Article Text

Abstract
Objective: To analyse the durability of the responses after haematopoietic stem cell transplantation (HSCT) for severe systemic sclerosis (SSc) and determine whether the high transplant related mortality (TRM) improved with experience. This EBMT/EULAR report describes the longer outcome of patients originally described in addition to newly recruited cases.
Methods: Only patients with SSc, treated by HSCT in European phase I–II studies from 1996 up to 2002, with more than 6 months of follow up were included. Transplant regimens were according to the international consensus statements. Repeated evaluations analysed complete, partial, or non-response and the probability of disease progression and survival after HSCT (Kaplan-Meier).
Results: Given as median (range). Among 57 patients aged 40 (9.1–68.7) years the skin scores improved at 6 (n = 37 patients), 12 (n = 30), 24 (n = 19), and 36 (n = 10) months after HSCT (p<0.005). After 22.9 (4.5–81.1) months, partial (n = 32) or complete response (n = 14) was seen in 92% and non-response in 8% (n = 4) of 50 observed cases. 35% of the patients with initial partial (n = 13/32) or complete response (n = 3/14) relapsed within 10 (2.2–48.7) months after HSCT. The TRM was 8.7% (n = 5/57). Deaths related to progression accounted for 14% (n = 8/57) of the 23% (n = 13/57) total mortality rate. At 5 years, progression probability was 48% (95% CI 28 to 68) and the projected survival was 72% (95% CI 59 to 75).
Conclusion: This EBMT/EULAR report showed that response in two thirds of the patients after HSCT was durable with an acceptable TRM. Based on these results prospective, randomised trials are proceeding.
- AD, autoimmune disease
- ATG, antithymocyte globulins
- EBMT, European Group for Blood and Marrow Transplantation
- G-CSF, granulocyte-colony stimulating factor
- HSCT, haematopoietic stem cell transplantation
- LVEF, left ventricular ejection fraction
- PAP, pulmonary artery pressure
- PBSC, peripheral blood stem cells
- SSc, systemic sclerosis
- TBI, total body irradiation
- Tlco, carbon monoxide transfer factor
- TLI, total lymphoid irradiation
- TRM, transplant related mortality
- VC, vital capacity
- systemic sclerosis
- autoimmune diseases
- autologous bone marrow transplantation
- haematopoietic stem cell transplantation
- Rodnan skin score
Statistics from Altmetric.com
- AD, autoimmune disease
- ATG, antithymocyte globulins
- EBMT, European Group for Blood and Marrow Transplantation
- G-CSF, granulocyte-colony stimulating factor
- HSCT, haematopoietic stem cell transplantation
- LVEF, left ventricular ejection fraction
- PAP, pulmonary artery pressure
- PBSC, peripheral blood stem cells
- SSc, systemic sclerosis
- TBI, total body irradiation
- Tlco, carbon monoxide transfer factor
- TLI, total lymphoid irradiation
- TRM, transplant related mortality
- VC, vital capacity
- systemic sclerosis
- autoimmune diseases
- autologous bone marrow transplantation
- haematopoietic stem cell transplantation
- Rodnan skin score
Systemic sclerosis (SSc) is a heterogeneous autoimmune disease (AD) characterised by predominant T cell activation, production of autoantibodies, and cytokine release. These all contribute to diffuse microvascular injury, fibroblast activation, and increased production of collagen, leading to diffuse sclerosis within the skin and internal organs.1,2 The exact cell lineage(s) responsible for the appearance of SSc remains unknown. However, both experimental3,4 and clinical data5–10 point to abnormal function of T and B cells, endothelial cells, and fibroblasts. When associated with early pulmonary, cardiac, or renal disease—diagnosed within the first 3–5 years after onset of the disease—SSc is responsible for a significantly reduced lifespan due to rapid end stage organ failure.11–13 Several recent studies have now confirmed that rapidly progressive SSc, both in its diffuse and limited cutaneous forms, has a 5 and 10 year survival rate of respectively 20–80% and 15–65% according to the major organ affected at diagnosis.14–16 No treatment has been proved to prevent disease progression, although intravenous monthly cyclophosphamide pulse therapy has been shown to improve skin score and pulmonary function in several phase II open studies.17–23 As a result of these data, several European groups applied myelo- and immunosuppression followed by autologous haematopoietic stem cell transplantation (HSCT) as a potential treatment for severe ADs under the auspices of the European