Article Text

Abstract
Objective: To examine relationships of bone quality as assessed by quantitative ultrasound (QUS) and bone mineral density (BMD, g/cm2) with quadriceps strength (QS) in women with rheumatoid arthritis (RA).
Methods: Sixty seven women with RA according to the 1987 American College of Rheumatology (ACR) criteria were examined. Mean (SD) age was 62 (13) years, mean disease duration 15 years. Most were or had been receiving glucocorticoid treatment. Calcaneal bone quality expressed as speed of sound (SOS, m/s), broadband ultrasound attenuation (BUA, dB/MHz), and stiffness was measured by QUS. BMD of the femoral neck, spine, and distal forearm was measured by dual energy x ray absorptiometry (DXA). Maximal voluntary isokinetic quadriceps strength (Nm) was assessed by isokinetic dynamometry. Pain was recorded on a visual analogue scale (VAS), disability was scored by the Stanford Health Assessment Questionnaire (HAQ), and the degree of physical impairment was expressed by the Steinbrocker index (SI).
Results: In multiple regression analyses, QS predicted SOS, BUA, and stiffness (rpartial ranging from 0.36 to 0.45, p<0.005) and femoral neck BMD (rpartial=0.30, p<0.05) independently of age, height, weight, disease duration, HAQ, VAS, SI, and cumulative steroid dose. BMD of the spine and distal forearm was not associated with QS. After adjustment for covariates, women with subnormal BMD of the femoral neck (T score <−1), had a 20% lower QS than those with normal BMD (p<0.0001).
Conclusions: Calcaneal bone quality and femoral neck BMD were associated with QS in women with RA. This finding indicates that physical activity including muscle strengthening exercises may play a part in the prevention of bone loss in these patients.
- rheumatoid arthritis
- muscle strength
- bone mineral density
- bone
- BMD, bone mineral density
- BUA, broadband ultrasound attenuation
- DXA, dual energy x ray absorptiometry
- HAQ, Health Assessment Questionnaire
- QS, quadriceps strength
- QUS, quantitative ultrasound
- RA, rheumatoid arthritis
- SI, Steinbrocker index
- SOS, speed of sound
- VAS, visual analogue scale
Statistics from Altmetric.com
- BMD, bone mineral density
- BUA, broadband ultrasound attenuation
- DXA, dual energy x ray absorptiometry
- HAQ, Health Assessment Questionnaire
- QS, quadriceps strength
- QUS, quantitative ultrasound
- RA, rheumatoid arthritis
- SI, Steinbrocker index
- SOS, speed of sound
- VAS, visual analogue scale
Bones continuously undergo change in response to imposed mechanical stress. The causal relationship between the architecture of bone and its functional loading was one of the earliest structure-function relationships recognised in modern biology.1 Although fracture risk has not yet been shown to be reduced by exercise, interventional studies and recent meta-analyses have demonstrated that physical activity may increase bone mineral density (BMD) in both pre- and postmenopausal healthy women.2–5. The positive effects of physical activity on BMD seem to be mediated by weight loading on the skeleton. In addition, the existence of positive associations between BMD and muscle strength found in healthy subjects suggests that the muscular action during activity may provide a stimulus for bone growth at the site of insertion.6–8
Bone loss is a well known complication of rheumatoid arthritis (RA).9, 10 Several factors, including disease mediated effects by the release of cytokines,11 steroid use,12 and reduced physical activity,10, 13, 14 have been implicated in its pathogenesis. Reductions in muscle strength are found already at the early stages of disease.15 With more prolonged disease duration, quadriceps strength (QS), for example, may be reduced by 20–50% compared with that in healthy age matched subjects.16, 17 It would seem reasonable to assume that BMD in RA is dependent on muscle strength, but only a few reported data on this issue are available.18–20
Women with RA bear a twofold risk of osteoporotic fracture of the spine and hip.21, 22 As the fracture risk may be higher than explained by BMD, it has been speculated that qualitative bone characteristics play a part.23 Commercial quantitative ultrasound (QUS) systems have become available for evaluating parameters associated with not only bone density but also with bone architecture and elasticity—namely, the speed of sound (SOS), broadband ultrasound attenuation (BUA), and stiffness.24, 25 Large prospective fracture studies have shown that both BUA and SOS at the calcaneus can predict osteoporotic fracture as well as dual energy x ray absorptiometry (DXA) can at the spine and hip.24, 26 SOS, BUA, and stiffness of the heel bone have been shown to be significantly compromised in women with RA, and SOS and stiffness significantly more than BMD measured by DXA at the femoral neck, spine, and distal forearm.17 QUS scanners measuring bone quality at these sites are manufactured but have not yet been sufficiently validated.27
The objectives of this cross sectional study were to examine associations of the calcaneal bone quality as assessed by QUS and BMD of the hip, spine, and forearm, with QS in women with RA.
