Article Text

Abstract
Background: Effective treatment of active rheumatoid arthritis (RA) requires early diagnosis and early disease modifying antirheumatic drug (DMARD) treatment to have an impact on long term morbidity and mortality. Clinical criteria would facilitate early referral of the patient with suspected RA to a rheumatologist for definitive diagnosis and initiation of DMARD treatment at that point in the disease most likely to have an impact on the long term outcome.
Objective: To develop a referral recommendation that may serve as a clinical guide for primary care doctors, enabling them to identify patients with suspected RA during the early inflammatory stages.
Methods: Key points of the referral criteria were formed based on a thorough literature review targeting early RA, early arthritis clinics, DMARD treatment for early RA, prognostic factors of disease progression, early RA clinical trials, and quality of life. Evidence was graded using the methods defined by Shekelle et al. A draft version of the criterion was circulated among the authors for critical evaluation. A consensus integrated these comments.
Results: Clinical evidence strongly supports the observations that structural damage occurs early in active RA and that early DMARD treatment improves the long term outcome of the disease. The observations indicate that rapid referral to a rheumatologist is advised when RA is suspected. This may be supported by the presence of any of the following: ≥3 swollen joints, metatarsophalangeal/metacarpophalangeal involvement, and morning stiffness of ≥30 minutes.
Conclusion: The proposed early referral recommendation is a viable tool for primary care doctors to identify potential patients with active RA early in the disease. Early referral to a rheumatologist for definitive diagnosis and early DMARD treatment should improve the long term outcome of RA.
- early rheumatoid arthritis
- referral
- early arthritis clinics
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- EACs, early arthritis clinics
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- RCTs, randomised controlled trials
- RF, rheumatoid factor
- US, ultrasound
Statistics from Altmetric.com
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- EACs, early arthritis clinics
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- RCTs, randomised controlled trials
- RF, rheumatoid factor
- US, ultrasound
Active rheumatoid arthritis (RA) is characterised by inflammation of the synovial tissue, which, if untreated, leads to permanent structural damage and eventual long term disability. Demographically, RA is the most common form of inflammatory arthritis and affects approximately 0.5–1.0% of the global population, with an economic impact comparable with that of coronary artery disease.1 Given that ∼90% of patients with RA have some form of disability within two decades of onset,2 early diagnosis and treatment of RA is of paramount importance. However, there are obstacles to early diagnosis and treatment, including the initial delay on the part of the patient to seek medical care, followed by a delay in primary care, where the early symptoms of RA are sometimes non-specific and inconclusive.
To deal with these obstacles, a referral recommendation has been developed that may serve as a clinical guide for primary care doctors, enabling them to identify patients with suspected RA during the early inflammatory stages. Early referral, followed by specific diagnosis of active RA and initiation of disease modifying antirheumatic drugs (DMARDs) during the early inflammatory stages of RA, will improve patient outcome and long term quality of life.
PURPOSE OF THE REFERRAL RECOMMENDATION
Clinical evidence, summarised in the following discussion, provides a clear indication of the benefits of early diagnosis and early DMARD treatment for the treatment of active RA. The purpose of the referral recommendation is to provide a tool based on clinical evidence that summarises the essential and basic diagnostic criteria, allowing early identification of the patient with suspected RA for referral to a rheumatologist. A relatively brief opportunity may exist for initiating the DMARD treatment that can substantially improve the long term outcome of the disease, as well as the overall quality of life for patients with active RA.
Criswell et al show evidence of systematic differences between rheumatologists and non-rheumatologists in initiating the use of DMARDs for the treatment of RA.3 Non-rheumatologists generally delay treatment, which can result in substantial differences in the long term outcome of the disease. Other investigations4–6 have shown that patients with RA managed by rheumatologists maintained greater functional status over the duration of the disease and had better health outcomes. In addition, newer treatments require specialised administration and monitoring for maximal efficacy and safety.
METHODS: CONSENSUS DEVELOPMENT
The initial stage in the development of the early referral recommendation involved a literature search of the Medline and Current Contents databases. The key terms of the search were the phrase “early rheumatoid arthritis” AND, separately, the terms “disease progression”, “clinical trial”, “early arthritis clinics”, “mortality”, “quality of life”, and “early treatment”. Published clinical evidence was classified and graded according to the methodology defined by Shekelle et al7 and is summarised in table 1.
