Article Text

Abstract
Objective: To measure serum interleukin 18 (IL18) and IL18 binding protein (IL18BP) levels in patients with inflammatory arthropathies, and to identify associations with disease status and the response to treatment.
Methods: Serum samples were obtained before and after methotrexate treatment from patients with rheumatoid arthritis (RA) and psoriatic arthritis (PsA) attending an early arthritis clinic. IL18 and IL18BP were measured by enzyme linked immunosorbent assay (ELISA).
Results: Sixty patients with RA and 13 with PsA were evaluated. Serum IL18 levels were significantly higher in RA than in PsA (p<0.001). After six months' treatment with methotrexate, IL18 levels were reduced, but the differences were not significant (p=0.052). In cross sectional analyses, no correlations between IL18 levels and measures of disease activity or structural damage in RA were found. In longitudinal analyses, no correlations between IL18 levels and the response to treatment or the degree of progressive joint damage were found. Similarly, IL18BP levels were raised in RA, and were not associated with measures of the clinical status or the response to treatment.
Conclusion: Raised serum levels of IL18 are consistent with a pathophysiological role in RA. However, in this study measurement of circulating IL18 and IL18BP did not correlate significantly with clinical measures of disease activity or the response to treatment in patients with early RA.
- interleukin 18
- rheumatoid arthritis
- BP, binding protein
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- IL, interleukin
- MTX, methotrexate
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- rh, recombinant human
Statistics from Altmetric.com
- BP, binding protein
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- IL, interleukin
- MTX, methotrexate
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- rh, recombinant human
The pathophysiology of rheumatoid arthritis (RA) is complex.1 Proliferating synovium may extend over the surface of adjacent articular cartilage to form a pannus. Cells originating in the synovium, cartilage, and bone that have the ability to degrade joint tissues accumulate at the junction between pannus and cartilage. The accumulating cells produce proinflammatory and destructive mediators, including cytokines and their inhibitors.2
Interleukin 18 (IL18) was first identified as an interferon γ-inducing factor.3,4 It is closely related to IL1α and IL1β. Two IL18 receptors, IL18Rα and IL18Rβ, have been identified and cloned, and both are important for IL18 signalling. IL18 is a pleiotropic cytokine that has costimulatory functions on Th1 cytokines. IL18 mRNA is widely expressed in human tissues. IL18 binding protein (IL18BP) belongs to a new family of secreted proteins which act as inhibitors of IL18 signalling.5 IL18BP effectively blocks IL18 by forming a high affinity complex that exhibits a very low dissociation rate.
The demonstration of IL18 mRNA and protein in the synovial tissues of patients with RA suggested a role in pathogenesis.6,7 It has also been suggested that IL18 may be an important therapeutic target in patients with inflammatory arthritis.8,9 This study aimed at evaluating sequential serum samples from patients with early inflammatory arthritis to determine if circulating levels of either IL18 or IL18BP were associated with measures of the clinical status, disease course, and response to treatment.
PATIENTS AND METHODS
Patients and serum samples
Samples were selected from a serum bank obtained from patients attending the early arthritis clinic at St Vincents University Hospital, Dublin. All patients had presented within two years of the first symptom of arthritis and had an established diagnosis of RA10 or psoriatic arthritis (PsA).11 None had previously received disease modifying antirheumatic drugs (DMARDS). In some patients, paired serum samples obtained immediately before and approximately six months after starting methotrexate (MTX) treatment were evaluated. Serum samples from healthy blood donors served as normal healthy controls. Serum levels of C reactive protein (CRP) were evaluated as measures of disease activity. Joint damage as quantified by a modified Sharp method12 in paired radiographs of hands and feet was obtained before and six to 26 months after starting MTX treatment. The observed change in the joint damage score was converted to an estimated change per year of follow up. All radiographs were evaluated by a single experienced investigator (BB) without knowledge of their sequence or of the clinical and laboratory details.
