Article Text

Abstract
Objective: To investigate at 5 years whether an initial 2 year home based strength training period imposes sustained effects on muscle strength, bone mineral density (BMD), structural joint damage, and on disease activity in patients with early rheumatoid arthritis (RA).
Methods: Seventy patients were randomised either to perform home based strength training with loads of 50–70% of repetition maximum (EG) or range of motion exercises (CG). Both groups were encouraged to take part in aerobic activities 2–3 times a week. Maximal muscle strength of different muscle groups was measured by dynamometers, and BMD at the femoral neck and lumbar spine by dual x ray densitometry. Disease activity was assessed by the 28 joint disease activity score, and joint damage by x ray findings.
Results: 62 patients completed 2 years’ training and 59 patients attended check up at 5 years. Mean (SD) maximum muscle strength indices increased from baseline to 2 years—in EG from 212 (78) kg by a mean (95% CI) of 68 (55 to 80) and in CG from 195 (72) kg by 35 (13 to 60) kg—and remained at that level for the next 3 years. Development of BMD in EG tended to be more favourable than that in CG. Muscle strength training was not detrimental to joint structures or disease activity.
Conclusion: The patients’ exercise induced muscle strength gains during a 2 year training period were maintained throughout a subsequent self monitored training period of 3 years. Despite substantial training effects in muscle strength, BMD values remained relatively constant. Radiographic damage remained low even at 5 years.
- BMD, bone mineral density
- CG, control group
- DAS, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- EG, experimental group
- HAQ, Health Assessment Questionnaire
- MTX, methotrexate
- RA, rheumatoid arthritis
- ROM, range of motion
- VAS, visual analogue scale
- rheumatoid arthritis
- muscle strength
- bone mineral density
- radiological damage
- disease activity
Statistics from Altmetric.com
- BMD, bone mineral density
- CG, control group
- DAS, disease activity score
- DMARDs, disease modifying antirheumatic drugs
- EG, experimental group
- HAQ, Health Assessment Questionnaire
- MTX, methotrexate
- RA, rheumatoid arthritis
- ROM, range of motion
- VAS, visual analogue scale
Rheumatoid arthritis (RA) interferes with physiological functions as well as structures of the musculoskeletal system—for example, by reducing muscle mass1 and strength2 and bone mineral density (BMD),3,4 leading to a predisposition to falls and bone fractures. Osteoporosis in patients with RA is reportedly generalised and associated with decreased physical activity,5 impaired function,3,6–8 disease duration,4,8–11 and the inflammatory process itself.4 The concomitant use of corticosteroids further enhances the decrease in BMD.12–16 The vicious circle resulting in loss of muscle strength, functional capacity, and BMD in RA is finally catalysed by the inflammation associated with generalised fatigue, resulting in further limited physical activity. This forces the patients to perform their daily activities and professional duties at a higher percentage of their maximum physiological reserve.17 Conversely, a sedentary lifestyle and poorer physical fitness are associated with increased morbidity and mortality.18,19
The existing evidence for prevention of bone loss by exercise mainly concerns healthy subjects.20 Exercise appears to slow bone loss provided that it is continued for at least 1 year.20 Further, dynamic (aerobic exercise, resistance exercises, and walking) rather than static loading seems to drive skeletal adaptation. A customary loading environment with similar or repetitive loading signals is likely to make bone cells less responsive to activity.21–24 In addition to maintaining or even enhancing BMD, physical exercises impose positive effects on muscle strength, reaction time, and coordination, reducing a person’s risk for falls and bone fractures. Exercise reportedly also reduces pain, stiffness, and joint tenderness in patients with RA16,25,26 and thus improves their functional capacity.27,28 Nevertheless, although perpetual physical activity is of central importance in maintaining or increasing muscle strength in patients with RA, long term studies about the effects of strength training on muscle performance16 and BMD are few.16,29
This randomised study aimed primarily at evaluating whether patients with early RA could maintain the gains in muscle strength obtained during an initial 2 year home based strength training period.16 Further, we focused on changes in the extent of joint damage as well as bone mineral density over the subsequent 3 year period.