Classification and grading of clinical evidence
Valid classification schemes categorise clinical evidence based on the potential for bias influencing the results. Thus the least biased, and therefore the highest category evidence (Ia, table 1) is represented by meta-analyses of randomised controlled trials (RCTs). Categories Ia and Ib (evidence from at least one RCT) provide support for a grade A recommendation. Conversely, the evidence category with the greatest potential for bias (category IV) is evidence from expert committees or the opinion of respected authorities7 and supports grade D recommendations. The evidence categories are open to interpretation, as questions about efficacy of intervention are most strongly addressed by RCTs, and clinical questions about risk are more appropriately assessed by prospective cohort investigations.7 Throughout this paper, evidence categories are indicated where appropriate by a Roman numeral and evidence grade by a letter, as defined in table 1.
A draft version of the clinical recommendation was prepared synthesising the recommendation and supporting clinical evidence and was then circulated among the authors for further review and critical evaluation. A final draft of the clinical guide and referral recommendation was then generated, merging the comments and critique of the six participants; this resulted in a consensus statement for early referral recommendation.
CLINICAL PROGRESSION OF RA: JOINT DAMAGE OCCURS EARLY
Radiographically measured progression of RA remains the best method of assessing structural damage associated with the disease. An inherent problem in comparing clinical studies of radiographic progression is variability of the study designs. Three designs predominate: cross sectional studies, prospective studies of patients with disease of varying duration, and prospective follow up studies of a cohort of patients with early RA.8 Of the three designs, the prospective follow up studies of patient cohorts with early disease is the best design for assessing the risks of disease progression.
Summarising prospective studies of radiographic progression of patients with early RA, van der Heijde concludes that ∼75% of patients with early RA have joint erosions and develop the initial erosions within the first two years of symptom onset.9 These early prospective investigations present strong evidence that joint damage occurs early in the course of RA (III).
A recent comprehensive evaluation of published reports which linked structural damage to disability10 concluded that joint damage progresses at a consistent rate over the course of the disease and that it accounts for ∼25% of the disability. The statistical association between radiographic damage and disability is strongest with disease duration of >8 years; however, prevention of structural damage early in the disease is likely to preserve patient function (III).11
Bone density is also seen to decrease during the early stages of RA. Measures of the axial bone mineral density12 in patients with RA with a mean disease duration of 10.4 months showed a significant reduction of axial and appendicular bone mineral density by one year. Mineral loss was closely correlated with raised C reactive protein (CRP) levels and functional impairment. Reduced peripheral bone mineral density was also seen with persistent disease.13 Patients with early RA with a median disease duration of nine months (n=42) as a group lost a significant amount of hand bone mineral density over the 12 month period of the study compared with the control population.14 There was a concomitant worsening of the radiographic Larsen score, indicating progression of structural damage. Both studies were prospective investigations and constitute category III evidence.
Joint erosions that are evident radiographically represent permanent structural damage and have prompted the investigation of alternative imaging techniques to identify synovial changes before permanent deterioration has occurred. Both ultrasound (US) and magnetic resonance imaging (MRI) techniques have been applied to the evaluation of synovitis in patients with early RA. A controlled clinical investigation (IIa) of the interrelationship between synovitis and bone in early RA concluded that metacarpophalangeal joint bone oedema is present in the majority of patients with RA at presentation and that joint structural changes are secondary to synovitis.15
A prospective study employing blinded observers (IIb) evaluated the effectiveness of three phase bone scintigraphy, US, MRI, and contrast enhanced MRI to determine the optimal imaging method for identification of both early erosions and acute phase inflammation compared with conventional radiography.16 The early RA cohort had a mean disease duration of 19 months, and the results indicated that scintigraphy, US, and MRI were significantly more sensitive than conventional radiography at detecting early inflammatory soft tissue and destructive joint processes before radiographic damage becomes evident.
In support of the evidence for early synovitis preceding structural damage in RA, Kraan et al examined histological synovial biopsy specimens of the unaffected joints of patients with established RA for signs of inflammation.17 The synovial tissue of asymptomatic joints was characterised by infiltrating macrophages and macrophage derived cytokine expression indicative of active inflammation.
