Article Text

Abstract
Objective: To assess the effect of a combination treatment using anti-hyperuricaemic agents with fenofibrate and/or losartan on uric acid metabolism in hypertriglyceridaemic and/or hypertensive patients with gout.
Methods: Twenty seven patients with gout were included in a fenofibrate plus anti-hyperuricaemic agents combination study, and 25 in a losartan plus anti-hyperuricaemic agents combination study. Serum uric acid concentration, uric acid clearance, and 24 hour urinary uric acid excretion were measured before and two months after the addition of fenofibrate (300 mg once daily) or losartan (50 mg once daily) to anti-hyperuricaemic agents.
Results: Combination therapy of fenofibrate or losartan with anti-hyperuricaemic agents, which included benzbromarone (50 mg once daily) or allopurinol (200 mg twice a day), significantly reduced serum uric acid concentrations in accordance with increased uric acid excretion.
Conclusion: A combination of fenofibrate or losartan with anti-hyperuricaemic agents is a good option for the treatment of gout patients with hypertriglyceridaemia and/or hypertension, though the additional hypouricaemic effect may be modest.
- losartan
- fenofibrate
- uric acid
- hypertension
- hypertriglyceridaemia
Statistics from Altmetric.com
Patients with gout often have complications of visceral fat obesity, hypertension, hyperlipidaemia, and impaired glucose tolerance.1,2 Hyperlipidaemia is seen in about 50% of Japanese patients with gout,3 while hypertension is found in 25–50% patients with gout worldwide.4 Therefore, it is important to treat these patients with such metabolic abnormalities by correcting the hypertriglyceridaemia and/or hypertension as well as the hyperuricaemia.
Fenofibrate, a hypolipidaemic fibric acid derivative, and losartan, an angiotensin II receptor antagonist, have been reported to reduce serum uric acid concentration through their enhanced renal clearance.5,6 The uricosuric action of losartan is exerted by its inhibition of the urate/anion exchanger in the brush-border membrane of the renal proximal tubules,7 whereas the action of fenofibrate has not yet been determined, though it may also increase urinary uric acid excretion through inhibition of this exchanger. The effect of a combination therapy of fenofibrate or losartan with anti-hyperuricaemic agents has not been extensively studied so far. Herein, we report our investigation of the beneficial effects of fenofibrate and losartan in hypertriglyceridaemic and/or hypertensive patients with gout receiving anti-hyperuricaemic agents.
PATIENTS AND METHODS
Patients
After specific informed consent was obtained, 27 male patients with gout with hypertriglyceridaemia and 25 male patients with gout with hypertension were enrolled in this study. Hypertriglyceridaemia was defined as a fasting serum triglyceride level of >1.69 mmol/l, and hypertension was defined as a systolic blood pressure of >140 mm Hg or diastolic blood pressure of >90 mm Hg, or both, on at least two occasions. The diagnosis of primary gout was made on the basis of criteria outlined by the American Rheumatism Association.8 Uric acid overexcretion was defined as a urinary uric acid excretion level ⩾2.85 mmol/m2/day, while uric acid underexcretion was defined as <2.84 mmol/m2/day together with a uric acid clearance of <6 ml/min, according to the criteria of Yamamoto et al.9 Drugs that might interfere with uric acid metabolism, blood pressure, and lipid parameters, except for allopurinol, benzbromarone, fenofibrate, and losartan, were stopped at least one month before and during the study. All patients were followed up as outpatients. Table 1 lists the demographic characteristics of the patients at baseline.
Demographic profiles of patient groups at baseline. Results are shown as mean (SEM)
Design of study 1: Effect of fenofibrate on uric acid metabolism in hypertriglyceridaemic patients with gout receiving anti-hyperuricaemic agents
Patients with gout with hypertriglyceridaemia were divided into two groups according to uric acid metabolism derangement, which resulted in 14 in the uric acid underexcretion type group and 13 in the uric acid overexcretion type. After three months of treatment with anti-hyperuricaemic agents (50 mg once daily of benzbromarone for underexcretory gout and 200 mg twice a day of allopurinol for overexcretory gout, except for one underexcretory gout patient treated with allopurinol because of urolithiasis), 300 mg once daily of fenofibrate was given to patients in both groups for two months. Uric acid metabolism, which included serum uric acid concentration, uric acid clearance, and 24 hour urinary uric acid excretion, as well as lipid profiles, were compared before and at the end of the two month fenofibrate administration.