PATIENTS AND METHODS
Patients
Sixty seven ambulatory women with RA according to the 1987 criteria of the American Rheumatism Association28 were enrolled consecutively into the study. Exclusion criteria were malignancies, untreated thyroid disease, insulin dependent diabetes mellitus, symptomatic heart disease, oedema and surgery during the previous year, and current or previous use of hormone replacement therapy, bisphosphonates, or other drugs used for the treatment or prevention of osteoporosis. To avoid joint damage during measurement of QS, patients with swollen knee joints due to acute inflammation were also excluded. Cumulative steroid doses were calculated from the patient files. Fifty six women were receiving or had been receiving steroids (cumulative prednisolone dose 0.05–66.2 g, median 2.5 g, mean 6.5 g). Twenty five women were currently receiving prednisolone (current dose 1.25–10.0 mg/day, median 5.1 mg/day, mean 5.0 mg/day).
All patients provided informed consent according to the Helsinki II Declaration. The investigation was approved by the Copenhagen ethics committee.
QUS measurements
Measurements of the left heel were performed using the Achilles ultrasound device (Lunar Corporation, USA).24 With this system, the heel is positioned between two transducers in a water bath (37°C). One transducer acts as the transmitter and the other as the receiver. The ultrasound beam is transmitted laterally through the centre of the os calcis. The two ultrasound parameters measured are SOS (m/s) and BUA (dB/MHz). A “stiffness” index (a combined parameter calculated by the computer from the BUA and SOS) is expressed as a percentage of the young adult mean value.24, 25 Measurement time is approximately three minutes.
At our laboratory, the in vivo reproducibility expressed as the root mean square coefficient of variation is 1.4% for BUA, 0.2% for SOS, and 1.2% for stiffness.17
Bone mineral density
Measurements were performed by a Norland XR-36 DXA scanner. BMD (g/cm2) was measured at the left femoral neck, left distal forearm, and spine (L2–L4). When orthopaedic material was present in the left side, the right side was measured. T scores for femoral neck and spine BMD were based on reference values for 326 healthy Danish women. As previously reported, the reproducibility of BMD measurements at our laboratory corresponds to that found by other investigators.29
Muscle strength
An isokinetic dynamometer (Cybex 6000, Cybex, Division of Lumex Inc, Ronkonkoma, NY, USA) was used to measure maximum voluntary isokinetic QS at 30°/s.30 Strength was expressed as peak torque in Newton-metres (Nm). Intrasession reproducibility in women with RA as expressed by the root mean square coefficient of variation was 6%. All measurements were performed by the same experienced examiner.
Clinical examinations and markers of disease impact
All women were examined by the same experienced rheumatologist. The numbers of swollen and tender joints (28 joint count) were registered in the women with RA. The functional class was expressed as the Steinbrocker index (SI).31 The Stanford Health Assessment Questionnaire (HAQ) was used to score patient disability.32 Pain as experienced by the women was recorded on a 100 mm horizontal visual analogue scale (VAS).
Statistical methods
Correlation coefficients (rS ) were studied using Spearman's correlation test. To examine how BMD and QUS variables were influenced by combinations of covariates, all data were ranked and partial rank correlation coefficients (rpartial) were derived from multiple regression analyses (stepwise selection).33
Analyses of between-group differences with adjustment for covariates were performed using ANCOVA. Statistical significance was accepted at an α level <0.05. Data are presented as means (SD) or as median (range). The tests were computed with SPSS/PC+ statistics V4.01.