The combined clinical evidence indicates that the physiological changes induced by RA within the synovial environment are evident during the early asymptomatic phase of the disease and, when left untreated, chronic inflammation leads to structural damage in active RA. The bulk of the clinical evidence for early structural damage is derived from prospective studies and composed of category III evidence; therefore, the observation that damage occurs early is assigned evidence grade C.
Tables 2 and 3 summarise selected prospective investigations dealing with the prognostic factors for radiographic progression and disability in early RA; table 4 isolates predictive factors evaluated in early arthritis clinics (EACs). Despite the heterogeneous results from these studies, common elements in the baseline risk factors exist for both radiographic progression and disability, including involvement of large joints, disease duration of ≥3 months, involvement of hand joints, ≥2 swollen joints, high disease activity at baseline, rheumatoid factor (RF) positivity, and raised CRP levels.18 Prognostic factors for radiographic progression and disability constitute category III evidence.
Risk factors indicative of radiographic damage in early RA
Risk factors indicative of disability in early RA
Risk factors for persistent RA, evidence from EACs
EARLY DMARD TREATMENT IMPROVES RA OUTCOME
Table 5 shows the results of placebo controlled trials of early DMARD treatment for patients with early RA and disease duration <2 years. Treatment with sulfasalazine, oral gold, and hydroxychloroquine significantly reduced the clinical signs and symptoms of early RA, and hydroxychloroquine improved patient function as assessed by the Health Assessment Questionnaire (HAQ) after 11 months of treatment.
Placebo controlled trials of DMARD treatment for early RA
Analysis of delayed treatment trials (extensions of placebo controlled investigations in which the placebo group is switched to active treatment at the end point of the initial study) shows the efficacy of early DMARD treatment for early RA (table 6). In each trial the group treated at presentation with DMARDs showed significantly more improvement in efficacy parameters than the groups whose treatment was delayed. Early intervention improved patient function (reduced HAQ score in three of the four presented trials) and reduced or slowed radiographic disease progression, as well as decreasing swollen joint counts in ∼50% of the trials.
Delayed DMARD treatment trials in early RA
Recent evaluation of primary trial data from 14 RCTs of DMARD treatments in RA indicates that patients with a longer disease duration did not have such a good response as patients treated at earlier stages of the disease.19 The study also noted that prior DMARD use, RA functional classification, and disease activity also had an impact on the potential outcome of treatment (Ia).
A recently published study of an inception cohort of 622 patients with newly diagnosed RA followed up for up to 10 years, evaluated patient mortality, functional ability, and prognostic factors for mortality.20 The cohort of patients with early RA treated aggressively with DMARDs showed no excess mortality within the first 10 years when compared with the normal population, and functional ability remained constant after an initial improvement from baseline. Age at onset and male sex were the only significant prognostic factors for mortality. The results of this investigation highlight the efficacy of an early, aggressive therapeutic strategy, indicating that treatment with conventional DMARDs improves the disease course and gives long term patient benefit.
To date there have been no long term investigations of the newer biological treatments on patient mortality and functional ability; this will be critical in determining the role of these treatments in the aggressive treatment of early RA.
Randomisation and placebo controls in the summarised trials of early treatment (presented above) represent category Ia and Ib evidence and constitute grade A support for early intervention with DMARDs in early RA.
EARLY DMARD TREATMENT IMPROVES LONG TERM OUTCOME AND PATIENT QUALITY OF LIFE
In 1998, Symmons et al examined the long term mortality outcome of a cohort of 489 patients with RA.21 The cohort was divided into three groups: early presenters (disease duration ≤5 years); late presenters (disease duration >5 years); and the inception cohort with disease onset after 1 January 1964. With increased disease duration, the incidence of deaths due to infection, renal failure, and non-Hodgkin's lymphoma increased beyond that of the control population; patients with RA who presented and were treated early in the disease did better than late presenters. The study concluded that early treatment improves prognosis and that as a result the patients may have milder disease.21
Radiographic and clinical comparisons of patients with RA, treated or not treated with DMARDs,22 indicate that patients not treated with DMARDs had a significantly higher number of deformed and damaged joints. Clinical evidence indicated that long term use of DMARDs did not necessarily prevent radiographic progression of joint damage, but it significantly slowed the rate of progression compared with non-steroidal anti-inflammatory drug (NSAID) treatment alone.22
A large prospective follow up study of 2888 patients over 20 years assessed long term disability in patients treated with DMARDs.23 Increased DMARD use was associated with a better long term HAQ disability index, showing that consistent DMARD use resulted in a conservatively estimated 30% reduction in disability over the duration of RA.