Group for Blood and Marrow Transplantation and the European League Against Rheumatism (EBMT/EULAR).24–26 An international consensus report was published to define the indications and the procedural guidelines,27,28 emphasising the importance of data reporting. The rationale for autologous HSCT transplantation in ADs has been reviewed previously.29–33 Before the treatment of ADs by HSCT, the transplant related mortality (TRM) in the autologous setting had been estimated at <3%.34 The results of several open multicentre phase I–II studies using a restricted number of treatment protocols36–38 have been recently published. These studies demonstrated the feasibility, the toxicity, and the early efficacy of this new treatment. In a previous paper by Binks et al,36 under the auspices of EBMT/EULAR, including several active North American groups, we described the preliminary results observed in the first 41 cases with at least 3 months’ follow up after transplantation. These results were reported to the EBMT/EULAR international data registry in Basel from 1996 to 1999. Striking improvement in the skin score was shown after autologous stem cell transplantation, with a trend towards stabilisation of lung disease. The TRM observed initially was high at 17%, although it fell to 12.5% when a further 24 patients were recruited. This reduced TRM was probably due to more careful patient selection, with better definition of exclusion criteria learnt from early experience.33,36–38
This follow up report from the EBMT/EULAR database describes the longer term outcome of those patients originally described in Binks paper36 with, in addition, newly recruited cases since then from all European phase I–II studies. The specific aims of this study were to evaluate the durability of the early positive responses and the possibility of reducing the TRM with better patient selection.
PATIENTS AND METHODS
We report results from patients with refractory severe SSc and early visceral involvement who were treated by autologous HSCT in several open, multicentre, uncontrolled phase I–II studies throughout Europe with at least 6 months’ follow up after transplantation and who were registered in the EBMT/EULAR International Stem Cell Project database up to August 2002. As previously published,36 participating centres were requested to follow the basic concepts and guidelines of the joint international committee of EULAR and EBMT25,28 for patients selection and protocol design. Patients with SSc, defined according to the American Rheumatism Association criteria,2 were eligible if they fulfilled at least one of the following characteristics: (a) early rapidly progressive diffuse SSc developing over the past 3 years despite continuing treatment and in the absence of end stage organ failure, or (b) limited SSc with life threatening pulmonary fibrosis or pulmonary hypertension. Patients written informed consent was required and each protocol was approved by local ethics committees.
Pretransplant evaluation
Pretransplant evaluation included (a) patient’s disease pattern (diffuse or limited skin sclerosis) and duration of the disease (in months since first diagnosis); (b) organ involvement to assess the severity of the disease according to (i) the extension of skin sclerosis using the Rodnan modified skin score40 with three local scoring system in addition to the Kahaleh score,41 (ii) electrocardiogram, echocardiography to measure left ventricular ejection fraction (LVEF, expressed as a percentage of normal), and mean pulmonary artery pressure (PAP in mm Hg), (iii) chest x ray examination, pulmonary function tests with vital capacity (VC) and carbon monoxide transfer factor (Tlco) expressed as a percentage of the predicted value to evaluate pulmonary function, (iv) creatinine clearance for renal function; (c) presence of anti Scl-70 (antitopoisomerase I) and anticentromere antibodies.
Mobilisation and collection of peripheral blood stem cells (PBSC)
Mobilisation and collection of PBSC was achieved with cyclophosphamide (4 g/m2) in combination with granulocyte-colony stimulating factor (G-CSF), or G-CSF alone according to local protocol or when cardiac function with decreased LVEF prevented the use of cyclophosphamide.
Cell selection
Cell selection before transplantation was performed or not, according to local protocol, using CD34 positive selection with or without additional lymphocyte depletion using monoclonal antibodies, particularly anti-CD52 (CAMPATH 1), anti-CD3, anti-CD19, or anti-CD20.