RESULTS
Table 1 shows the general group characteristics and results for measurements of BMD, SOS, BUA stiffness and muscle strength. According to the WHO study group criteria,34 the number of women with osteopenia (−2.5<T scores<−1) and osteoporosis (T score ≤−2.5) of the femoral neck was 28 and 20, respectively. The corresponding numbers for the lumbar spine were 38 and 5.
Characteristics of the study group (n=67)
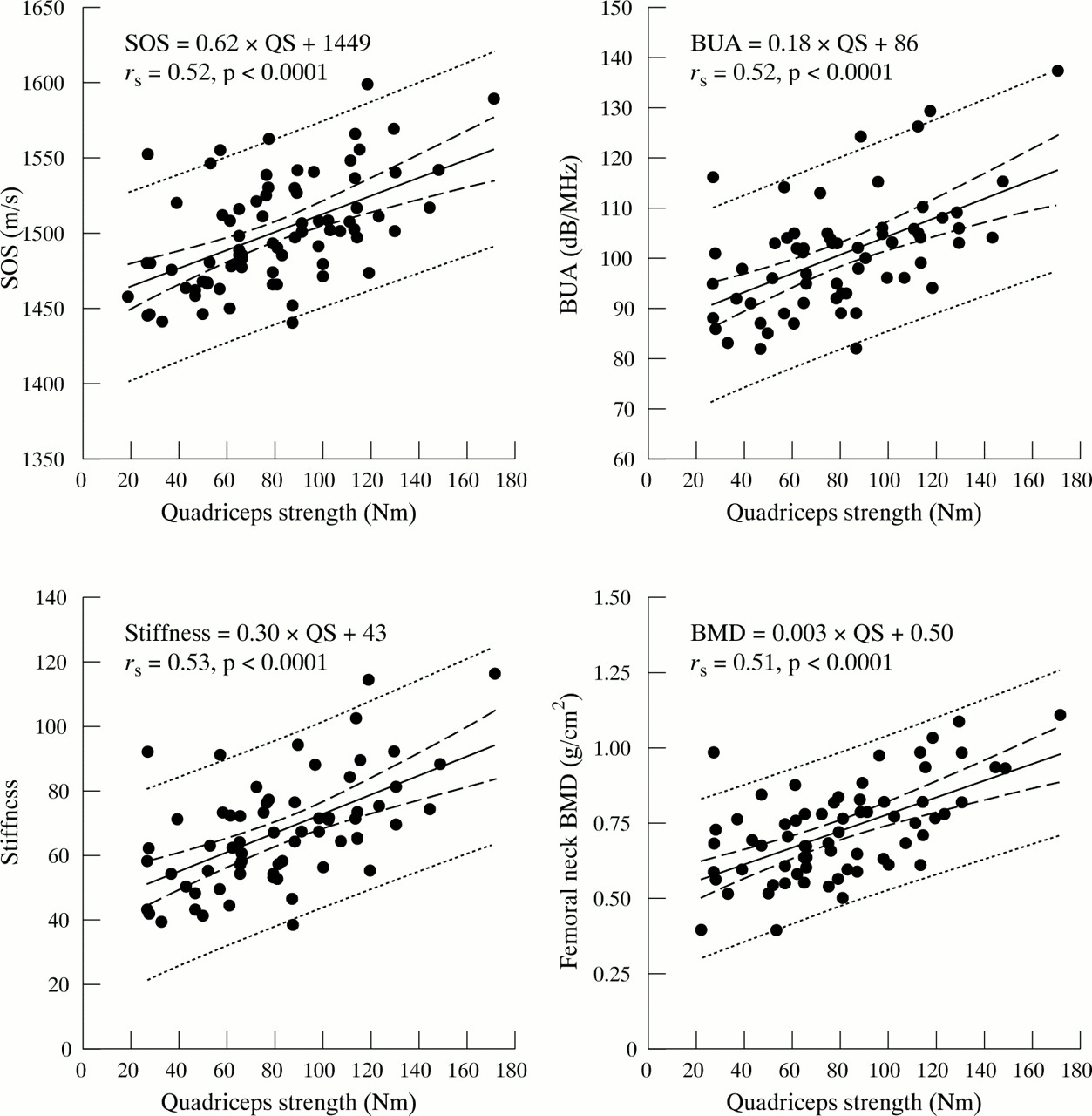
Table 2 presents simple correlations of BMD and QUS variables with age, height, weight, disease duration, SI, number of swollen and tender joints, VAS and HAQ score, cumulative and current steroid dose, and QS. Figure 1 illustrates correlations of SOS, BUA, stiffness, and femoral neck BMD with QS.