Each of the three trials represents category III evidence, supporting the statement that DMARD use improves the long term outcome and quality of life over the lifetime of patients with RA.24
COMPARATIVE TOXICITY OF NSAIDS AND DMARDS
DMARD treatment in the past was initiated when “NSAIDs no longer worked,” and to a certain extent, this philosophy also served as a referral guideline when considering the aid of a rheumatologist in the treatment of patients with RA. This was based on the assumption that NSAIDs are a benign treatment for the early inflammatory stages of RA and that the potential toxicity of DMARDs precluded their use until the benefits outweighed the risks.
In recent years, it has been recognised that long term treatment with NSAIDs is associated with increased morbidity and mortality among patients with RA owing to the adverse effects of these drugs on the gastroduodenal mucosa. The more serious side effects of chronic NSAID use include peptic ulceration and upper gastrointestinal bleeding. Admissions to hospital and deaths in the American population related to gastrointestinal effects are estimated to be 26 000–47 000 and 4400–7700, respectively.25 Combined deaths related to chronic NSAID use in RA and osteoarthritis are estimated to be ∼16 500, which is comparable with the total number of deaths caused by the human immunodeficiency virus.25 Much of the clinical evidence for the toxicity of NSAIDs is derived from the Arthritis, Rheumatism, and Ageing Medical Information System (ARAMIS) database.26
Fries et al have compared toxicity profiles of NSAIDs and DMARDs by calculating a toxicity index derived from symptoms, abnormal laboratory measures, and admissions to hospital related to treatment.27, 28 Comparison of the quantitative toxicity estimates of NSAIDs and DMARDs indicates that there are no substantial differences between drug categories.27, 28 Ibuprofen, naproxen, and sulindac each had toxicity indices comparable with that of intramuscular gold.27, 28
The long term toxicity of DMARD use is at least no worse than the toxicity of chronic NSAID use, a fact supported by category III and IV evidence. DMARD treatment is usually started within three years of diagnosis in 90% of patients with RA29; therefore, most patients with RA eventually are subjected to the risks of DMARD toxicity, and it is pointless to delay treatment that may improve both long term outcome and patient function if started early.
CLINICAL EXPERIENCE: EACS
Early arthritis clinics (EACs), located predominantly in Europe, have addressed the issue of early referral and treatment of patients with early RA, providing insight into the initial stages of RA. Table 4 summarises the risk factors identified by EACs, indicating potential baseline characteristics of patients with early RA likely to have persistent RA. A variety of selection criteria were employed in these EACs, including arthritis of <12 weeks,30 arthritis of ≥1 joint for ≤6 months,31 and arthritis of <2 years.32 In a clinical evaluation of 63 patients with mild, untreated, early arthritis seen at an EAC in the UK, Green et al found that the strongest predictor of persistent disease was a disease duration of >12 weeks.33
Kim and Weisman summarise the persistence of RA in the selected groups presenting at EACs compared with RA persistence in population based studies.18 Persistent RA, classified as compliance with either the 1958 American College of Rheumatology (ACR) or 1987 ACR diagnostic criteria or clinical diagnosis, was seen in 27–68% of the EAC patients. Population based investigations indicated that the prevalence of RA was decidedly smaller, of the order of 2.6–6% in the groups studied. These observations indicate that the simple selection criteria employed in the EACs potentially allow the sensitive isolation of patients with RA whose disease is likely to be persistent and active.
The inherent problem with treatment of early RA is the long lag time between the onset of disease and referral to a rheumatologist for accurate and specific treatment. Specific analysis of the lag time between onset of symptoms and diagnosis of treatment, based on a review of medical records,34 indicates two factors that delay diagnosis: firstly, the time between symptom onset and the patient's subsequent visit to primary care providers and secondly, the length of time required to make the diagnosis. Because diagnosis of early RA is often difficult, the diagnostic lag time was found to be the major contributor to the overall delay in treatment. The median lag time to diagnosis in the study group was 18 weeks, with a shorter period for patients with progressive disease and seropositive for RF.
