Article Text

Abstract
Background MRI is increasingly used to measure inflammation in rheumatoid arthritis (RA) research, but the correlation to clinical assessment is unexplored. This study determined the association and concordance between inflammation of small joints measured with MRI and physical examination.
Methods 179 patients with early arthritis underwent a 68 tender joint count and 66 swollen joint count and 1.5T MRI of MCP (2–5), wrist and MTP (1–5) joints at the most painful side. Two readers scored synovitis and bone marrow oedema (BME) according to the OMERACT RA MRI scoring method and assessed tenosynovitis. The MRI data were first analysed continuously and then dichotomised to analyse the concordance with inflammation at joint examination.
Results 1790 joints of 179 patients were studied. Synovitis and tenosynovitis on MRI were independently associated with clinical swelling, in contrast to BME. In 86% of the swollen MCP joints and in 92% of the swollen wrist joints any inflammation on MRI was present. In 27% of the non-swollen MCP joints and in 66% of the non-swollen wrist joints any MRI inflammation was present. Vice versa, of all MCP, wrist and MTP joints with inflammation on MRI 64%, 61% and 77%, respectively, were not swollen. BME, also in case of severe lesions, occurred frequently in clinically non-swollen joints. Similar results were observed for joint tenderness.
Conclusions Inflammation on MRI is not only present in clinically swollen but also in non-swollen joints. In particular BME occurred in clinically non-inflamed joints. The relevance of subclinical inflammation for the disease course is a subject for further studies.
- Arthritis
- Inflammation
- Magnetic Resonance Imaging
- Rheumatoid Arthritis
- Synovitis
Statistics from Altmetric.com
Introduction
In recent years MRI is increasingly being used to measure disease states and treatment response in rheumatoid arthritis (RA) research.1 The development of dedicated extremity-MRI and validated scoring methodology OMERACT RA MRI scoring (RAMRIS) has boosted the use of MRI. MRI has important advantages over conventional radiographs as, in addition to structural damage, inflammation of the synovium of the joints, tendons and bone (bone marrow oedema, BME) can be visualised and quantified.2 ,3 BME is not detected by ultrasound or radiographs and is a strong predictor of erosive progression.4–13 Recent data suggest that the presence of tenosynovitis in early arthritis is associated with progression to RA,14 though more studies on this matter are required. Moreover, the exact role of MRI for diagnosing or prognostication of patients with early arthritis in clinical practice is not yet established.15
Independent of the purpose of MRI use, it is fundamental to understand to what extent abnormalities on MRI are concordant with abnormalities at physical examination of joints. A recent study found a moderate correlation between disease activity score in 28 joints and inflammation scores on MRI,16 but the association between MRI and joint examination has never been studied thoroughly on joint level in patients with early arthritis. Given the general conception that MRI is more sensitive than physical examination; we assumed that inflammation detected at physical examination can be seen on MRI and that MRI may be able to detect more inflammatory lesions than physical examination. We aimed to address the following items: (1) To what extent joint swelling (or tenderness) at physical examination is associated with inflammation on MRI. (2) In what proportion of swollen (or tender) joints is inflammation present on MRI. (3) In what proportion of non-swollen (or non-tender) joints is inflammation present on MRI. (4) Finally, we evaluated all joints that showed inflammation on MRI and determined how many of these joints are clinically not swollen (or non-tender). This last objective addressed the frequency of MRI inflammation that is undetected by clinical examination and therefore reflects subclinical inflammation.
Patients and methods
Patients
One hundred and seventy-nine patients with early arthritis were included in the Leiden Early Arthritis Clinic between August 2010 and February 2012 and underwent MRI at baseline. The Early Arthritis Clinic is a population-based inception cohort that includes patients with confirmed arthritis and symptoms for <2 years. At baseline, patients and rheumatologists completed questionnaires, a 68 tender joint count and 66 swollen joint count was performed by trained research nurses and serum was obtained.17 Written informed consent was obtained from all participants. The study was approved by the local medical ethics committee.