SUBJECTS AND METHODS
Subjects
Seventy consecutive patients with recent onset RA according to the American College of Rheumatology 198731 criteria volunteered for the 2 year study. Patients had been referred to the rheumatology unit at Jyväskylä Central Hospital for diagnosis and treatment. Their duration of symptoms was <24 months at inclusion, and the patients had not been treated with prednisolone or disease modifying antirheumatic drugs (DMARDs) before inclusion. Jyväskylä Central Hospital is the only rheumatological centre in the Central Finland district, which has a population of 265 000. All new RA cases are referred to the centre for diagnosis and treatment. The patients were randomly assigned either to the strength training (EG) or to the control group (CG) (table 1). The randomisation was carried out using clusters of four patients stratified according to age and sex (under and over 50 years old, female and male subjects) to ensure that the demographic data of the study groups remained comparable. During the 2 year training period two patients from the EG and three from the CG discontinued the exercises, while three patients were excluded owing to a changed diagnosis. Three years later, at the 5 year check up, 59 of the 62 patients, who completed the training period were re-examined (two patients had moved from the district and one was not interested in participating) (fig 1).
Baseline characteristics of experimental (EG) and control (CG) patients with early RA
Trial profile.
Training programmes
The average stay in the rheumatology unit was 5 days for both groups. During that period, after the baseline measurements, three individual training sessions were conducted under the supervision of an experienced physiotherapist so that the strength training or conventional training programmes could be learnt properly.
Strength training
The strength training programme included exercises for all muscle groups of the arms (biceps curl, lateral pull down, forward single up-rise), legs (knee extension and flexion, hip extension and abduction, squat), and trunk (abdominal crunch and leg lifts while lying on the back, back hyperextension in prone position) using body weight, rubber bands, and dumb-bells as resistance. The training session was about 45 minutes. Subjects were instructed to exercise twice a week with moderate loads (50–70% of the repetition maximum), two sets for each exercise, and 8–12 repetitions for each set. The intensity and technique of exercises were checked at 6, 12, 18, and 24 month follow up visits.
Conventional training
The patients in the CG were instructed to perform range of motion (ROM) and stretching exercises twice a week. Gentle ROM exercises for all joints of upper and lower extremities and neck were instructed to be performed 10 times for each exercise. The stretching exercises included active straight leg raising for hamstring muscles, stretching of quadriceps femoris muscle, calf muscles, pectoralis minor and major muscles, and biceps and triceps muscles. It was recommended that each stretching exercises should be performed with three repetitions for 30 seconds.
After the 2 year measurements the control subjects also were instructed to carry out the strength training programme. However, the instructions for the CG patients were given only once at the outpatient clinic after the 24 month measurements without any check up visits.
In addition, all patients were encouraged to perform aerobic exercises 2–3 times a week.
Assessments
Muscle strength
The maximum unilateral concentric strength of the knee extensors was measured with the David 200 dynamometer (Outokumpu, Finland).32 For this the subject was in a sitting position with the hips fixed on a seat for a flexion position of 110°. The ankle was supported just above the malleoli. The load in the weight stack of the machine was gradually increased until the subject was unable to perform the full knee extension (starting from knee flexion of 110° to the full extension) in order to record a subject’s one repetition maximum (kg). The maximal isometric trunk flexion and extension forces were measured by an isometric strain gauge dynamometer.33 For this the subject was in a standing position. The hips were fixed at the level of the spina iliaca anterior superior. A 5 cm wide strap was tightened around the shoulders at the level of the clavicle in trunk flexion and at the level of the spina scapulae in trunk extension. Isometric grip strength was measured by a Digitest dynamometer (Oulu, Finland).34 In the analysis the best absolute result of each strength measurement (knee extension, trunk extension and flexion as well as grip strength) was combined as a muscle strength index. Both groups were measured at months 0, 6, 12, 18, 24, and at 5 years.
Bone mineral density
BMD (g/cm2) was measured in duplicate at the Rheumatism Foundation Hospital using dual x ray absorptiometry bone densitometry (Lunar DPX, Lunar Radiation Corporation, Madison, WI) at months 0, 12, 24, and at 5 years. The measurement sites were the lumbar vertebrae L2-4 (BMDspine) and the left proximal femur (BMDfem). Quality assurance tests for densitometry were run daily. The precision of the method had previously been tested on adults, and the coefficient of variation (CV%) calculated to be 1.0% for the spine and 1.8% for the femoral neck.
