and benzbromarone had no effect on endothelial function and haemodynamic impairment, respectively, although they significantly decreased urate levels.31 ,32 Thus, the mechanism of improvement with allopurinol may rely more on its ability to reduce oxidative stress rather than on its impact on urate levels.28 Some studies have reported a dose-response effect of allopurinol31 not found in our study. The difference may be due to a lack of power of our work to demonstrate such an association, as very few patients use a high dose of allopurinol (>300 mg). In our study, allopurinol use was reported by about 3–4% of cases and controls, a proportion that is higher than the estimated prevalence of gout in general practice European populations, 0.5–1.5% of adults33 ,34 and in our control group (0.9%). This difference may be explained by an inappropriate prescription of allopurinol for asymptomatic hyperuricaemia in France.35 By contrast, febuxostat prescription was considerably less frequent; it was reported by 0.1% of controls and no cases, which precluded computing the risk of MI associated with its use. This assessment would have been interesting for at least two reasons: to test the hypothesis that the effect of allopurinol we found is due to its ability to inhibit the XO activity and not another property; and to more deeply understand the links between the use of febuxostat and cardiovascular adverse outcomes. Indeed, animal studies found that febuxostat improved ventricular function36 ,37; unexpectedly, a pivotal trial found an early, although non-significant, cardiovascular safety signal38 not found in a large subsequent randomised study.39
We found colchicine not associated with a modified risk of MI. This finding is in contrast with a recent observational study showing a lower prevalence of MI for patients with gout who took colchicine.18 This apparent discordance might be explained, in part, by the difference in sample characteristics, and mostly by the use of International Classification of Diseases code for diagnosis of gout and MI in the previous study,18 which is a known limitation for interpreting results of such observational studies. However, we acknowledge that our findings, due to the low exposure to colchicine, should be cautiously interpreted.
Our study is original in two ways. First, most previous studies have investigated the possible effect of allopurinol in patients with advanced heart disease, but our cases had no history of coronary disease. Second, we used a case-control methodology, which is appropriate for the study of non-frequent events, such as first-ever MI. Moreover, the PGRx methodology minimises sources of bias that can affect case-control studies.19 ,40 The main PGRx features are (1) a systematised collection of cases, performed independently of exposure; (2) a two-step gathering of a pool of referents from which controls are individually selected and matched to cases, so the selection of controls is independent of exposure and (3) the objective documentation of all drugs used through medical prescriptions and patient self-reporting or records. Specific strengths of the present study were its large size, controls matched to cases on classical matching factors (eg, age, sex) and also on hypertension, and major vascular risk factors were taken into account in multivariate analyses. Our study contains some limitations that deserve comments. In comparison between cases and matched controls, the study power was not sufficient for strictly reaching the statistical significance. However, the validity of our findings was supported by several arguments. First, the association between allopurinol use and risk of first-ever MI was statistically significant when using less stringent matching criteria. Moreover, the association was consistent across different strata by hypertension status and sex. However, a weakness of our study is that we could not investigate a link between duration of allopurinol use, as was done in other studies,22 ,26 and MI risk, because most allopurinol users (90%) reported continuous use during the two preceding years. Importantly, we cannot exclude a potential survival bias in our study because fatal MI cases were not included. This implies that our data need to be confirmed by subsequent studies using incident users. Yet, data from 56 MI cases presented with a resuscitated cardiac arrest did not suggest higher exposure to allopurinol among the most severe MI cases. Indeed, among these 56 cases, none had previously used allopurinol, compared to 3.8% of their matched controls. Although these data do not allow excluding a survival bias, they are not in favour of this hypothesis.
Additionally, we were unable to study the impact of allopurinol use in patients with gout because of too few untreated patients with gout among cases and controls. However, this situation is unlikely to be a major issue because we took into account all gout-associated conditions. Additionally, there is in the literature evidence that allopurinol can improve angina pectoris or ventricular dysfunction in patients without gout. Indeed, in randomised, placebo controlled trials, allopurinol given in patients without any history of gout prolonged exercise capability24 and reduced left ventricular mass,41 ,42 respectively.
In conclusion, we found that allopurinol use may be associated with a 20% decreased risk of MI, a finding of relevance, given the high cardiovascular risk in patients with gout. Large randomised trials evaluating the efficacy of XOIs on cardiovascular outcomes in gout are now warranted to carefully evaluate the cardiovascular benefits and risks of such treatments.