MRI scanning and scoring
The metacarpophalangeal (MCP) joints (second to fifth joints), wrist and (metatarsophalangeal) joints (first to fifth joints) at the most painful (or dominant side in case of equally severe symptoms at both sides) were scanned with an ONI-MSK-extreme 1.5T extremity-MRI-scanner (GE, Wisconsin, USA). For the MCP joints and wrists the following sequences were acquired: coronal T1 spin echo (SE) and T2 SE fatsat, and axial T1 SE fatsat postgadolinium. For the MTP joints axial T1 SE and T2 SE fatsat sequences were obtained. Because of time limitations (the current protocol takes 75 min), postgadolinium sequences were not obtained for the MTP joints. See the online supplementary methods for a detailed scan protocol. Synovitis and BME were quantitatively scored according to RAMRIS.3 Tenosynovitis in the MCP joints and wrists was assessed as described by Haavardsholm et al.2 The MRIs were scored by two readers independently, blinded to clinical data; the mean scores were studied. The within-reader intraclass correlation coefficients for the total RAMRIS score were 0.98 and 0.83; the between-reader interclass correlation coefficient 0.82.
Analyses
Information on swelling of the MCP joints, wrists and MTP joints at physical examination of the scanned joints on the side that was MR-imaged was extracted from the joint count data. Joint tenderness is frequently considered as reflecting local inflammation and was also studied.
To make the MRI data comparable with the data on physical examination, the following items were summed. To calculate the BME score per MCP or MTP joint the score of the distal and the proximal bone was summed (range 0–6). Scoring the wrist according to the RAMRIS method implies that 15 bones are assessed, though not all of these are located around the radioulnar carpal joint that is assessed with physical examination. For the wrist we therefore evaluated the highest score of the bones lining the joint space: distally the proximal carpal row: scaphoid, lunate, triquetrum and pisiform and proximally the radius or ulna. These distal and proximal scores were summed (range 0–6).
The synovitis scores of the MCP and MTP joints were straightforward (range 0–3). The synovitis score of the wrist joint was the highest score of the radioulnar and radiocarpal compartment (range 0–3).
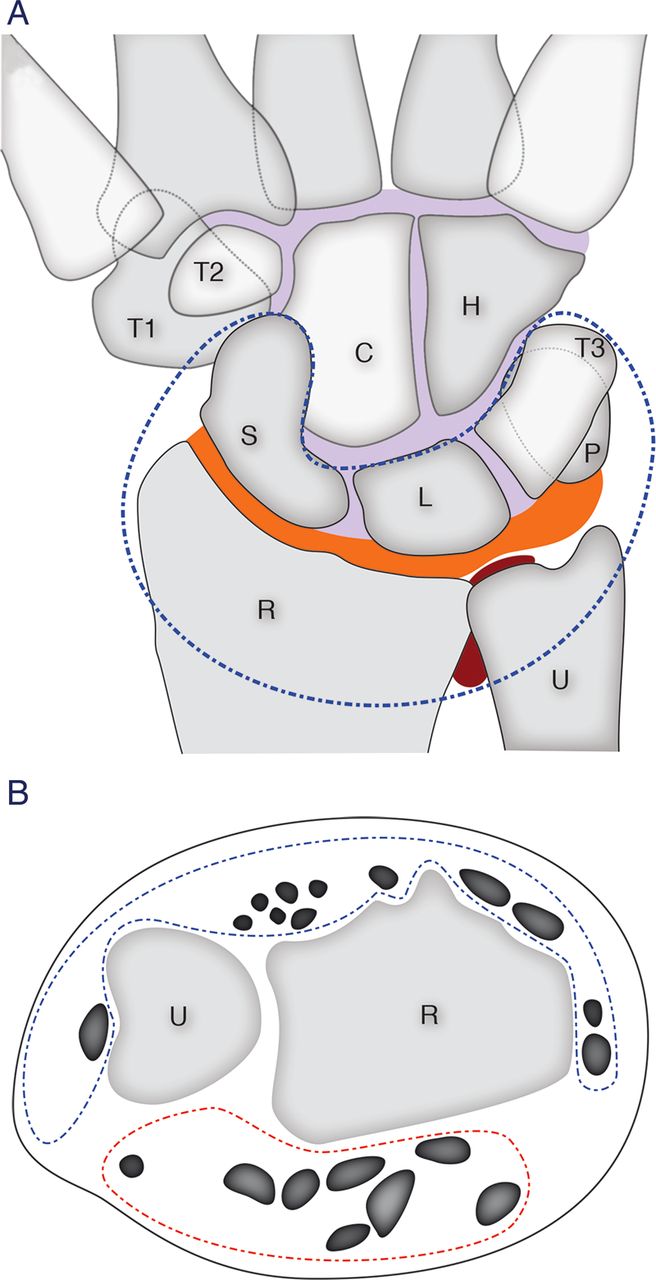
A swollen or tender joint at physical examination can also be (partly) due to tenosynovitis and therefore tenosynovitis was also assessed. To determine the tenosynovitis score per MCP joint we added up the scores of the extensor and the flexor tendons around the MCP joint (range 0–6). For the wrist, the highest score of the tenosynovitis around the extensors and around the flexors were summed (range 0–6). It was not possible to score tenosynovitis of the MTPs, because no coronal sequences, perpendicular to the axis of the metatarsals, were performed. See also figure 1 and online supplementary table S1 for an overview of score calculations.