Joint radiology
Radiographs of hands and feet were taken at baseline, and 1, 2, and 5 years thereafter. The radiographs were scored according to the Larsen method.35 The II-V metatarsophalangeal joints, wrists, and metacarpophalangeal joints were assigned a score of 0–5, with a total score of 0–100.36,37 Joints with a score of 2 or higher were considered erosive. All the x ray findings were scored simultaneously after the 5 year follow up by an experienced rheumatologist (TS) who did not know which group the patients were in.
Functional capacity
The Finnish version of the Health Assessment Questionnaire (HAQ), scoring from 0 to 3, was used to measure functional capacity.38
Clinical disease activity
The modified 28 joint disease activity score (DAS), including the number of tender and swollen joints, patient’s self reported global status (on a 0–100 mm visual analogue scale (VAS)), and erythrocyte sedimentation rate, were used to evaluate clinical disease activity.39 Pain, as assessed on a VAS and morning stiffness in minutes were also evaluated.
Physical activity
All subjects completed training diaries and mailed them to investigators every second month during the 2 year follow up. In addition, the type, frequency, and duration of leisure time physical activities during the past 12 months were assessed by a questionnaire at the 5 year check up visit.
Statistical methods
Results were expressed as means with standard deviations (SD) or with 95% confidence interval (95% CI). The normality of variables was evaluated by Shapiro-Wilk statistics. Means between the groups were compared using analysis of covariance with the baseline value, age, sex, disease activity (DAS), and use of prednisolone as covariate. Spearman’s correlation coefficients were calculated to assess the relationships between individual variables.
RESULTS
After initial assessments, treatment with DMARDs (sulfasalazine as the first drug with a few exceptions) was instituted in all patients. However, 24% and 50% of the patients were taking methotrexate (MTX) or a combination of DMARDs including MTX at the 6 month and 2 year visits, respectively, and the majority of the patients (70%) were taking these drugs at the 5 year visit (figs 2A and B). Three patients in both groups used no DMARDs at the 5 year visit owing to remission. Ten patients in the EG and 22 in the CG were treated with low dose prednisolone (2.5–7.5 mg/day) on average (SD) for 8.0 (7.5) months and 30.2 (23.7) months, respectively, during the 5 year follow up period. In those patients the median (interquartile range (IQR)) cumulative doses of prednisolone were 0.76 (0.15–1.42) g and 3.25 (0.80–6.71) g (p = 0.005), respectively. Further, four EG and eight CG patients received drug treatment for osteoporosis (seven patients with alendronate and one patient subsequently with salmon calcitonin, etidronate, and alendronate) for an average (SD) of 45 (1) and 31 (19) months, respectively.

Disease modifying antirheumatic drugs taken by the experimental (A) and 31 control (B) patients with early RA. The percentage of patients taking each drug or combination over 5 years is shown. INFL, infliximab; COMBO+MTX, combination of DMARDs including methotrexate; DMARD, disease modifying antirheumatic drug; MTX, methotrexate; COMBO−MTX, combination of DMARDs without methotrexate; SSZ, sulfasalazine; MYO, intramuscular gold; HCQ, hydroxychloroquine.
The strength training compliance averaged 1.4–1.5 times a week in the EG during the 2 year training period. According to the training diaries the mean (SD) times used for various types of physical exercises (including strength training in the EG) throughout the first 2 years for the EG and CG were 245 (115) and 195 (104) minutes a week, respectively. During the 5th year the corresponding times were 237 (147) and 223 (131) minutes. Reportedly 20 EG and 12 CG patients at least occasionally practised also intensive aerobic exercises (leading to sweating and getting out of breath). Further, 10 EG but no CG cases continued with their strength training during the 5th follow up year.
During the 2 year training period the mean (SD) maximum muscle strength indices in EG and CG increased from 212 (78) kg and from 195 (72) kg by a mean (95% CI) of 68 (55 to 80) kg (32.1%) and 35 (13 to 60) kg (17.9%), respectively (table 2). Further, at the 5 year check up visit the respective muscle strength indices in EG and in CG were 59 (46 to 70) kg (27.8%) and 30 (13 to 46) kg (15.4%) above the baseline values. After adjustment by age, sex, disease activity (DAS), and the use of prednisolone, the differences between the groups were p = 0.050 at 2 years and p = 0.081 at 5 years.
