Article Text

Abstract
Objectives: To describe the impact of musculoskeletal pain (MP); to compare management of MP by the population and by primary care physicians; and to identify misconceptions about treatment.
Methods: 5803 people with MP and 1483 primary care physicians, randomly selected, in eight European countries were interviewed by telephone. A structured questionnaire was used to ask about usual management of MP and perceived benefits and risks of treatment. Current health status (SF-12) was also assessed.
Results: From primary care physicians’ perceptions, MP appears to be well managed. All presenting patients are offered some form of treatment, 90% or more doctors are trying to improve patients’ quality of life, and most are aware and concerned about the risks of treatment with NSAIDs. From a population perspective, up to 27% of people with pain do not seek medical help and of those who do, several wait months/years before seeing a doctor. 55% or fewer patients who have seen a doctor are currently receiving prescription treatment for their pain. Communication between doctors and patients is poor; few patients are given information about their condition; and many have misconceptions about treatment.
Conclusions: Management of MP is similar across eight European countries, but there is discordance between physician and patient perspectives of care. Some people with pain have never sought medical help despite being in constant/daily pain. Those who do seek help receive little written information or explanation and many have misperceptions about the benefits and risks of treatment that limit their ability to actively participate in decisions about their care.
- musculoskeletal pain
- arthritis
- pain management
- non-steroidal anti-inflammatory drugs
- side effects
- AAG, Arthritis Action Group
- GI, gastrointestinal
- MP, musculoskeletal pain
- NSAIDs, non-steroidal anti-inflammatory drugs
- OA, osteoarthritis
- OTC, over the counter
- RA, rheumatoid arthritis
Statistics from Altmetric.com
- AAG, Arthritis Action Group
- GI, gastrointestinal
- MP, musculoskeletal pain
- NSAIDs, non-steroidal anti-inflammatory drugs
- OA, osteoarthritis
- OTC, over the counter
- RA, rheumatoid arthritis
Chronic musculoskeletal pain (MP) is a debilitating condition that affects over 100 million people in Europe and around one in four people in less developed and more developed countries world wide.1 Despite its importance to patients, healthcare practitioners, and policy makers, insufficient is currently known about its impact on quality of life, how it is managed, and what factors influence its management.2
The Bone and Joint Decade (2000–2010),3,4 supported by World Health Organisation, is the umbrella for a number of global and local initiatives aimed at improving the quality of life of people with musculoskeletal conditions. One initiative, the Arthritis Action Group (AAG), is a collaboration of rheumatologists, epidemiologists, gastroenterologists, clinical pharmacologists, orthopaedic surgeons, and primary care physicians from across Europe. Its remit is to advance the awareness of rheumatic conditions and the choices of management so that healthcare providers, patients and their carers can work in true partnership towards maximum quality of life.
The AAG undertook the first extensive pan-European survey to quantify the impact of MP on quality of life, to describe current management, and to identify the beliefs and perceptions of treatment that are held by physicians and people with chronic MP.
METHODS
A telephone survey of primary care physicians and people with chronic MP was undertaken in eight European countries: France, Germany, Ireland, Italy, Spain, Sweden, Switzerland, and the UK. Data were collected between July 2001 and June 2002.
Participants
Primary care physicians were randomly selected from the medical registers in each of the eight countries. Eligible physicians worked in primary care and had been in practice for a minimum of 2 years. They had seen a minimum of 10 adult patients with chronic MP or arthritis in the past week.
People with MP were recruited from a population sampled by random digit dialling. Eligible participants were: male and female adults (18 years and over) who had experienced chronic (lasting for at least 5 consecutive days), non-injury related pain, swelling, or stiffness in joints (hands, knees, other joints, neck, or back) or muscles, at least once a month within the past 12 months. Participants (described collectively as the population or people with MP) are described as patients if they had sought medical help for their pain.
Data collection
The telephone survey was based on structured questionnaires designed specifically for the survey and piloted in each population before use to ensure acceptability, practicality, and semantic equivalence across all language versions. The physician and population questionnaires differed in specific content but covered the same broad areas: current management of MP, perceptions of the efficacy, benefits and risks of treatment, and treatment beliefs relating to non-steroidal anti-inflammatory drugs (NSAIDs). Participants with MP also completed a quality of life questionnaire, SF-12,5 a shortened version of the SF-36 health status questionnaire. Table 1 lists the domains covered in the questionnaires.