Design of study 2: Effect of losartan on uric acid metabolism in hypertensive patients with gout receiving anti-hyperuricaemic agents
Patients with gout with hypertension were divided into two groups according to uric acid metabolism derangement, which resulted in 13 in the uric acid underexcretion type group and 12 in the uric acid overexcretion type. After three months of treatment with anti-hyperuricaemic agents (50 mg once daily of benzbromarone for underexcretory gout and 200 mg twice a day of allopurinol for overexcretory gout, except for one underexcretory gout patient treated with allopurinol because of urolithiasis), 50 mg once daily of losartan was given to patients in both groups for two months. Uric acid metabolism, which included serum uric acid concentration, uric acid clearance, and 24 hour urinary uric acid excretion, as well as blood pressure and creatinine clearance, were compared before and at the end of the two month losartan administration.
Laboratory methods
Concentrations of uric acid in serum and urine were measured by a uricase/peroxidase method. Serum lipids, as well as serum and urinary creatinine concentrations were measured with an automated analyser in our hospital laboratory. Clearances of uric acid and creatinine were calculated from fasting blood samples and 24 hour urine data.
Statistical analysis
The results are expressed as mean (SEM). Statistical differences between or among groups were analysed by analysis of variance. Statistical significance was accepted at a p value of <0.05.
RESULTS
Study 1
Fenofibrate significantly decreased serum levels of triglyceride in both benzbromarone treated and allopurinol treated patients (benzbromarone plus fenofibrate treated patients, from 2.87 (0.34) mmol/l to 1.79 (0.23) mmol/l, p<0.01; allopurinol plus fenofibrate treated patients, from 3.04 (0.44) mmol/l to 1.66 (0.22) mmol/l, p<0.01), whereas total cholesterol levels were decreased significantly only in the allopurinol treated patients (benzbromarone plus fenofibrate treated patients, from 5.60 (0.20) mmol/l to 5.44 (0.26) mmol/l, NS; allopurinol plus fenofibrate treated patients, from 5.86 (0.18) mmol/l to 5.40 (0.17) mmol/l, p<0.01). HDL-cholesterol levels were not significantly changed in either group (benzbromarone plus fenofibrate treated patients, from 1.17 (0.08) mmol/l to 1.31 (0.08) mmol/l, NS; allopurinol plus fenofibrate treated patients, from 1.30 (0.06) mmol/l to 1.40 (0.09) mmol/l, NS). Further, alkaline phosphatase activity fell significantly in both benzbromarone plus fenofibrate treated and allopurinol plus fenofibrate treated patients.
Figures 1A, B, and C indicates that the addition of fenofibrate to benzbromarone caused a significant decrease in serum uric acid (from 350.9 (11.9) μmol/l to 297.4 (17.8) μmol/l, p< 0.01), in accordance with increased uric acid clearance (from 6.6 (0.4) ml/min to 9.4 (0.7) ml/min, p<0.01) and 24 hour urinary uric acid excretion (from 2.17 (0.11) mmol/m2/day to 2.56 (0.10) mmol/m2/day, p< 0.01). Similarly, the addition of fenofibrate to allopurinol (figs 1D, E, and F) caused a significant decrease in serum uric acid (from 362.8 (11.9) μmol/l to 309.3 (17.8) μmol/l, p<0.01), in accordance with increased uric acid clearance (from 4.6 (0.3) ml/min to 7.7 (0.7) ml/min, p<0.01) and 24 hour urinary uric acid excretion (from 1.57 (0.08) mmol/m2/day to 2.18 (0.13) mmol/m2/day, p<0.01). In both groups, clinical features, including body mass index (BMI), alcohol consumption, blood pressure, creatine kinase (CK), and liver and renal function did not change after the co-administration of fenofibrate (data not shown).

Changes in uric acid metabolism at baseline (before) and after the addition of fenofibrate. (A, B, C) 1, baseline; 2, benzbromarone; 3, benzbromarone + fenofibrate. (D, E, F) 1, baseline; 2, allopurinol; 3, allopurinol + fenofibrate.
Study 2
Losartan significantly decreased systolic and diastolic blood pressure in both benzbromarone treated and allopurinol treated patients (benzbromarone plus losartan treated patients, 160 (3)/101 (2) mm Hg v 137 (3)/83 (1) mm Hg, p<0.01; allopurinol plus losartan treated patients, 161 (4)/101 (1) mm Hg v 129 (3)/80 (2) mm Hg, p<0.01). However, creatinine clearance did not significantly change before or after the administration of losartan (benzbromarone plus losartan treated patients, from 93.1 (3.9) ml/min to 93.7 (4.3) ml/min, NS; allopurinol plus losartan treated patients, from 112.4 (6.0) ml/min to 109.3 (7.0) ml/min, NS).