Measurement of IL18 levels in serum
Serum IL18 levels were measured by enzyme linked immunosorbent assay (ELISA) at the Division of Immunology and Allergy, University Hospital, Geneva. To select the optimal assay for the study, IL18 recovery and the effect of IL18BP were assessed by three commercially available assays: Medical and Biological Laboratories (MBL), Nagoya, Japan; R&D Systems Inc, MN, USA, and Diaclone, Besancon, France. Firstly, 250 or 500 pg/ml of recombinant human (rh) IL18 (Serono Pharmaceutical Research Institute, Geneva, Switzerland) was added to normal human sera and the total IL18 was measured (data not shown). Then, 500 pg/ml rhIL18 was added to serum from a patient with RA, both in the presence and absence of 1500 pg/ml rhIL18BP (Serono Pharmaceutical Research Institute). The assay (MBL, Nagoya, Japan) in which increasing serum concentrations of IL18 were clearly demonstrated after spiking, and in which the presence of rhIL18BP did not alter the results, was selected for the remainder of the study. The development and validation of the assay has been previously described.13 The concentration of IL18 demonstrated in normal human serum by the manufacturer ranged between 37 and 215 pg/ml.
Measurement of IL18BP levels in serum
Serum IL18BP levels in patients with RA were measured by ELISA at the Department of Molecular Genetics, Weizmann Institute of Science, Rehovot, Israel. The details of the method have been previously published.14
Statistical analysis
Analysis of the data was performed using Mann-Whitney U test, Student's t test, and Spearman's rank correlation.
RESULTS
Clinical and demographic details
Sixty patients with RA and 13 with PsA were studied. The mean disease duration was 7.7 months in patients with RA and 10.3 months in PsA. As expected, the patients with RA had more swollen joints and higher CRP values (mean swollen joint count and CRP in RA, 11.6 and 66.2 mg/l, respectively; PsA, 6.1 and 39.6 mg/l). Additional serum samples were obtained from 29 of the patients with RA, and from all of the patients with PsA, about six months after starting MTX.
Serum IL18, IL18BP and disease activity
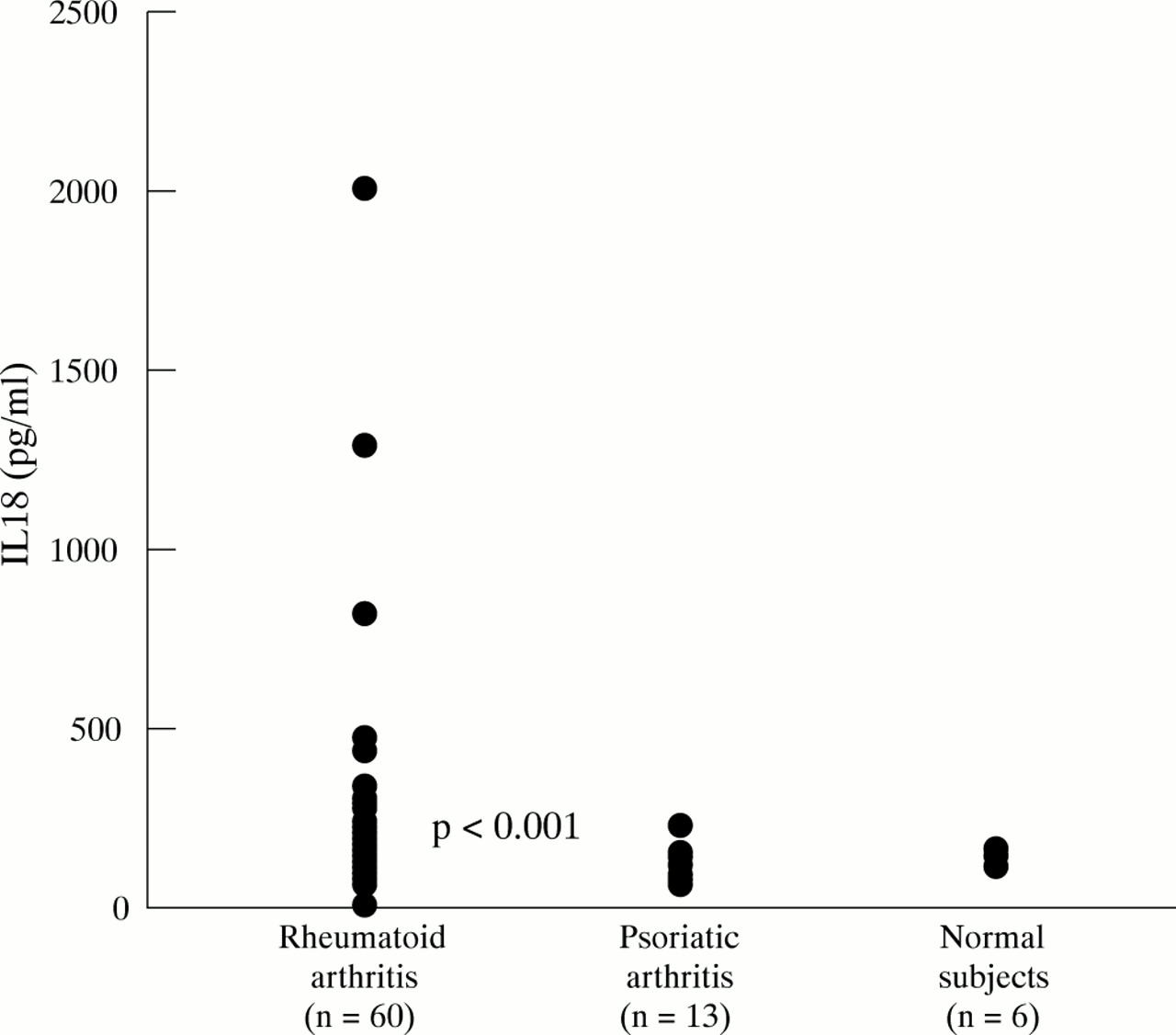