Conditioning regimen
The conditioning regimen, as previously described,36 used various combinations of cyclophosphamide alone (at 150 or 200 mg/kg total dose) or with the addition of total body irradiation (TBI), total lymphoid irradiation (TLI), antithymocyte globulins (ATG), or CAMPATH 1 to achieve further T cell depletion, or another regimen (BEAM: carmustine, cytarabine, melphalan, and etoposide or fludarabine alone or carmustine (BCNU) alone.
Patient follow up
To assess the durability of the observed responses, repeated evaluation of skin score, pulmonary, cardiac, and renal functions by the local investigators were recorded at 6, 12, 24, and 36 months after transplantation. Results were given as a percentage of baseline values compared with those obtained at the time of the pretransplant evaluation as assessed at inclusion. A decline in skin score was considered significant if it differed by more than 25% from baseline values42 or by more than 10% of the maximum skin score.36 A 15% change in VC or in Tlco was considered to be clinically significant. At each evaluation, the patient outcome was classified by the local investigators according to results of clinical and laboratory examination according to the EBMT definition as follows: complete response if the overall response was above 50%, partial response if the overall response was above 25% and below 50%, stable disease with no response, or progression as compared with inclusion. Relapse was defined by the onset of progression after prior partial or complete response. Disease progression was defined as an increase in skin score above 25% compared with the baseline values, the onset of a decrease in VC or Tlco above 15% compared with baseline, and/or progressive vital organ failure.
The cause of death was classified as disease progression or treatment related. The final TRM and other negative outcomes were calculated for the whole group of patients—that is, some of those previously reported in Binks paper36 and the newly recruited patients since then. Clinical and laboratory data were collected at 6-monthly intervals.
Statistical analysis
Results are described using the median and range of respective values. Outcomes are reported as of August 2002. Values after the transplant were compared with values at inclusion using the Wilcoxon signed rank test with a p value of 0.01 for significance to adjust for multiple comparisons. Probabilities of survival and of disease progression were calculated using the Kaplan-Meier estimator.43 For survival, death after transplantation was considered as an event, and patients were followed up to the last follow up. For the probability of disease progression, clinical evidence of disease progression in any of the organ systems affected was considered as an event, patients dying of treatment related complications were censored at the time of death.
RESULTS
From January 1996 to August 2002, 57 patients with severe SSc (table 1) treated by autologous peripheral (n = 55) stem cell or bone marrow (n = 2) transplantation with at least 6 months’ follow up were reported by 22 European centres from nine countries to the EBMT/EULAR Registry. This new cohort included 32 patients previously analysed with a shorter follow up in Binks’ paper36 and 25 patients enrolled thereafter between August 1999 and August 2002. The geographical distribution of the patients was as follows: France (n = 14), Germany (n = 13), Netherlands (n = 8), United Kingdom (n = 7), Italy (n = 7), Spain (n = 4), Switzerland (n = 2), Finland (n = 1), Belgium (n = 1). Their median age was 40 (9.1–68.7) years with a female predominance (10 male, 47 female). Fifty patients had diffuse SSc and among them 62% of the patients (n = 26/42) had a skin score >50% of maximum, 57% (n = 25/44) a VC <70%, 62% (n = 28/45) a Tlco <70% of body mass related mean, and 61% (n = 28/46) had anti-Scl-70 antibodies. Four patients had limited disease, one was associated with a CREST syndrome—with anti-Scl-70 antibodies present in two of the four patients and anticentromere antibodies in one of two patients. Table 2 shows the disease characteristics and the severity criteria according to organ involvement, as described by the contributing doctor at inclusion. In the whole cohort, 82% (n = 40/49) of the patients had pulmonary disease with either a forced VC <70% and/or a Tlco <70% of reference values, 31% (n = 10/32) had a PAP >30 mm Hg, and 19% (n = 4/21) had these three severity criteria at inclusion. Symptoms of Raynaud’s phenomenon were present in 83% (n = 45/54) of the patients and the LVEF was <45% at inclusion in one of the 42 patients for whom these data were available. None of the 19 patients with available data had a creatinine clearance below 70 ml/min.