Correlations (rs) of QUS and BMD variables with other variables

Correlations of calcaneal SOS, BUA, stiffness, and femoral neck BMD with quadriceps strength in 67 women with rheumatoid arthritis. The 95% confidence intervals (inner lines) and the 95% prediction interval (outer lines) are shown.
Table 3 shows the results of multiple regression analyses with SOS, BUA, stiffness, and BMD of the hip, spine, and distal forearm as dependent variables, and age, height, weight, disease duration, SI, VAS, HAQ, cumulative steroid dose, and QS as independent variables. Age was the strongest predictor of all QUS and BMD variables (rpartial ranging from −0.51 to −0.75, p<0.0001). QS turned out to be the second strongest predictor of SOS, BUA, stiffness, and of femoral neck BMD (rpartial ranging from 0.30 to 0.45, p<0.05–0.005). Spine and distal forearm BMD was not associated with QS. Cumulative steroid dose added independently to the prediction of SOS, BUA, and stiffness (rpartial ranging from −0.34 to −0.42, p<0.05–0.005), but not to the prediction of BMD. When cumulative steroid dose was replaced by current dose in these analyses, similar results were obtained. QS remained an independent predictor of SOS (rpartial=0.39, p<0.005), BUA (rpartial=0.37, p<0.005), stiffness (rpartial=0.45, p<0.005), and femoral neck BMD (rpartial=0.30, p<0.05), and did not predict BMD of the spine and distal forearm. Current steroid dose added significantly to the prediction of SOS, BUA, and stiffness (rpartial ranging from −0.32 to −0.36, p<0.05) but not to the prediction of BMD measurements. When QS was excluded from the regression analyses, SOS, BUA, and stiffness were independently predicted by age, cumulative steroid dose (or current dose), and HAQ, and femoral neck BMD by age and HAQ. As recently reported, no associations between steroid use and muscle strength were found.35
Partial rank correlation coefficients (rpartial) obtained from multiple regression analyses with QUS variables and BMD as dependent variables
To examine quantitative differences in muscle strength between women with normal and subnormal femoral neck BMD, the women were stratified into those with T scores ≤−2.5, −2.5<T scores<−1, and T scores ≥−1. After correction for between-group differences in age, height, weight, disease duration, cumulative steroid dose, SI, VAS, and HAQ, QS was approximately 20% lower (p<0.0001) in women classified as osteopenic or osteoporotic than in those with normal BMD (fig 2). Significant differences between osteopenic and osteoporotic women could not be demonstrated.

{kind=link}
{kind=link}
Corrected quadriceps strength in 67 women with RA stratified according to femoral neck BMD and the WHO criteria for osteoporosis. Quadriceps strength is corrected for between-group differences in age, height, weight, disease duration, cumulative steroid dose, Steinbrocker index, VAS, and HAQ.
DISCUSSION
In this sample of female patients with RA, femoral neck BMD and calcaneal QUS were weakly but significantly associated with QS. The associations were not eliminated by correction for age, weight, height, disease duration, SI, HAQ, VAS, and cumulative or current steroid dose. Corrected QS was reduced by 20% in patients with subnormal BMD of the femoral neck. The variance (Rmultiple2) explained by the regressions did not exceed 72%, indicating that BMD and QUS variables are also determined by variables which were not measured in this study. Moreover, it may be that estimations of muscle strength and of other independent variables included in the regression analyses did not possess adequate precision for stronger correlations to emerge.