Domains included in the physician and population questionnaires
Data were collected locally and collated centrally by Roper Starch Worldwide and subjected to rigorous quality control to ensure the validity, completeness, and accuracy of the data.
Statistical analysis
All data were entered in SPSS databases and analysed by a member of the AAG (AJC). Population data were weighted to correct for response bias. Descriptive statistics were used to describe the management of MP separately for physicians and the population within each country. Percentages presented here represent the weighted responses for each country, with N representing the number of people who were asked the question. Data for individual countries were analysed separately and ranges of percentages represent the range across all eight countries. Between-country differences were assessed using χ2 tests for categorical data and analysis of variance for continuous data.
Ethical approval
The survey was submitted for relevant ethics approval in each of the participating countries. In the UK, submission was made to MREC who considered the application and ruled that it did not require ethics approval because recruitment of the population was direct, without any prior knowledge of their medical condition or treatment.
RESULTS
Participants
A total of 1483 primary care physicians (around 200 in each country) and 5803 patients and non-help-seekers (around 800 in each country except Switzerland (501) and Ireland (500)) were recruited (table 2). Most people with MP who had seen a physician had a self reported diagnosis (that they had been given by their physician) of “arthritis” or “wear and tear”.
Number of respondents (primary care physicians and people with MP) and demographic characteristics of respondents with MP by country
Impact of MP
In all countries, MP had an impact on quality of life. Mean SF-12 scores ranged from 39 (SD 12, min–max 11–65) in Italy to 43 (SD 10, min–max 14–60) in Switzerland. 27–56% of people with MP rated their health as poor or fair. 15–26% reported that their pain limited a lot their ability to perform moderate tasks such as vacuuming or playing golf. 38–52% reported that they had accomplished less than they would like in their daily activities as a result of their pain. Up to 57% of respondents were in constant pain and 15–22% were in daily pain.
Management of MP
Physician management
At least 90% of physicians in all countries reported a real interest in trying to improve patients’ quality of life and offered all patients some form of treatment.
Few physicians (17% or fewer in all countries except Germany (34%, n = 201) and Spain (28% n = 200,), χ2 = 281.69, p = 0.0001) routinely provided patients with written information about their condition and fewer routinely provided written information about treatment options (16% or fewer in all countries except Germany (29%, n = 201) and Spain (25%, n = 200)).
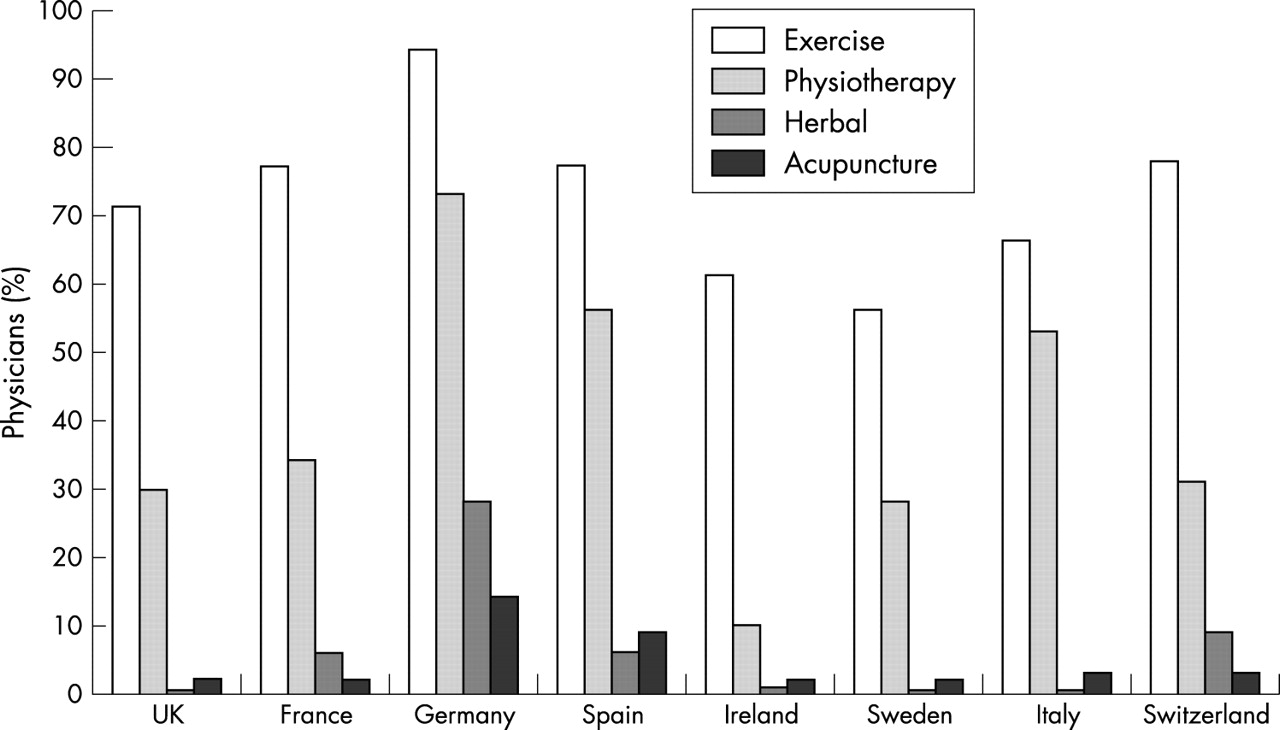
Non-pharmacological approaches most frequently used included advice to exercise and referral for physiotherapy. Figure 1 shows the percentage of physicians in each country who recommended non-pharmacological interventions to all or most of their patients.
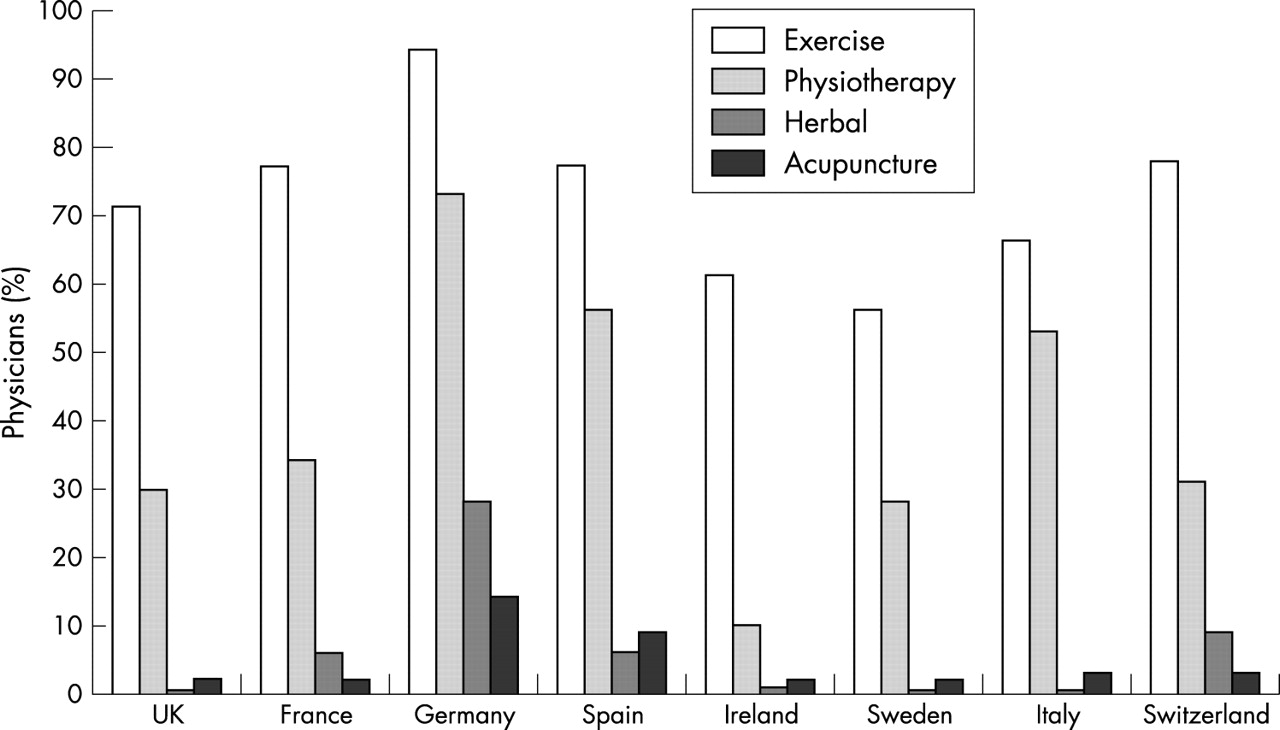
Percentage of primary care physicians in each country who recommend non-pharmacological interventions to all or most patients with MP.