Overview of bones and joints in the wrist assessed for bone marrow oedema and synovitis (A) and the tendons assessed for tenosynovitis (B). (A) Coronal plane of the wrist, with the 5 metacarpal heads, trapezium (T1), trapezoid (T2), capitate (C), hamate (H), scaphoid (S), lunate (L), triquetrum (T3), pisiform (P), radius (R), ulna (U). The three synovial compartments are depicted in different colours: intercarpal (purple), radiocarpal (orange) and radioulnar (red). To make the MRI score data comparable with the data at physical examination only the scores of the bones and synovial compartments within the dotted line were analysed. The bone marrow oedema score of the wrist was the sum of the distal and the proximal parts. The distal bone marrow oedema score was the highest score among the scores of the scaphoid, lunate, triquetrum and pisiform. The proximal bone marrow oedema score was the highest score between the scores of the radius and the ulna. The synovitis score of the wrist was the highest score between the radiocarpal and the radioulnar compartments. (B) Axial plane of the wrist, with the radius (R) and the ulna (U) and all the tendons. To make one tenosynovitis score in the wrist we summed the flexor and the extensor scores. The flexor score was the highest score among the tendons within the red dotted line. The extensor score was the highest score among the tendons within the blue dotted line.
First the association between inflammation detected by physical examination and MRI was studied per joint type, using logistic regression analyses with the continuous imaging scores as the independent variable and the joint examination results as dependent variable. Then, the association between inflammation detected by physical examination and by MRI was studied in all joints together. This analysis was done using generalised estimated equations as this model takes into account that in every patient 10 joints were assessed. Adjustments for age and gender were included. The exchangeable correlation matrix was used.
Subsequently the continuous MRI data were dichotomised to compare the concordance and discordance with physical examination. First, the cut-off of 1.0 was chosen; this score was achieved if the mean of both readers was ≥1.0. Two-by-two tables were made and proportions calculated. SPSS V.20.0 was used. p Values <0.05 were considered statistically significant.
Results
Clinical baseline characteristics
Baseline characteristics of the 179 patients with early arthritis studied are presented in table 1. As shown in table 2, the percentage of patients with at least one clinically swollen or tender MCP, wrist and MTP joint ranged between 30% and 40%. Among the MCP and MTP joints, the second and the third joints were most frequently swollen and tender. The majority of swollen joints at examination (79%) were also tender. Conversely, 49% of the tender joints were also swollen at physical examination. The relation per joint region is depicted in figure 2.
Characteristics of the 179 patients with early arthritis
Frequency of patients with inflammation in MCP, wrist or MTP joints at physical examination and MRI

Inflammation features at physical examination and on MRI and their occurrences in MCP, wrist and MTP joints.
MRI baseline characteristics
Per patient 10 joints (4 MCPs, 1 wrist and 5 MTPs) were scanned. The frequencies of synovitis, tenosynovitis and BME are presented in table 2. In the wrists these features were more frequently present than in the MCP and MTP joints. Among the MCP joints, the second and the third MCPs were most frequently affected by synovitis, tenosynovitis and BME. In the wrist, the lunate showed most frequently BME (41% had a score ≥1) and among the MTP joints synovitis, tenosynovitis and BME were most often present in MTP1. The MRI features of inflammation frequently occurred together (figure 2).