Several cross sectional studies have shown correlations adjusted for age and body size between muscle strength and BMD of the forearm, spine, proximal femur, and tibia in pre- and postmenopausal healthy women.6–8 The maximal effect of mechanical loading on bone is assumed to occur in regions where muscles attach to bone, but it has been proposed that muscles may also indirectly contribute to bone density at sites where they do not directly insert, as normal muscle activity is linked to the simultaneous contraction of functionally related muscle groups.6 Given this assumption, the associations of calcaneal bone quality and femoral neck BMD with QS found in this study are biologically plausible. Moreover, QS may reflect the habitual weight loading on the skeleton by physical activity in daily life, especially on the legs. The important role of weight loading in regulating bone remodelling is well known.36 In our study, however, associations of QUS and femoral neck BMD with QS were independent of HAQ score and SI, both of which may be considered as markers of physical activity.37, 38 Bone mass and muscle strength may also be indirectly related through factors which cannot be adjusted for, such as genetics influencing the size of both muscles and bones.
QS had no influence on BMD measured at more distant sites—that is, forearm and spine. Thus QS was not an indicator of global BMD. This might be attributed to the sample size. Moreover, spinal BMD may be falsely overestimated because of osteophytes or vertebral fractures. Radiographs were not obtained, but the correlation between spinal BMD and muscle strength might have been influenced by such changes.
Data on associations of BMD with muscle strength and physical activity in RA are few and inconclusive. In cross sectional studies, correlations of grip strength with hand and forearm BMD have been reported.39 Häkkinen et al found correlations of knee extensor and trunk strength with femoral neck BMD but not with spine BMD in women with recent onset RA and normal BMD. Correction for covariates was not performed.18 Other studies have indicated relationships between BMD and surrogate measures of physical performance such as self reported physical activity,18, 39–41 HAQ score,10, 42 and SI.38 Sinigaglia et al, for example, found that HAQ was an independent determinant of femoral neck and spine BMD as well as of fracture risk.42 In a prospective study, self reported physical activity was a determinant of bone mass in the radial diaphysis.41 Gough et al reported associations between HAQ score and changes in hip and spine BMD in early RA,10 whereas such associations were not found by Shenstone et al and Kroot et al.37, 43 Kroot et al reported associations between hip BMD and “activity load” in postmenopausal women, however.43 Njeh et al found significant correlations between finger QUS (SOS) and grip strength, but did not correct for potential covariates such as disease duration.44 Mayoux-Benhamou et al reported relationships between calcaneal BUA and SOS with plantar flexor strength in 45 healthy postmenopausal women.45 To our knowledge, no other data on relationships between QUS and muscle strength are available.
Exercise in RA is well tolerated and may be associated with large gains in muscle strength,19, 20, 46 but only a few interventional studies have evaluated the effect of exercise on bone mass. In women with early RA most of whom had normal BMD at baseline, 12 and 24 month dynamic strength training programmes increased muscle strength, but BMD remained nearly unchanged.19, 20 Bones in women with recent onset disease, however, will probably benefit less from exercise than those in patients with prolonged disease duration and more reduced bone mass.47 In a recent study, a 12 month weightbearing exercise programme tended to reduce bone loss from the femoral neck and spine in steroid treated women with RA, but statistical significance was not reached.48 Thus the effect of exercise on BMD in RA may be small in the short term, but it might be substantial if accumulated over a number of years through continuing exercise programmes.
The adverse effects of steroids on BMD and fracture risk are well recognised,12, 49 but the time and dose dependency is controversial.9, 10, 39, 40 Not only cumulative and current steroid dose but also time elapsed since the last treatment, length of treatment periods, and previous doses may influence the effect of steroids on bone mass. In agreement with the findings of, for example, Hansen et al,39 we found no independent associations between BMD and cumulative or current steroid dose. Calcaneal QUS variables, however, were independently associated with both cumulative and current dose, suggesting that bone quality may be more sensitive to steroids than BMD. This issue has been discussed in more detail elsewhere.17
In conclusion, femoral neck BMD and calcaneal bone quality as assessed by QUS were associated with QS in women with RA. Long term longitudinal studies are required to determine the effect of physical activity and muscle strengthening exercises on the prevention of bone loss and osteoporotic fractures in these patients.
Acknowledgments
This study was financially supported by the “Danish Hospital Foundation for Medical Research, Region of Copenhagen, The Faroe Islands, and Greenland”. We are indebted to laboratory technician Ulla Pedersen for performing the DXA and ultrasound scans.