First line pharmacological management differed between countries but use of NSAIDs was common in all countries except the UK. Figure 2 shows first line pharmacological management in each country.

Bar chart showing drugs prescribed as first line treatment by primary care physicians and drugs currently taken by patients with MP. The physician bars (Dr) show the percentage of primary care physicians who prescribe analgesics alone, NSAIDs alone, or both NSAIDs and analgesics as first line pharmacological treatment. The patient bars (Pt) show the percentage of patients who take analgesics alone, NSAIDs alone, a combination of analgesics and NSAIDs, non-prescription (non-Rx) drugs alone, unclassified prescription drugs, or no medication.
Population management
Although many people with MP (73–88%) in all countries had sought medical help and been given a diagnosis (48–75%), up to 27% (12–27%) had never sought medical help for their pain. At least 38% (38–57%) of these were in constant or daily pain. Those that had sought medical help might have waited several months or years before approaching their doctor. Fewer than 38% of patients had sought help within 1 week of the onset of symptoms and between 12% and 34% had waited a year or more. Although quality of life was generally poor in all people with MP, people who had sought medical help had significantly poorer quality of life than those who had never sought help (mean difference in SF-12 scores: −4.78 to −9.32, p<0.006 to p<0.0001, 95% confidence interval (CI) from −8.21 to −1.39, to −11.74 to −6.91).
Many people with MP who had seen a doctor had obtained some information about their condition or treatment (49–72%), but few had received this information from their doctor. 12–33% of patients had received written information about their condition and 10–33%, written information about their treatment from their doctor. Other sources of information included newspapers and magazines (16–35%), friends and family (11–32%), television (8–32%), and physiotherapists (10–44%).
Many patients used non-pharmacological approaches (predominantly physiotherapy (17–45%) and exercise (39–79%)) to manage their pain.
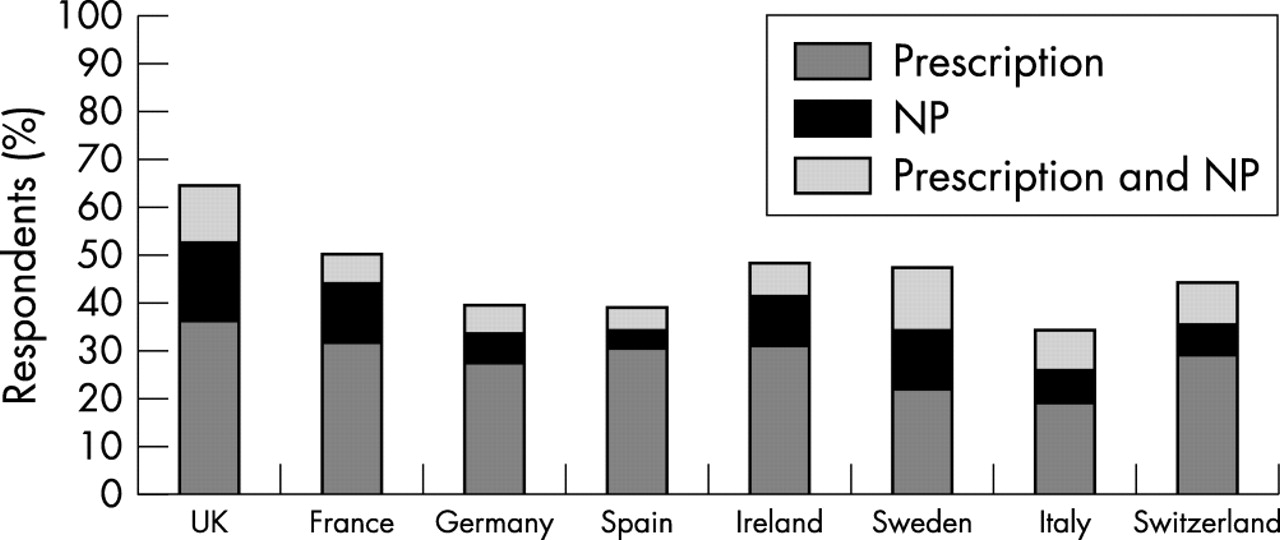
Pharmacological management of MP differed between countries. Between 34% (in Italy) and 64% (in the UK) of people with MP were currently taking drugs for their pain. Most of these (>61%) were taking a prescription drug, of whom, 42%–64% were taking an NSAID. 23%–59% were taking a non-prescription (NP) drug (fig 3). Figure 2 shows a comparison between physicians’ first line pharmacological management and patients’ current use of prescription drug by country. A small proportion of patients in each country who were taking prescription drug (4–17%) had not seen their doctor for at least 2 years. In every country, more than 40% of patients taking prescription NSAIDs (43–65%) had a self reported diagnosis of osteoarthritis (OA), “arthritis”, or “wear and tear”. 4–24% of patients taking prescription NSAIDs had a self reported diagnosis of rheumatoid arthritis (RA).