Serum levels of IL18 were significantly higher in RA than in PsA (p< 0.001) (fig 1). The range in sera from six normal healthy controls was similar to the normal range provided by the manufacturer (see “Patients and methods”). In patients with RA, no statistically significant correlations between serum levels of IL18 and the number of swollen joints or the CRP levels were found. Serum IL18BP levels in patients with RA ranged between 0.6 and 25.8 ng/ml (mean 7.8). No statistically significant correlations between serum levels of IL18BP and the number of swollen joints or the CRP levels were found. Similarly, there were no correlations between the circulating IL18:IL18BP ratios and measures of the clinical status.

Serum IL18 levels in patients with RA and PsA, and in normal healthy control subjects.
Serum IL18, IL18BP and methotrexate treatment
Twenty nine patients with RA received MTX treatment (12.5–20 mg/week). Serum samples obtained after approximately six months' treatment were evaluated. As expected, a significant fall in serum CRP values was seen (p=0.003) (fig 2A). The serum levels of IL18 were also lower after MTX treatment, but the differences were not significant (p=0.052) (fig 2B). After treatment, IL18BP levels were not significantly different from the pretreatment values (p=0.105).

{kind=link}
{kind=link}
Serum CRP (A), and IL18 (B) levels in patients with RA before and after treatment with MTX.
Serum IL18, IL18BP and joint damage
Paired radiographs, obtained immediately before and at least six months after starting treatment with MTX, were available from 14 patients with RA. Convincing evidence of joint damage was present in 12: the total modified Sharp score ranged from 1 to 41 (mean 15.4) (table 1). A cross sectional analysis failed to reveal a correlation between IL18 values and the total Sharp score. An unexpected inverse correlation was seen between IL18 levels and the degree of joint space narrowing (rs=-0.60; p=0.03). No correlation was found with the erosion score (rs=0.10; p=0.72). No correlations between the levels of IL18BP and measures of joint damage were seen.
Joint damage in patients with early rheumatoid arthritis
The interval between the paired radiographs ranged from six to 26 months. Increased joint damage was seen in 11 patients (79%) (table 1). No correlations were seen between the pretreatment or post-treatment IL18 levels and any measure of progressive joint damage, whether expressed as the final score or as the estimated change per year from the pretreatment score. There were no correlations between the pretreatment and post-treatment IL18BP levels and any of the measures of joint damage.