Baseline demographic data and duration of follow up in all the patients with severe systemic sclerosis (SSc) treated by autologous peripheral blood stem cell (PBSC) or bone marrow (n = 2) transplantation with at least 6 months’ follow up and reported by centres from nine European countries to the EBMT/EULAR registry between August 1996 and August 2002
Disease characteristics and severity criteria of the patients at the time of inclusion
Table 3 shows the regimen used for priming, PBSC selection before reinjection, and conditioning. Mobilisation of stem cells was successful in all but one of the 56 patients who underwent this procedure. This patient subsequently received bone marrow transplantation using ATG in addition to cyclophosphamide at the time of conditioning to achieve further T cell depletion. The other bone marrow transplant recipient received standard conditioning with cyclophosphamide alone. Cell selection was performed in 87% (n = 48/55) of the cases, mostly using CD34+ selection alone (n = 38/55) or with the addition of another monoclonal antibody (n = 9/55) (table 3). Engraftment was successful in all cases.
Treatment regimen employed
Toxicity
After a median follow up of 20 (range 0.6–81.1) months, 45 out of the 57 patients with severe SSc who had been enrolled in various phase I–II studies throughout Europe were alive with a projected 5 year survival of 72% (95% CI 59 to 75) (fig 4). In the whole cohort, the TRM was 8.7% (n = 5/57) and deaths related to disease progression accounted for 14% (n = 8/57) of the 23% (n = 13/57) total mortality rate observed in the cohort at the time of census. Among the 25 patients enrolled since the first report, two deaths were reported as “procedure related”, one in a patient with an LVEF below 40% and the other with a PAP of 33 mm Hg at inclusion (table 4).
Details relevant to the deaths of all patients registered with EBMT for autologous HSCT in SSc

Evaluation of skin score in patients with severe systemic sclerosis before inclusion (n = 47) and then at 6 (n = 37), 12 (n = 30), 24 (n = 19), and 36 (n = 10) months after HSCT. The proportional change from baseline measurement was calculated for each patient at each available point using the Wilcoxon signed rank test, (p<0.001).

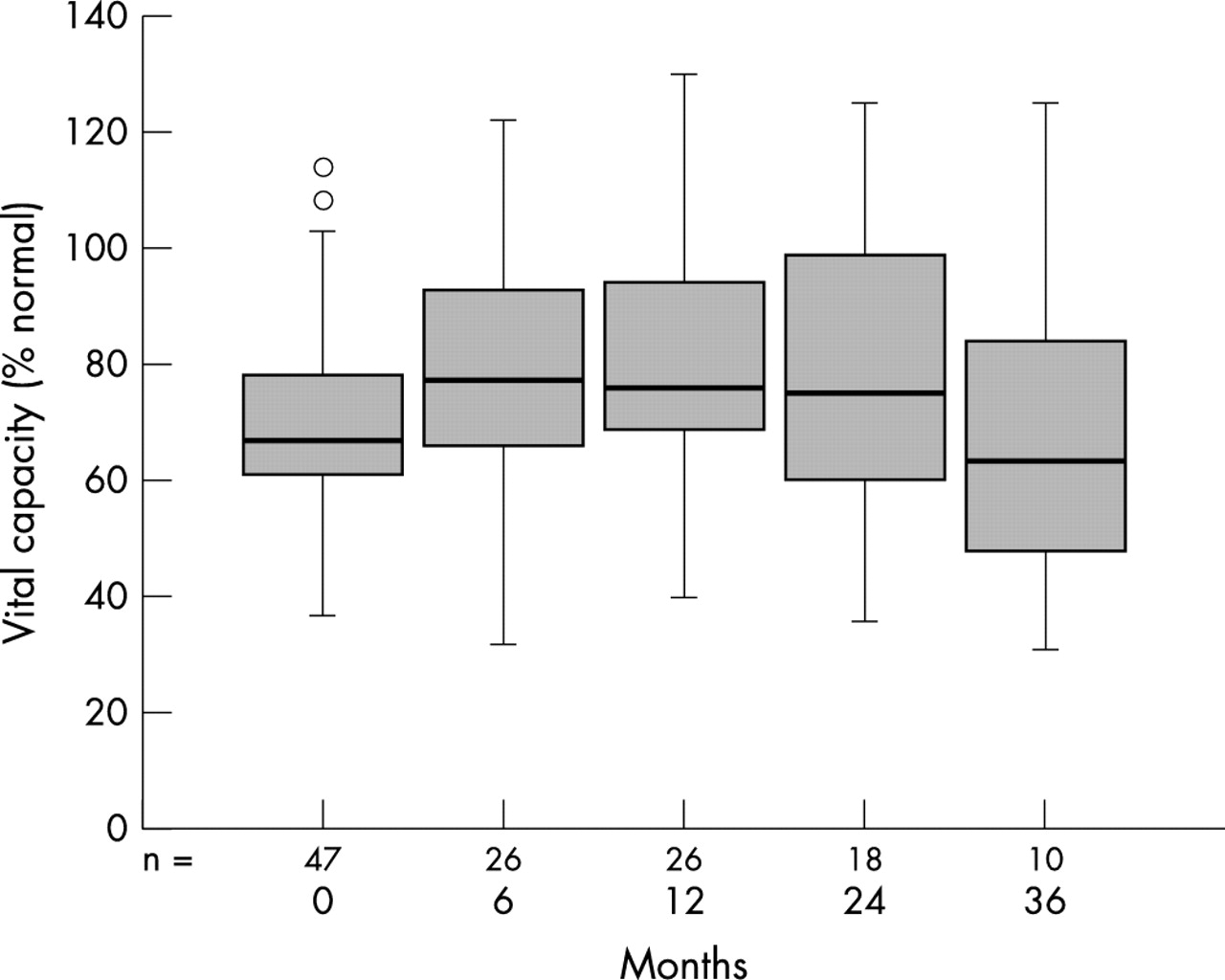