Acknowledgments
We thank all the investigators who collected data for this study. We also thank the patients who agreed to be recruited in this case-control study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
-
Collaborators The PGRx-MI study group: Philippe Fromage, MD, CHI d’Annemasse, Alain Furber, MD, PhD, CHU d'Angers, Denis Mery, MD, Hôpital Joseph Imbert, Adnan El Jabali, MD, Centre Hospitalier Louis Pasteur, Jean-Luc Banos, MD, Clinique Lafourcade, Philippe Tarabbia, MD, Clinique Paulmy, Shahin Sedighian, MD, Centre Hospitalier de Béziers, Robert Lallemant, MD, Centre Hospitalier du Duchenne, Attia Kadri, MD, Centre Hospitalier Pierre Oudot, Michel Ovize, MD, PhD, Hôpital Cardio-vasculaire et Pneumologique Louis Pradel, Georges Saint-Mézard, MD, Centre Médical de Cambo les Bains, Philippe Brandstatt, MD, Centre Château Le Moine, Bassel Koujan, MD, Centre Hospitalier Châteauroux, Aimé Amonchot, MD, CHU Gabriel-Montpied, Thomas Gouvion, MD, Groupe Hospitalier du Centre Alsace, Kamel Ouanes, MD, Centre Hospitalier de Crest, Yves Cottin, MD, PhD, Hôpital du Bocage, Hocine Zaouali, MD, Centre Hospitalier de la Dracénie, Véronique Dormagen, MD, Hôpital Simone Veil, Zahi Afif, MD, Centre Hospitalier de Firminy, Jean Philippe Godenir, MD, Hôpital Marie Madeleine, Jean Philippe Alary, MD, CHI Fréjus Saint-Raphaël, Bruno Pierrard, MD, Centre Hospitalier de Villefranche sur Saône, Manuel Imianitoff, MD, Centre Hospitalier de Grasse, Gérard Bessede, MD, Centre Hospitalier de Guéret, Bruno Vaquette, MD, Centre Hospitalier Saint-Louis, Michel Martelet MD, Centre Hospitalier de Langres, Joseph Mouallem, MD, Centre Hospitalier de Langres, Raif Sader, MD, Centre Hospitalier de Laon, Hervé Gorka, MD, Centre Hospitalier Louis Pasteur, Philippe Rosak, MD, Centre Hospitalier du Mans, Michel Viallet, MD, Centre Hospitalier Emile Roux, Jazila Mokaddem, MD, Centre Hospitalier du Nord Mayenne, Gérard Brefort, MD, CHI du Sud Aveyron de Millau, Noureddine Dahmani, MD, Clinique Kennedy, Olivier Nallet, MD, CHI Le Raincy-Montfermeil, Philippe Guillot, MD, Clinique du Millénaire, Florence Leclercq, MD, PhD, Hôpital Arnaud de Villeneuve, Yann Jamon, MD, Nîmes, Emmanuel Tcheng, MD, Centre Hospitalier Louis Giorgi, Olivier Dibon, MD, Hôpital La Source, Aurès Chaib, MD, Hôpital Européen Georges Pompidou, Olivier Lozinguez, MD, Clinique Bizet, Gabriel Steg, MD, PhD, Hôpital Bichat, Nicolas Delarche, MD, Centre Hospitalier François Mitterrand, Christian Boureux, MD, Hôpital Saint-Jean, Erick Merle, MD, Centre de Réadaptation et de Convalescence Cardiocéan, Fatima Boukhsibi, MD, Hôpital Départemental Stell, Charlotte Mestrallet Rivet, MD, Centre Hospitalier de Rumilly, Patrick Broin, MD, CHI de Sallanches, Luc Boulain, MD, Centre Hospitalier de Salon de Provence, Bertrand Ferron, MD, Centre Hospitalier Gaston Ramon, Elian Hajmoussa, MD, Centre Hospitalier de Saint-Amand, Felix Pradies, MD, Clinique La Pinède, Sylvain Destrac, MD, CHI du Val d'Ariège, Nathalie Prouteau, MD, CHI du Val d'Ariège, Daniel Heiligenstein, MD, Hôpitaux du Léman, Michel Galinier, MD, PhD, CHU Toulouse Hôpital Rangueil, Jonathan Banayan, MD, Hôpital Trousseau, Chandrah Goburdhun, MD, Centre Hospitalier de Tulle, Augusta Dobocan Craciun, MD, Centre Hospitalier de Valence, Michel Zylberberg, MD, Centre Hospitalier La Chartreuse, Pierre Guéranger, MD, Centre Hospitalier La Chartreuse.
-
Contributors PR and LGB designed the study and wrote the manuscript LGP, AA, EA participated in the study design and statistical analysis ND, MR, LA have set up the PGRxMI group. AA contributed to manuscript writing and review.
-
Funding This work was funded by the ‘Association Rhumatisme et Travail’ (Rheumatology Department, Lariboisière Hospital, Paris, France).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.