Association between inflammation detected by MRI and physical examination
First the association between inflammation on MRI and at physical examination was analysed per joint type (eg, all MCP2 joints). The OR on joint swelling for every unit increase in MRI score is depicted in figure 3. All three inflammatory measures visualised on MRI were significantly associated with the presence of joint swelling at physical examination. Among the MCP joints the strongest associations were observed for MCP2 and MCP3 joints and among the MTP joints for MTP3 and MTP4 joints.

{kind=link}
{kind=link}
{kind=link}
The association between inflammation detected by MRI and physical examination, for every MCP and MTP joint separately. *=p<0.05. The association between inflammation detected by physical examination and MRI was studied per joint type, using logistic regression analyses with the continuous imaging scores as independent variable and the joint examination results as dependent variable. The OR reflects the ratio between the odds on joint swelling and the odds on no joint swelling for every unit increase in MRI score per joint type. It was not possible to score tenosynovitis of the MTPs, because here no right-angled (coronal planes) MR-images were available.
Second for all 1790 joints together the association between inflammation detected by MRI and physical examination was analysed. All three inflammatory measures visualised on MRI were significantly associated with the presence of joint swelling at physical examination. Synovitis on MRI was more strongly associated with clinical joint swelling than with tenosynovitis or BME. As the MRI inflammation features often occurred together, all three features were entered in one analysis, to evaluate which of these variables were independently associated with clinical joint swelling. In the MCP joints, synovitis and tenosynovitis were independently associated with clinical swelling (OR 3.3 and 2.4, p<0.001), but BME was not independently associated with joint swelling (OR 1.2, p=0.13). In the wrist, similar results were obtained: synovitis and tenosynovitis were independently associated to clinical swelling (OR 2.3 and 1.8, p=0.03), in contrast to BME (OR 1.0, p=0.8) (see online supplementary table S2).
Frequency of MRI inflammation in clinically swollen joints
Subsequently the continuous MRI scoring data were dichotomised and the concordance and discordance between inflammation detected by physical examination and MRI studied (table 3). Of all swollen MCP joints at physical examination, any MRI measure of inflammation was present in 86%, synovitis in 73%, tenosynovitis in 65% and BME in 50%. Of all swollen wrists, any MRI measure of inflammation was present in 92%, synovitis in 83%, tenosynovitis in 78% and BME in 75%. Of all swollen MTP joints, synovitis was seen in 21%, BME in 23% and any of these features in 29%.
Inflammation on MRI in relation to joint swelling at physical examination
Frequency of MRI inflammation in clinically non-swollen joints
Of all non-swollen MCP joints at physical examination, any MRI measure of inflammation was observed in 27%, synovitis in 18%, tenosynovitis in 13% and BME in 10%. Of all non-swollen wrists, any MRI measure of inflammation was observed in 66%, synovitis in 50%, tenosynovitis in 41% and BME in 51%. Of all non-swollen MTP joints, any MRI measure of inflammation was observed in 13%, synovitis in 5% and BME in 11% (table 3).
Frequency of clinically non-swollen joints in the presence of inflammation on MRI
Subsequently, it was studied how often physical joint examination was normal, given the presence of inflammation on MRI, indicating what proportion of MRI abnormalities is clinically not detected.
First all MCP joints that revealed any inflammation on MRI were evaluated. Of these, 64% were not swollen at physical examination. Then the MRI inflammatory features were studied separately. Of all MCP joints that had synovitis, 57% were not swollen. Of all MCP joints with tenosynovitis, 54% were not swollen. Of all MCP joints with BME this was 53%. Thereafter, these frequencies were determined for more severe inflammatory features on MRI (cut-off scores ≥2 and ≥3). The frequencies of MCP joints with synovitis, tenosynovitis or BME on MRI that were clinically not swollen, decreased (table 3).
Next, the wrists that showed inflammation on MRI were evaluated in the same way. Of these joints with any inflammation on MRI, 61% were not swollen at physical examination. Of all wrists that had synovitis, tenosynovitis or BME, 58%, 54% and 60%, respectively, were not swollen. When using higher cut-offs to define MRI inflammation (scores ≥2 and ≥3), the part of subclinical synovitis (synovitis at MRI but not at physical examination) of all detected synovitis decreased. However, in the wrists with tenosynovitis score ≥3 and BME score ≥3, 33% and 35% were still clinically not swollen.