Evaluation of vital capacity (VC) in patients with severe systemic sclerosis before inclusion (n = 47) and then at 6 (n = 26), 12 (n = 27), 24 (n = 18), and 36 (n = 10) months after HSCT. There was no significant deterioration for each patient when calculated at the available point compared with the baseline measurement using the Wilcoxon signed rank test (NS).

Evaluation of Tlco in patients with severe SSc before inclusion (n = 47) and then at 6 (n = 25), 12 (n = 26), 24 (n = 18), and 36 (n = 10) months after HSCT. The proportional change from baseline measurement was calculated for each patient at each available point using the Wilcoxon signed rank test (NS).

Cumulative probability of survival was 72+13% at 5 years according to Kaplan-Meier plot calculation.
Skin scores
Skin scores were evaluated in 47 patients at inclusion with serial measurements from 6 to 36 months after HSCT. A significant fall in skin score, as defined in the “Patients and methods” section, was observed up to 24 and 36 months after HSCT, despite a slight increase at 36 compared with 24 months in two patients. Figure 1 illustrates the change in skin score from baseline for each case with at least 6 months’ follow up after HSCT. The median skin scores were significantly lower at 6 (n = 26/37 patients), 12 (n = 20/30 patients), 24 (n = 15/19 patients), and 36 (n = 6/10 patients) months than those measured at inclusion (p<0.005) (fig 1).
Lung function
Measurements of VC and Tlco were obtained at inclusion (n = 47 patients), with serial follow up available for the VC from 6 months (n = 26) up to 12 months (n = 26), 24 months (n = 18), and 36 months (n = 10) and for the Tlco from 6 months (n = 25) up to 12 months (n = 26 patients), 24 months (n = 18 patients), and 36 months (n = 10 patients) after HSCT. Overall, there was no significant change in the VC (fig 2) or in the Tlco (fig 3) throughout this follow up after HSCT.
Cardiac function
The LVEF was measured before transplantation in 42 patients with a median value of 60% (range 30–85%). Two patients in the whole cohort, who had been previously reported in Binks paper,36 would now be considered as having cardiac exclusion criteria. One patient had an LVEF <45% at inclusion. He died 8 days after the intensification procedure from septicaemia plus cardiac failure and death was reported as “procedure related”. The other one, with an initial PAP of 64 mm Hg, died from “disease progression” and pulmonary hypertension at 7 months after HSCT.
Renal function
No significant deterioration in renal function was reported throughout the follow up.