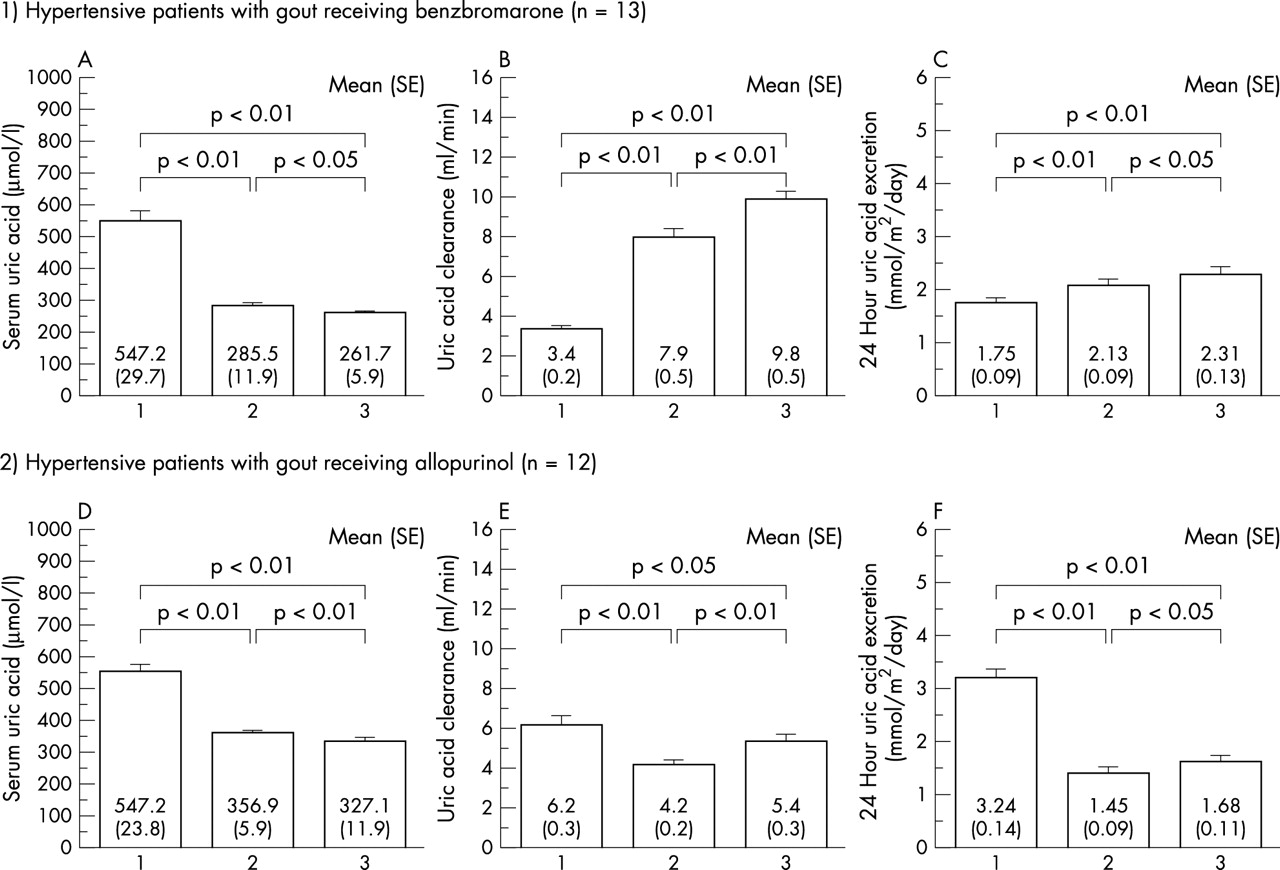
Figures 2A, B, and C show that the addition of losartan to benzbromarone caused a significant decrease in serum uric acid (from 285.5 (11.9) μmol/l to 261.7 (5.9) μmol/l, p<0.05), in accordance with increased uric acid clearance (from 7.9 (0.5) ml/min to 9.8 (0.5) ml/min, p<0.01) and 24 hour urinary uric acid excretion (from 2.13 (0.09) mmol/m2/day to 2.31 (0.13) mmol/m2/day, p<0.05). Similarly, the addition of losartan to allopurinol (figs 2D, E, and F) caused a significant decrease in serum uric acid (from 356.9 (5.9) μmol/l to 327.1 (11.9) μmol/l, p<0.01), in accordance with increased uric acid clearance (from 4.2 (0.2) ml/min to 5.4 (0.3) ml/min, p<0.01) and 24 hour urinary uric acid excretion (from 1.45 (0.09) mmol/m2/day to 1.68 (0.11) mmol/m2/day, p< 0.05).