Mean (SD) muscle strength recorded before and after the 2 year strength training period and after the subsequent 3 year follow up in experimental (EG) and control (CG) patients with early RA
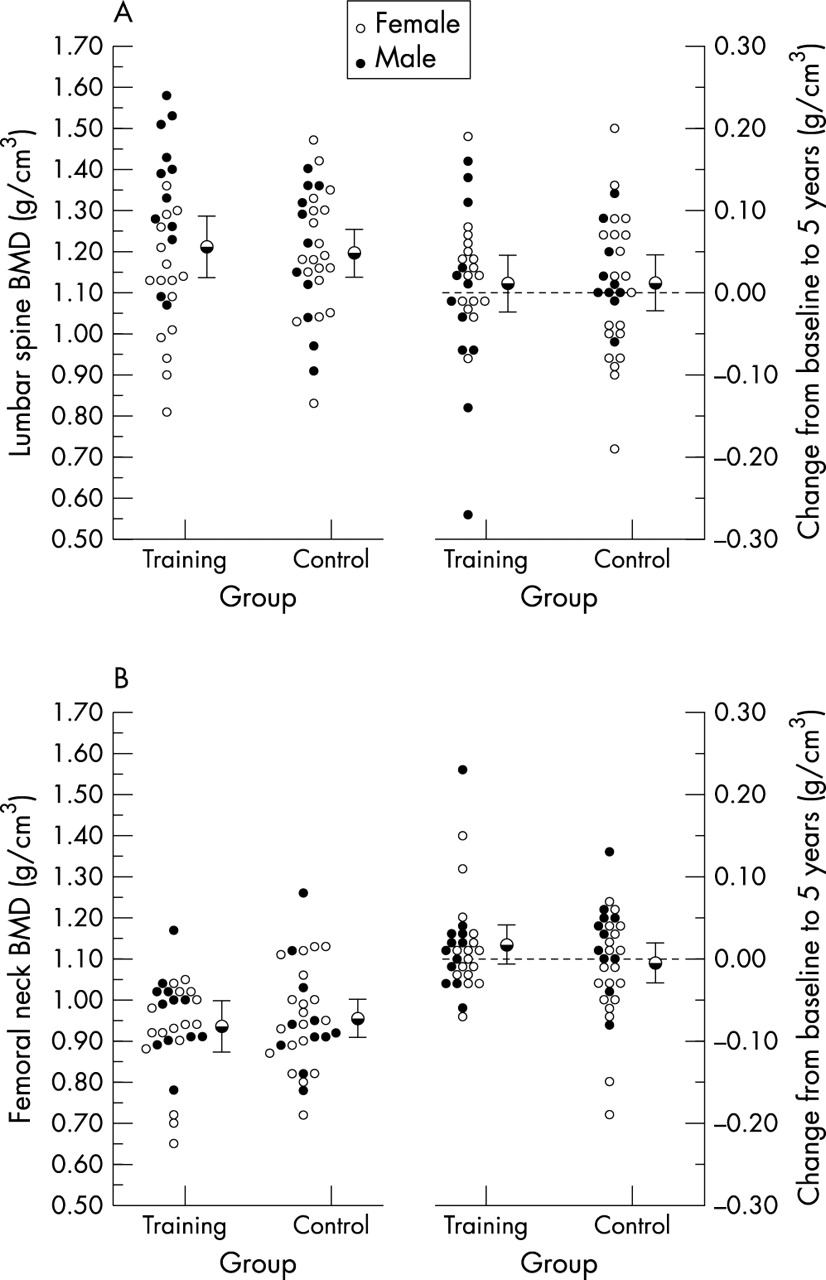
Table 3 presents the absolute BMD values as well as Z scores in both measured sites. No significant intergroup differences in BMD at either of the measured sites were found at baseline (figs 3A and B). The mean BMDfem increased by 0.60% in EG patients, while it decreased by 1.46% in CG during the 2 year strength training period. The corresponding changes in the mean BMDspine were +0.96% and −1.44% in the EG and CG, respectively. After adjustment by age, sex, disease activity (DAS), the use of prednisolone, and drug treatment for osteoporosis, the differences in BMDspine (p = 0.65) and in BMDfem (p = 0.54) between the groups were not significant at the 2 year check up. The respective changes at the 5 year check up from baseline were +1.53% v +1.05% for BMDspine, and +2.12% v −0.45% for BMDfem. After adjustment, the changes in BMDspine (p = 0.21) and in BMDfem (p = 0.68) between the groups did not reach significance. On the other hand, the observed changes of BMDspine (rs = −0.28; p = 0.031) as well as BMDfem (rs = −0.34; p = 0.009) correlated negatively with the cumulative dose of prednisolone in those 32 patients who had been treated with the drug. In EG, the improvements in the age matched Z scores in BMDfem, both from the baseline to 2 years (p = 0.005) and from baseline to 5 years (p = 0.008), were significant.