Disease outcome
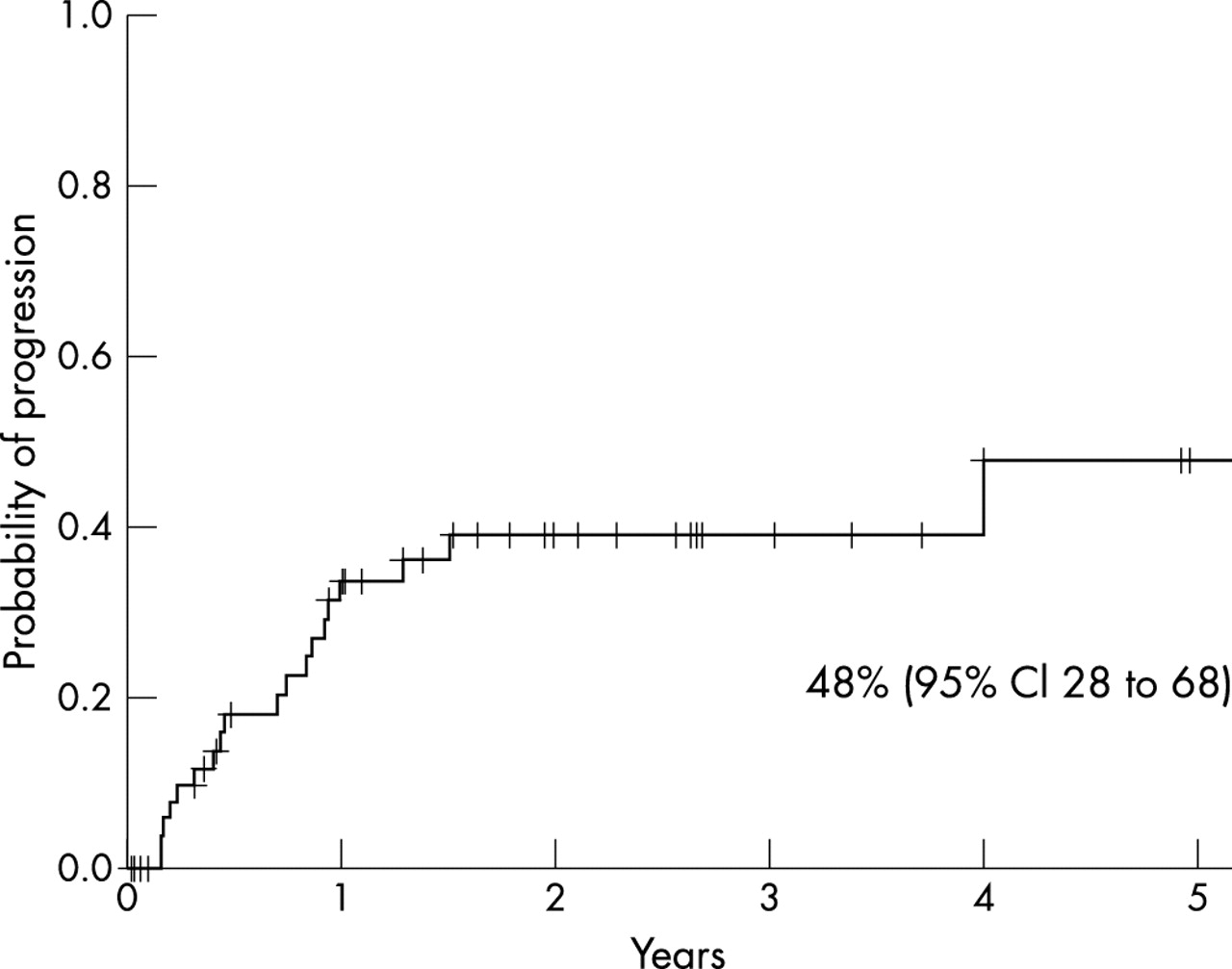
The degree of disease response, as estimated by the local investigator, was reported in 48 patients with at least 6 months’ duration of follow up after PBSC transplantation. Among the two other patients who had received a bone marrow transplant, one patient showed complete remission for 1 year, followed by relapse and death from disease progression at 16.2 months of follow up. The other patient who had received a bone marrow transplant showed partial response until 33 months of follow up. Overall, among the 50 patients with at least 6 months follow up, a partial (n = 32) or a complete response (n = 14) was seen in 92% of the cases and non-response was observed in 8% (n = 4) within 22.9 (range 4.5–81.1) months after autologous HSCT. Longer follow up, showed that 35% of the initial patients with partial (n = 13/32) or complete response (n = 3/14) eventually relapsed within 9 months (range 2.2–48.7) after HSCT. Disease progression, leading to the addition of various immunosuppressive drugs according to local centres, was reported in 38% (n = 19/50) of the patients, of whom 42% (n = 8) subsequently died. The cumulative probability of disease progression at 5 years, calculated according to the Kaplan-Meier method, was 48% (95% CI 28 to 68) (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative probability of disease progression in 57 patients with severe SSc, as reported by local investigators, was estimated at 48+20% at 5 years according to the Kaplan-Meier method calculation. Disease progression was defined by an increase in skin score >25% compared with baseline values, the onset of a decrease in VC or in Tlco >15% compared with baseline, and/or progressive vital organ failure.