{kind=link}
{kind=link}
Changes in uric acid metabolism at baseline (before) and after the addition of losartan. (A, B, C) 1, baseline; 2, benzbromarone; 3, benzbromarone + losartan. (D, E, F) 1, baseline; 2, allopurinol; 3, allopurinol + losartan.
In both groups, clinical features including BMI, alcohol consumption, and liver and renal function did not change after the co-administration of losartan (data not shown).
DISCUSSION
It has been extensively reported that patients with gout often have the complications of hypertriglyceridaemia and hypertension, with a prevalence of 50–75% and 50%, respectively.3,4 Therefore, inclusive treatment for hypertriglyceridaemia or hypertension seems necessary for patients with gout who have these complications, as well as for the correction of hyperuricaemia.
Fenofibrate, a hypolipidaemic agent, and losartan, an angiotensin II receptor antagonist, have been reported to decrease serum uric acid levels by increasing the renal clearance of uric acid. It has been shown that fenofibrate alone decreases serum uric acid by 20%,10 whereas losartan alone decreased it by 13%.11 As a result, these agents seem to hold promise for the treatment of hyperuricaemic patients with hypertriglyceridaemia or hypertension. However, studies of co-administration of fenofibrate or losartan with anti-hyperuricaemic agents are rare, and only one is known to have examined the co-administration of allopurinol and fenofibrate,12 though it is well known that a single administration of fenofibrate or losartan decreases serum uric acid concentration.
Our results demonstrated an additive uric acid lowering effect of fenofibrate and/or losartan in hypertriglyceridaemic and/or hypertensive patients with gout who were receiving anti-hyperuricaemic agents. According to Hepburn et al, the addition of fenofibrate at 200 mg/day to allopurinol in three patients with gout for three weeks caused a 35–39% fall in serum uric acid concentration together with a doubling of uric acid clearance.12 In our study a combination of fenofibrate at 300 mg/day with allopurinol or benzbromarone reduced serum uric acid levels by 15% and 15%, respectively, whereas a combination of losartan and allopurinol or benzbromarone reduced them by 11% and 15%, respectively. The combination of fenofibrate with anti-hyperuricaemic agents in this study did not produce a greater fall in serum uric acid level than that reported by Bastow et al10 and Hepburn et al.12 Although the reasons for this uric acid lowering effect by fenofibrate plus allopurinol remain unknown, our results suggest that a combination of these agents is beneficial in the treatment of hypertriglyceridaemia and/or hypertension as well as hyperuricaemia in patients with gout who have these complications.
Twenty four hour urinary uric acid excretion did not exceed 6.5 mmol/m2/day, a value indicative of a greater than 50% risk for the development of urolithiasis,6 after two months of a combination treatment with benzbromarone and fenofibrate and/or losartan. However, co-administration of fenofibrate and/or losartan with benzbromarone as an initial treatment of hyperuricaemic patients with hypertriglyceridaemia and/or hypertension may cause urolithiasis by an unexpectedly strong uricosuric action, though uricosuria induced by losartan may not cause an increased incidence of urolithiasis because of its urine alkalinisation action.13 Moreover, it seems necessary to start allopurinol before the initiation of fenofibrate and/or losartan when treating uric acid overexcretion type hyperuricaemic patients with hypertriglyceridaemia and/or hypertension, in order to prevent the development of urolithiasis, because an initial administration of fenofibrate or losartan to these patients may cause an exaggerated excretion of uric acid.
Another problem is the possible attenuated uric acid lowering effect of allopurinol during co-administration with fenofibrate or losartan, because these combinations are known to increase oxypurinol (an active allopurinol metabolite) clearance in addition to uric acid clearance.14,15 However, in this study, co-administration of allopurinol and fenofibrate or losartan caused further decreases in serum uric acid levels, as compared with allopurinol alone. Therefore, at least in clinical practice, there should be no concern about the attenuated uric acid lowering effect of allopurinol during co-administration with fenofibrate and/or losartan.
In summary, we conclude that an additive uric acid lowering effect can be expected with the addition of fenofibrate and losartan in hypertriglyceridaemic and/or hypertensive patients with gout receiving anti-hyperuricaemic agents, though the additional hypouricaemic effect may be modest. Thus, the use of these agents seems preferable for patients with metabolic syndrome X (plus).