Bone mineral density of the lumbar spine and femoral neck in experimental (EG) and control (CG) patients with early RA

Bone mineral density of the lumbar spine (A) and femoral neck (B) in the experimental (EG) and control groups (CG) at baseline and after 5 years’ follow up.
The mean (SD) DAS decreased significantly from 4.4 (1.2) to 2.2 (1.2) in the EG and from 4.9 (1.1) to 2.7 (1.2) in the CG during the 2 year training period. The corresponding DAS indices were 2.3 (1.0) and 3.0 (1.2) at the 5 year check up visit. The respective improvements in HAQ during the 2 year training period in the EG and CG were from 0.59 to 0.13 and from 0.77 to 0.35, respectively. At 5 years the HAQ values were 0.30 (0.42) and 0.40 (0.51), respectively. Pain decreased from 42 (19) mm by 67% in the EG and from 41 (27) mm by 39% in the CG and were 22 (20) mm and 26 (24) mm at 5 years. In both groups the improvements both in HAQ (p = 0.023) and in pain (p = 0.033) were in favour of the EG at 2 years. At the 5 year check up visit the significance between the groups had disappeared.
Figure 4 shows the individual values of the Larsen scores at baseline and 5 years. The respective median (IQR) Larsen scores in the EG and CG were 0 (0–1), 0 (0–2), 0 (0–3), and 0 (0–3), 2 (0–5), 2 (0–4) at baseline, and at the 2 and 5 year check ups, respectively. No between-group differences were found (p = 0.268).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual values of the Larsen scores in experimental (EG) and control (CG) groups at baseline and after 5 years’ follow up.
DISCUSSION
This study showed that individually tailored and regularly conducted physical exercises in the early phases of the disease lead to long term increases in muscle strength in patients with RA. The patients can maintain exercise induced muscle strength gains obtained during a 2 year training period throughout a subsequent self monitored training period of 3 years. Despite substantial training effects in muscle strength, the BMD values remained relatively constant. Further, the extent of radiographic damage remained low even at 5 years, showing that patients actively treated with DMARDs can safely carry out the applied, moderate intensity physical activity.
Each activity—including activities of daily living, such as rising from a seated position or climbing stairs—requires a certain amount of strength. Many people with clinically active or with longlasting RA live just above the threshold of the capacity needed for such tasks. The reserve in performance capacity may be so slight, that even a small additional decline in strength may cause serious difficulties in performing some of the daily activities. RA is a chronic inflammatory disease, disturbing the body’s metabolism and composition and favouring the loss of tissue proteins and the accretion of fat.1 Preservation of muscle strength as well as overall physical function are important elements in the prevention of disability in patients with RA. Thus, to prevent the RA induced loss of muscle strength and muscle mass, restoration and improvement of muscle reserves should be started from the very onset of the disease.
In the present study the EG patients could maintain the training induced increases in muscle strength of all measured muscle groups up to 5 years. Significant increases in muscle strength of patients with RA has also been reported.28,40–43 In these studies the patients carried out two to five training sessions a week, but the length of the total training period was rather short, only from 3 to 24 weeks. In our study the frequency of strength training was rather low. According to the patient diaries they trained only 1.4–1.5 times a week during the first 2 years and even less thereafter. However, the loading and duration of training obviously remained sufficient to maintain the muscle strength values at the achieved level. The CG patients were encouraged also to perform ROM, stretching, and aerobic exercises. Thus, the CG patients also were able to improve their muscle strength to some extent, directly owing to a different form of exercise or indirectly owing to decreased pain and disease activity. Regardless of the group to which they had initially been allotted, patients continued to use 4–5 hours a week for physical activities throughout the follow up. Further, 10 patients in the EG continued strength training also after the 2 year intervention, and 20 EG and 12 CG patients reportedly performed aerobic exercises with moderate intensity (sweating and getting out of breath while exercising). Thus both the type and the intensity of training in EG patients explain a substantial part of the difference in the observed muscle strengths in favour of the EG. However, we emphasise that all patients were actively treated with DMARDs and optionally also with prednisolone to keep clinical disease activity low.