DISCUSSION
The patients selected for this study were attending a dedicated early arthritis clinic. Serum levels of IL18 were significantly greater in patients with RA than in PsA. In RA, serum levels of IL18 were independent of pretreatment measures of disease activity. There was an inconsistent relationship between serum levels of IL18 and radiographic measures of joint damage. IL18 levels were not significantly altered after six months' treatment with MTX. Serum IL18BP levels were also raised in this study with a mean value that was about three times higher than the mean value reported in healthy subjects by the same laboratory.14 The levels of IL18BP in serum were also independent of the clinical measures of disease activity and the response to treatment.
The three commercially available IL18 assays that were evaluated in this study produced different results. This phenomenon has been previously seen in other cytokine immunoassays where specific circulating inhibitory factors, such as soluble receptors and binding proteins, were present in serum samples.15,16 Moreover, in longitudinal studies of chronic diseases, serum cytokine levels may be poor indicators of clinical change. Immunoassays depend on the quality of the capture and detection antibodies. The antibodies may have different affinities, or recognise different epitopes on the cytokine molecule. For example, the antibodies employed in IL18 immunoassays may bind to natural and recombinant proteins differently, and may even distinguish between recombinant proteins originating from different sources. The ability of the antibodies to capture free and binding protein-associated IL18 is also likely to modify the sensitivity of the assay. The assay selected for this study exhibited linear recovery of IL18 in serum samples that had been spiked with rhIL18, and was not altered by the addition of recombinant IL18BP. This suggests that the assay detected both free and IL18BP-bound IL18. However, the possibility that rheumatoid factors present in the serum of patients with RA interfere with IL18 measurement could not be excluded. The assay used in this study was similar to that used in recent studies, which showed no correlation between serum IL18 and rheumatoid factor levels.7,17 In these studies, IL18 bioactivity was considerably weaker than the concentration of IL18 measured by ELISA, confirming that the assay detects both active and inactive proteins.
The demonstration of raised serum levels of IL18 highlighted in this study is consistent with the hypothesis that IL18 has a pathophysiological role in RA.6–9,18 In a recent study, significantly raised levels of IL18 were demonstrated in the serum and synovial fluid of patients with RA.7 The patients had chronic disease (>2 years' duration) and were receiving DMARDs and low dose corticosteroids. Two further studies demonstrated markedly raised serum levels of IL18 in patients with adult onset Still's disease.17,19 In these studies the evaluation of serum samples from other systemic inflammatory diseases, including RA, suggested that overproduction of IL18 might be specific for adult onset Still's disease. Serum IL18 levels in patients with active RA were similar to those in healthy control subjects. The reason for the discrepancies between these and the present study may relate to differences in patient selection or the assay conditions. The failure to find a positive correlation between IL18 levels and measures of disease activity in this study suggests that IL18 may have a limited ability to induce acute phase proteins and mediators of inflammation in early RA. The sustained rise in serum IL18 levels after MTX treatment, in contrast with the significant fall in CRP levels, supports the suggestion that the acute phase response may be largely independent of IL18. The simultaneous presence of IL18BP, which acts by blocking IL18 signalling,6 may be an alternative explanation for the dissociation between serum IL18 levels and measures of disease activity. The inverse correlation between IL18 levels and the degree of joint space narrowing was unexpected. This finding, and the lack of a positive correlation between IL18 and any measure of joint damage, may represent the coexisting protective and destructive effects of IL18 on cartilage and bone degradation.18
In conclusion, this study supports a pathophysiological role for IL18 in RA. However, as with many cytokines and their inhibitors in other chronic diseases, measurement of circulating IL18 and IL18BP does not appear to be of consistent value in the assessment of disease status or the response to treatment in early RA.
Acknowledgments
This study was supported in part by the Swiss National Fund for Research. Barry Bresnihan was supported by a grant from the Novartis Foundation, Switzerland. Serum IL18 binding protein levels were measured by Daniela Novick and Menachim Rubinstein, Department of Molecular Genetics, The Weizmann Institute of Science, Rehovot, Israel. The authors thank Dr Charles Dinarello, University of Colorado Health Sciences Center, Denver, USA, for advice during the preparation of the manuscript.