When evaluating the MTP joints that showed any inflammation on MRI, 77% were not swollen at physical examination. With regards to synovitis, the majority of MTP joints had a score of ≥1; 67% of these joints were not swollen at physical examination. For BME, 78% of the MTP joints that had BME (score ≥1), were not swollen, indicating the presence of subclinical inflammation. Also when assessing the MTP joints with high BME scores (score ≥3), 58% were clinically not swollen. Hence, the proportion of subclinical BME of all detected BME, was the highest in the feet (table 3).
Analysis on MRI inflammation in relation to joint tenderness at physical examination
Since joint tenderness at physical examination can be considered as a sign of inflammation, all analyses mentioned above were repeated with joint tenderness instead of joint swelling. The association between inflammation on MRI and joint tenderness was less strong (lower OR) than the association between joint swelling (see online supplementary table S2). The concordance between inflammation on MRI and joint tenderness was almost similar (table 4), but the frequency of MRI inflammation in tender MCP joints was less than in swollen MCP joints. Also here, when evaluating all joints with any inflammation on MRI, a large proportion was not tender at examination (56% for MCP joints, 51% for wrists and 59% for MTP joints). Additionally, it was observed that of the joints with relative severe BME (score ≥3), 31–45% were still not tender (table 4) and 19–45% were neither swollen nor tender. Also here these frequencies were the highest in the feet.
Inflammation on MRI in relation to tenderness at physical examination
Subanalyses in early RA
Subsequently we questioned whether the results were different when evaluating only the subgroup of patients with early arthritis diagnosed with RA (2010 criteria; n=66) at first visit. Here the prevalence of all MRI inflammation features was higher than in the total group of patients with early arthritis. The concordance analyses were repeated; overall this did not yield different conclusions (see online supplementary table S3 A,B).
Serological markers and subclinical inflammation
Additionally, the prevalence of subclinical inflammation in patients positive and patients negative for serological markers was evaluated. We observed that BME (score ≥1) was more prevalent in non-swollen joints of anticitrullinated peptide antibody (ACPA) positive patients than in that of ACPA negative patients (p=0.01). Synovitis and tenosynovitis were not significantly different (p=0.65 and p=0.56, respectively). Similar findings were found for rheumatoid factor (RF) RF positive and negative patients (p=0.047, 0.82, 0.17; for BME, synovitis and tenosynovitis). When comparing MRI inflammation in non-swollen joints of patients with and without a raised C reactive protein (CRP), no different prevalence was observed (p=0.82, 0.46 and 0.19, respectively).
Discussion
This study investigated whether joint swelling, which is conceived as a reflection of local inflammation at physical examination, is associated with inflammation reflected by MRI. This study of patients with early arthritis showed that inflammation on MRI is present in the large majority of clinically swollen joints and in non-swollen joints. Furthermore, a high proportion of joints with MRI inflammation had no signs of clinical inflammation. For instance; 35–58% of the joints with severe BME, a MRI feature that was associated with erosive progression in other studies, were non-swollen at physical examination.
All three features of inflammation depicted by MRI (synovitis, tenosynovitis and BME) were significantly associated with the presence of clinical joint swelling. As expected, synovitis had the strongest association. Furthermore, the MRI features of inflammation frequently occurred together in the same joint and the association between BME and clinical swelling was not independent of synovitis and tenosynovitis.
The highest frequencies of MRI inflammation scores were seen in the wrists. More bones, synovium compartments and tendons were assessed in wrists than in MCP and MTP joints. With regards to BME in the wrist, we decided not to evaluate all carpal bones included in the RAMRIS but only the bones that are located around the joint space. This was done to have the same anatomical area investigated by physical examination and MRI. Nonetheless, the percentage of joints, swollen and non-swollen, with inflammatory features on MRI was higher in wrists than in MCP and MTP joints.