Compared with healthy subjects, patients with RA are at increased risk of developing osteoporosis.44,45 In this study most of the patients had BMD values within age matched reference values at baseline. Thus, the realistic target for the physical training was the prevention of disease related bone loss. There were no differences in the changes of absolute BMD between the groups during the 5 year follow up. However, one should note that the EG patients showed statistically significant improvements in age matched Z scores of BMDfem during the 2 year training as well as during the subsequent 3 year follow up period. Previous studies have provided some evidence that prolonged physical exercise delays the decrease of bone loss in healthy postmenopausal women.20 Further, Madsen et al concluded that the effect of exercise on BMD in RA is small, but it may become substantial if accumulated over a number of years.46 In addition to improving muscle strength and maintaining BMD, physical exercise provides other benefits. It improves reaction time, balance, and coordination, and may reduce the risk of falls.47 Thus improvements in neuromuscular function and maintenance or increase in BMD would be the most adequate approach to diminish a person’s risk of bone fractures. High clinical disease activity as well as glucocorticoid treatment have been recognised as the most important contributory factors to the development of osteopenia.4 In the present study, the majority of the patients treated with prednisolone as well as with antiresorptive agents were included in the CG group. The more frequent need for these drugs may reflect higher disease activity, contributing to the observed slight differences in the BMD values. On the other hand, the favourable effects of glucocorticoids on inflammation and alendronate on bone resorption apparently also contributed to the maintenance of their BMD at the baseline level.
Detection of joint erosions by radiography is the “gold standard” for assessing disease progress and the effectiveness of treatment in RA. Historically, dynamic exercises with intensity adequate to improve muscle strength and aerobic capacity were thought to provoke disease activity and to accelerate the development of joint damage. However, only a few earlier randomised studies have assessed the long term effects of physical exercise on radiological joint damage.16,25,48 The present patients had the potential for an erosive disease. Nevertheless, the extent of radiographic damage remained low throughout the whole 5 year follow up. The most probable explanation is, that our patients were actively treated with DMARDs during the entire follow up period as depicted in fig 1.30 Furthermore, the efficacy as well as the safety of the treatment was confirmed with regular clinical assessments and laboratory tests by a rheumatologist. Luukkainen et al showed a quarter of a century ago that radiographic damage in patients with RA can be retarded over 5 years with early and active treatment with intramuscular gold.48 Recent results of two randomised clinical trials confirm the benefits of early and active treatment on the development of joint destruction in early RA over a 5 year period.49,50 Thus, active treatment with DMARDs helps the patients with RA to use continuous dynamic exercise treatment without detrimental effects on joints. Also, the other measures of clinical disease activity confirmed the safety of active training with the premises applied.
One limitation of the study was that the patients in the CG required more active treatment—for example, with prednisolone and with antiresorptive drugs. Thus, it is impossible to unambiguously conclude that the strength changes seen are solely due to the exercise intervention. A strength of the study was that the rheumatologist who assessed the clinical status and x ray findings of the patients did not know which group the patients were in. On the other hand, the physiotherapists were not “blinded”. An advantage of the study is that it was performed, and provides long term evidence, in a real clinical setting. In contrast, most of the earlier short term studies were carried out in expensive laboratory settings, but we used low tech and low cost systems that allow patients with RA to exercise at home.
In conclusion, individually tailored and regularly conducted physical exercises provide long term benefits for patients with early RA. Structural joint damage remained low and clinical disease activity decreased during the whole 5 year follow up, indicating that patients actively treated with DMARDs can safely carry out the applied, individually tailored, moderate intensity physical activity.
Acknowledgments
This study was supported by a grant from the Central Finland Health Care District.