Outcome in children
HSCT was performed in five children (four female/one male) under the age of 18 years. Their median age at the time of HSCT was 12 years (range 9–17). All had lung disease at inclusion and SSc (four diffuse and one limited) had been diagnosed within 62 (range 26–85) months before HSCT. They all received the same mobilisation regimen using cyclophosphamide and G-CSF (n = 5) plus cell selection before transplantation with either CD34+ selection alone (n = 3) or CD34+/4+/8+ (n = 2). Different conditioning regimens were used: cyclophosphamide + antiCD52 (CAMPATH 1) (n = 3), cyclophosphamide + TBI + ATG (n = 1), or cyclophosphamide alone (n = 1). After a median duration of follow up of 37.5 (range 13.5–67.6) months, all the five children were alive. Four complete remissions, one partial remission, and one disease progression was observed. One relapse after initial complete remission occurred 9.2 months after transplant.
DISCUSSION
This study demonstrates long term efficacy and improved safety of autologous HSCT in patients with severe SSc. HSCT had a marked and lasting impact on skin involvement, allowing a significant fall in skin score >25% of initial values in 79% of the 19 patients with data available at 2 years after the procedure. To our knowledge, this result has never been previously reported in such severe forms of the disease, with any other treatment. Pulmonary function did not change significantly with prolonged follow up, as initially reported in the short term.36 It is impossible in this setting to speculate on the efficacy or not of HSCT on pulmonary disease, because irreversible pulmonary fibrosis might have been present before the HSCT. Functional improvement with either complete or partial remission, as assessed by the local investigator, was seen in 92% of these patients. However, the onset of relapse in 35% of the initial responders, with a 48% cumulative probability of disease progression at 5 years suggests the possibility that a stronger immunosuppressive regimen at the time of intensification or for maintenance immunosuppression thereafter may be necessary.38 The importance of patient selection was demonstrated by a lower than initially feared TRM rate, because no other change in the selection criteria or in the protocol strategy was performed. Better patient selection, especially in the light of careful cardiac and pulmonary function evaluation, which are often underestimated in patients with severe SSc, has allowed us to decrease the crude TRM, as repeatedly underlined.34–39,44,45 Indeed, the overall mortality from the first 41 patients included in phase I–II studies during the “pioneer period” was 27% and the TRM was 17%.36 At that time, when a larger cohort of 65 patients was considered, with the exclusion criteria according to consensus guidelines,36 the recalculated TRM had fallen to 8%. In the present extended cohort of 57 patients, the TRM was 8.7%, and could be as low as 5.2% if recalculated with consideration of the exclusion criteria before inclusion, a rate comparable to the natural history of this SSc subgroup.11–16 The importance of a learning curve for patient selection and for the overall procedure has been well described in other types of bone marrow43,43 or organ44,47 transplantation. It contributes to the centre effect on a survival curve and may have been enhanced when treating severe SSc, which can often be clinically underestimated.48,49
Patient selection, therapeutic regimen, and graft manipulation were heterogeneous, because data were collected from 22 different European groups with various local practices. Although patients had been included in several small phase I–II trials,33,36 each local protocol was in accordance with the initial consensus guidelines published in 1996 for patient selection and therapeutic regimen.25,28 Therefore the whole cohort constituted a rather homogeneous group of patients, who had undergone autologous HSCT to assess the feasibility of the procedure, its toxicity, and clinical results and who were closely evaluated by each local investigator. All the patients, with either diffuse (n = 50) or limited (n = 4) disease had severe SSc, because the skin score was >50% maximum in 62% of cases, pulmonary involvement with forced VC and/or Tlco <70% was present in 82%, and pulmonary