Limitations of the present study are the absence of coronal sequences, perpendicular to the axis of the metatarsals, making it impossible to evaluate tenosynovitis of the forefoot. The absence of postcontrast images of the foot resulted in less reliable scoring of synovitis, because hyperplasic inflamed synovium could not be adequately differentiated from fluid in the MTP joints. The absence of postcontrast images may hypothetically have resulted in either overestimation or underestimation of MRI synovitis and therefore the present data do not allow drawing definitive conclusions on the association between synovitis detected by MRI and physical examination of the foot.
For BME evaluation however, contrast enhancement is not required. Interestingly, of all joints with BME score ≥1, the majority was not clinically inflamed and this proportion was the highest in the feet. This indicates that with respect to BME, subclinical inflammation is most often present in the feet. The fact that MTP joints are more difficult to physically examine than other small joints may play a role here.
Hence, we observed that BME is not independently associated with joint swelling and that joints with BME are frequently not swollen (in case of joints with a BME score ≥1 this concerned 53–78% and in joints with a BME score ≥3 this was 35–58%). BME is previously observed to be a prognosticator for erosive joint damage progression in RA.6–8 ,10 ,18 In patients with unclassified arthritis, BME was predictive for progression to RA.19 BME is also called osteitis, as studies that combined MRI and histology observed inflammatory infiltrates at the location of BME. In these samples; osteoclasts were observed nearby, suggesting a link between inflammation and erosive bone damage.20 A previous study showed that clinically relevant progression of joint damage does occur in patients with RA in prolonged remission.21 We showed that BME is also present in the non-swollen joints and by knowing that BME is predictive for erosive progression, BME could reflect subclinical inflammation predicting progression during periods of low disease activity. Unfortunately, in this study we had no longitudinal data and therefore we could not draw conclusions about the follow-up of the non-swollen joints with BME.
Because a joint can be clinically swollen due to inflammation of the synovium of the joints and the tendons, tenosynovitis was scored in addition to synovitis. Both features indeed presented frequently in the same joint. When tenosynovitis was present, synovitis occurred in 78–88%. As far as we know this finding is not reported in previous studies and more research on the value of tenosynovitis as part of joint inflammation in early arthritis is needed.
The evaluation of synovitis and tenosynovitis of the MCP joints and wrists was not hampered by technical issues and we observed that synovitis and tenosynovitis occurred in clinically non-swollen joints. The frequency of this subclinical inflammation depended on the degree of MRI inflammation. For instance, when MRI-synovitis was present with a score ≥1, 57–58% of the joints were not swollen and in case of joints with a MRI synovitis score ≥2 this was 32–33%. One explanation of this finding is that MRI is more sensitive for identifying synovitis than physical joint examination. Alternatively, there are many false-positive findings if we rely on minimal findings.
Joint swelling was studied as the main parameter for clinical joint inflammation. Joint tenderness was assessed as well. The association of inflammation on MRI with swollen joints was stronger than with tender joints. This can possibly be explained by the tender joint count being more frequently affected by processes other than inflammation.
In conclusion, this study observed a high frequency of subclinical inflammation in patients with early arthritis, detected by MRI. The relevance of subclinical inflammation for the disease course is a subject for further studies, though previous studies have indicated that BME is particularly associated with disease progression.
Acknowledgments
The authors express their gratitude to Dr Espen A Haavardsholm and Dr Pernille Bøyesen from Diakonhjemmet Hospital in Oslo, Norway for their training in the OMERACT RAMRIS score. The authors thank G Kracht for making the illustrations of the wrist.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien
-
Contributors Clinical and MRI data were collected by AHMvdHvM, MR, WS and AK. Analyses were performed by AK. The manuscript was written by AHMvdHvM and AK. Critical and valuable comments on the article were made by WS, TWJH, DvdH, JLB and MR.
-
Funding This work is supported by a Vidi grant of the Dutch organisation of Health Research and Development. The research has been funded by The European Community Seventh Framework Program FP7 Health-F2-2008-223404 (Masterswitch) and by a core grant of the Dutch Arthritis Foundation. The work of AK is supported by a grant of the Dutch Arthritis Foundation. The work of WS and MR is supported by the CTMM, the Center for Translational Molecular Medicine (http://www.ctmm.nl), and the Dutch Arthritis Foundation, project TRACER (grant 04I-202).
-
Competing interests None.
-
Ethics approval The study was approved by the local medical ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.