Bar chart showing the percentage of people with MP in each country who currently take drugs for pain and the type of drug taken (prescription only, non-prescription (NP), or combined prescription and NP drugs).
Perceptions of treatment: benefits and risks
Of patients taking prescription NSAIDs, 23–47% thought their treatment very effective in managing their pain. Physicians’ perceptions of treatment efficacy were similar to those of patients (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar chart showing the percentage of patients taking NSAIDs who think that their treatment is not at all or only a little effective in managing their pain. The doctors’ data represent the percentage of patients whom primary care physicians think will require a change in their treatment because of lack of efficacy.
Physician and population perceptions of treatment related risk differed. Most physicians (67–94%), except in Italy (28% n = 198), were very or somewhat concerned about the risks associated with NSAID treatment. Conversely, 37% or fewer patients taking NSAIDs were very/somewhat concerned.
There was a lack of knowledge about side effects among some patients: 19% of patients taking NSAIDs in Spain, 45–51% of patients in Sweden, Ireland, Germany, France, and the UK, and 69–75% of patients in Switzerland and Italy were aware of any side effect associated with NSAIDs, and 16–27% of patients taking drugs believed that warning signs would always precede serious gastrointestinal (GI) side effects such as ulcers. A similar proportion of physicians (2–29%) also believed that warning signs would always precede serious GI side effects. Many physicians (40–64% in all countries except Italy (26%, n = 198)) felt it best to tell patients only about the most common side effects associated with NSAIDs. Table 3 shows the percentage of patients taking NSAIDs who had established risk factors for side effects.
The percentage of patients in each country taking NSAIDs who have established risk factors for GI side effects (age, previous ulcer, comorbidity, co-medication) and the percentage of patients taking NSAIDs who have GI sensitivity (dyspepsia/acid reflux)
Most people with MP who were taking drugs reported fears of tolerance (65–77%) and addiction (64–82%, except in Spain (33%)) in relation to NSAID treatment. These views were shared by some physicians. 22–42% of physicians in all countries except Sweden (7%) endorsed perceptions of tolerance, and 26–51% (12% of Swedish physicians) agreed that daily use leads to over-reliance. More than 50% of people with MP (51–75%) in all countries except Sweden (42%) and more than 60% of physicians (61–86%) in all countries except Italy (46%) thought the side effects from drug treatment could be worse than the condition itself.
DISCUSSION
These data represent the first extensive trans-European survey of the management of MP from a physician and population perspective. Although there are some differences between countries in the management of pain, the impact of pain and perceptions of treatment are similar across all eight countries, especially in the population data.
MP across Europe is associated with a significant burden. 60–75% of people with MP are in constant/daily pain and it has an impact on quality of life, limiting the ability to perform physical and daily living activities.
From the physicians’ perspective, it seems that MP is well managed in primary care across Europe, with 90% or more doctors committed to improving patients’ quality of life, all patients offered some form of treatment for their pain, and most doctors aware of and concerned about the risks of NSAID treatment. Although there are no published guidelines for the primary care management of general MP, there are European and US guidelines for the management of OA, a predominant cause of MP.6,7 In this survey, management reported by physicians largely follows these guidelines, although physician awareness and use of guidelines was not assessed.
The population perspective, however, presents a less optimistic picture. Patients delay seeking medical help for their pain. Many do not take treatment. They lack information about their condition and treatment, and as a result, are unlikely to participate in their care in an informed way. These combined factors are likely to adversely affect their outcome.