hypertension (PAP >30 mm Hg) in 31%. The therapeutic regimens were similar in most of the cases. For the mobilisation, the use of cyclophosphamide 4 g/m2+ G-CSF (84% of cases) was preferred over G-CSF alone (10.7%). This choice was irrespective of the risk for cyclophosphamide cardiotoxicity, because most of the patients mobilised by G-CSF alone had normal LVEF and a PAP <30 mm Hg at inclusion. Flares of autoimmune disease with the use of G-CSF alone have been reported in rheumatoid arthritis,50,51 multiple sclerosis,52,53 and in a few cases of systemic sclerosis.54,55 The use of cyclophosphamide based PBSC mobilisation protocol has therefore been encouraged, because the addition of a cyclophosphamide to G-CSF enhances the mobilisation efficacy, decreases the risk of flare, and may result in some clinical improvement after mobilisation alone.38,50–58 Cell selection before reinjection was performed in 87% of the cases, using mostly CD34+ selection alone or with another monoclonal antibody. For the conditioning, cyclophosphamide at 150–200 mg/kg total dose over 4 consecutive days (90% of cases) was used most commonly, either alone (n = 35 patients) or in combination with ATG (n = 12 patients). The aim of adding ATG to the conditioning regimen was to achieve further T cell depletion and more intense immunosuppression, but the small number of patients in each group did not allow us to analyse its efficacy in lowering the risk of sustained disease activity or in preventing the onset of relapse after longer follow up.
This extended follow up enabled us to report the durability of the skin response up to 2 and 3 years after HSCT, noticing that at that time several patients had a new increase in skin score with a relapse in some of them. Despite the biases of data registry analysis and the limits of skin scoring,2,41,42,59 such impressive and sustained responses have never been shown by any other therapeutic intervention. The Rodnan modified score40 and the Kahaleh score41 have been validated as the best clinical tools for skin evaluation with tight correlations with survival, and more than 25% fall in the skin score compared with baseline values is clinically significant.42,59 The median disease duration before HSCT was 3 years, which meant that patients were at a later stage of their progressive course, reinforcing the significance of improved skin score.11–16,60,61
In conclusion, this extended report, as part of a European collaborative effort, enabled us to gather all available data from phase I–II European clinical trials reported in the EBMT/EULAR registry. It confirmed that autologous HSCT is feasible, with low mortality in carefully selected patients,3,38 and allows impressive initial clinical responses which had not been previously obtained with any other therapeutic intervention in severe SSc. For the first time, it showed the durability of complete or partial remission observed in two thirds of the patients who had received a transplant up to 3 years after HSCT. The onset of relapse and the presence of sustained disease activity after longer follow up, which had already been reported in SSc38 and in other types of ADs treated by HSCT62 in 20–35% of the cases should not prevent the use of this promising therapeutic option in patients with severe SSc. Although some patients have evidence of disease activity after HSCT, they still do better than before, with a median skin score at 3 years still <25% of baseline values. Further studies will help to elucidate if the use of more intensive immunosuppression at the time of transplant, or maintenance of immunosuppressive drugs thereafter, such as mycophenolate mofetil,63 could lower this risk. The promising experience of these phase I and II studies has been exploited in the design of a phase III, prospective randomised controlled trial, ASTIS (Autologous Stem Cell Transplantation International Scleroderma) Trial (http//www.astistrial.com), which is currently running under the auspices of the EULAR and EBMT.
Acknowledgments
Data reporting was to the EBMT/EULAR registry in Basel. The work was partly supported by the Horten Foundation, the Délégation Régionale à la Recherche Clinique Assistance Publique-Hôpitaux de Paris (PHRC 1997 AOM 97–030). We are also indebted to EBMT corporate members for their contribution.