Up to 27% of people with MP across Europe do not seek medical help for their pain despite some of them being in constant or daily pain. Among those who do seek help, a large proportion suffer months or even years before seeing their doctor. Barriers to seeking help are likely to be complex and could not be adequately predicted from this cross sectional study. Attitudinal factors or interpretation of symptoms, such as a tendency to normalise symptoms as due to age (as identified in previous studies in OA8 and RA9), may provide some explanation.
When patients do seek help, they may be offered some form of treatment, but few receive any written information about their condition or treatment. As a result, patients taking prescription NSAIDs are ill informed about the risks associated with treatment and many significantly underestimate their personal risk. Lack of relevant and meaningful information may also account for patient reported fears of addiction, tolerance, and side effects. The adverse impact of such fears on drug taking has been well documented in several patient groups10–12 and may explain low use of prescription drugs (28–54% of patients) in this study, even among patients in constant or daily pain (50–66% of patients who are not taking drugs are in constant/daily pain). For patients who are taking drugs, these fears may prevent their effective use and may in part explain why 53% or more of patients taking prescription NSAIDs in this study report some lack of efficacy. That such fears are shared by some physicians is likely to reinforce patient beliefs and misperceptions and implies a lack of awareness of the different treatment choices available for patients with specific risk profiles.13
Lack of accurate, meaningful information that inhibits patients’ ability to make informed choices about treatment is a major barrier to patient involvement in disease management. Patient involvement has been highlighted as a priority by many countries across Europe on the basis that it is associated with higher levels of patient satisfaction, a reduced symptom burden, and fewer referrals for specialist care.14–16 In the UK, self management programmes for arthritis17 have been available for some time and are now being expanded to other chronic conditions through the Expert Patient Programme. In this respect, the results from this study are disappointing. Few patients received written information or explanation from their doctor and many had misperceptions about the risks and benefits of treatment. The likely result of this is limited involvement in their care, lack of choice in the treatment they receive, no knowledge of the different risks and benefits of individual treatments, low adherence to effective treatment, and poor long term outcome.
The results of this survey highlight discordance between medical perceptions of the management of MP and population experience that is common to many European countries. Discrepancy between medical and patient perspectives has been described in relation to assessment of physical and mental functioning, pain ratings, psychological distress, and disease activity in patients with rheumatic disease,18–21 with primary care physicians generally underestimating the impact or severity of patients’ pain or psychological distress.22,23 This probably accounts for doctors’ difficulty in identifying those disease or treatment outcomes of importance to patients24 and may explain some of the discordance reported in this study. If doctors and patients have different perceptions of, and priorities for, disease and outcome patients’ needs or fears may not be addressed and patients may be less likely to adhere to treatment recommendations. Although satisfaction surveys among many patient populations report high levels of satisfaction with care, dissatisfaction is associated with a lack of patients’ involvement in their care or the inability of the doctor to deal with their needs.25 The OMERACT (Outcome Measures in Rheumatology Clinical Trials) Patient Perspective international initiative is an attempt to ensure that assessment of disease and outcome is based on factors of importance to patients.
Although many primary care physicians are providing good clinical care, the effectiveness of the treatment they offer could be maximised by changes in the ways in which they communicate information about the condition and treatment options, improved assessment of patients’ risk, elicitation of patients’ perceptions and priorities for treatment, and more appropriate use of available treatments.
Authors and contributors
AD Woolf was involved in the design of the study, interpretation of the results, drafting and revising the paper, and approving the final version for publication.
H Zeidler, U Haglund, S Chaussade, D Cucinotta, DJ Veale, and E Martin-Mola were involved in the interpretation of the results, revising the paper, and approving the final version for publication.
AJ Carr was involved in the analysis of the data, interpretation of the results, drafting and revising the paper, and approving the final version for publication.
The other members of the Arthritis Action Group: Professor P Bertin, Professor Frolich, Dr Bolten, Professor B Michel, Mr A Blower, Dr A Aly, Dr N Amin, Professor M Guslandi, Dr Garcia Rodriguez, and Professor S Lohmander were actively involved in the review and interpretation of the data and approved the final version of the paper for publication.
Acknowledgments
Financial support for the study: the Arthritis Action Group (an independent group of specialist physicians) acknowledges that this survey was supported by an educational grant from Pharmacia Corporation and Pfizer Inc. The Arthritis Action Group retains complete control over the study instrument design, data interpretation, and communication of results.