The rates of persistent disease reported in studies from EACs show the effectiveness of the early referral of patients to specialty arthritis clinics by primary care doctors and the selection and treatment of patients with progressive RA early in the disease. Van der Horst-Bruinsma et al compared patients with early RA (n=233) referred to an EAC with patients (n =241) from a routine outpatient clinic.35 The study assessed the lag time between the onset of symptoms and referral to a rheumatologist, as well as the consistency of the initial diagnosis after one year. The referral criteria for the early RA group were defined simply as patients presenting with at least two of the following features: joint pain, joint swelling, or reduction of joint mobility with a duration of less than two years.
The conclusions of this investigation provide a nice summary of the early referral initiative. The study concluded that in 70% of cases the diagnosis of definite RA, as defined by the 1987 ACR classification criteria, can be made by a rheumatologist within two weeks after the first visit, including atypical cases.35 The diagnosis was reliable and was rarely changed over the one year study period. The observation that erosions are often noted at presentation “justifies considerable effort to motivate both patients and primary care doctors to regard early RA as a medical emergency and thereby to reduce the lag time even more.”35
Recent evidence from an open, prospective, dynamic cohort study compared early DMARD treatment with delayed DMARD treatment for patients with recent onset RA (<2 years).36 The early treatment group had median disease duration of 130 days and the conventional treatment group 166 days. The conventional treatment group with an ACR diagnosis of probable or definite RA received NSAIDs at the point of inclusion in the study, and after ∼3 months the patients with active disease received hydroxychloroquine or sulfasalazine. Within two weeks of inclusion in the study, patients with definite and probable disease in the early treatment group were treated with either hydroxychloroquine or sulfasalazine, and the patients with less active RA were also treated with either hydroxychloroquine or sulfasalazine assigned at random.
Assessments included Health Assessment Questionnaire (HAQ) and radiographic joint damage, erythrocyte sedimentation rate (ESR) and CRP, morning stiffness, the number of swollen joints, and the Ritchie score. After only three months of treatment, the early treatment group showed significant reductions of ESR, CRP, and morning stiffness compared with the group receiving conventional treatment.36 Significant improvement in the duration of morning stiffness was sustained at one year with early treatment. Dramatic improvements were also shown by the Sharp score, which evaluates radiographic progression. After two years of treatment, the early treatment group had significantly less radiographic progression than the conventional treatment group, with no advancement of structural damage after the first year. Patient function, determined by the HAQ score showed clinically significant improvement at both one and two years. Conventional treatment showed a slight improvement in the HAQ score, which did not reach the clinically significant threshold.
The results of this study36 provide convincing evidence (III, C) of the crucial clinical benefit of early diagnosis and early DMARD treatment (>2 weeks after inclusion in the study) compared with conventional treatment. Early intervention resulted in a favourable outcome over the two years of the investigation; however, long term follow up is needed to confirm the distinct advantage of early DMARD treatment.
DURATION OF MORNING STIFFNESS
Morning stiffness, a common problem of patients with RA, affects quality of life and ability to function in the morning.37 The duration of morning stiffness correlates with disease activity11, 38, 39 and is a component of the revised American Rheumatism Association (ARA) criteria for RA.40 However, morning stiffness as a quantitative evaluation of disease activity or as an outcome assessment in clinical trial may have limited validity.24, 41–44
Regardless of the quantitative power of its duration, morning stiffness is a commonly recognised clinical characteristic of RA. Indeed, morning stiffness and fatigue are often the first symptoms.45 The duration of stiffness specific for RA as defined by the revised ARA criteria40 is at least 60 minutes and present for six weeks, whereas morning stiffness associated with non-inflammatory joint diseases almost always lasts for less than 30 minutes.46 In accord with this observation, the duration of morning stiffness in early RA may be ≥30 minutes (IV). An EAC study included a morning stiffness duration of >30 minutes as a predictor, among other indices, of active disease (Lard, unpublished data).36
EARLY REFERRAL RECOMMENDATION FOR EARLY RA
The graded clinical evidence provides clear support for the observations that: (a) permanent structural damage occurs early in the course of active RA,24, 39 and (b) early DMARD intervention slows the progression of structural joint damage11 and improves long term outcome, as well as overall patient quality of life.24 These points establish the need for a reliable and sensitive method of referral, enabling the rapid diagnosis of active RA and the subsequent initiation of DMARD treatment.
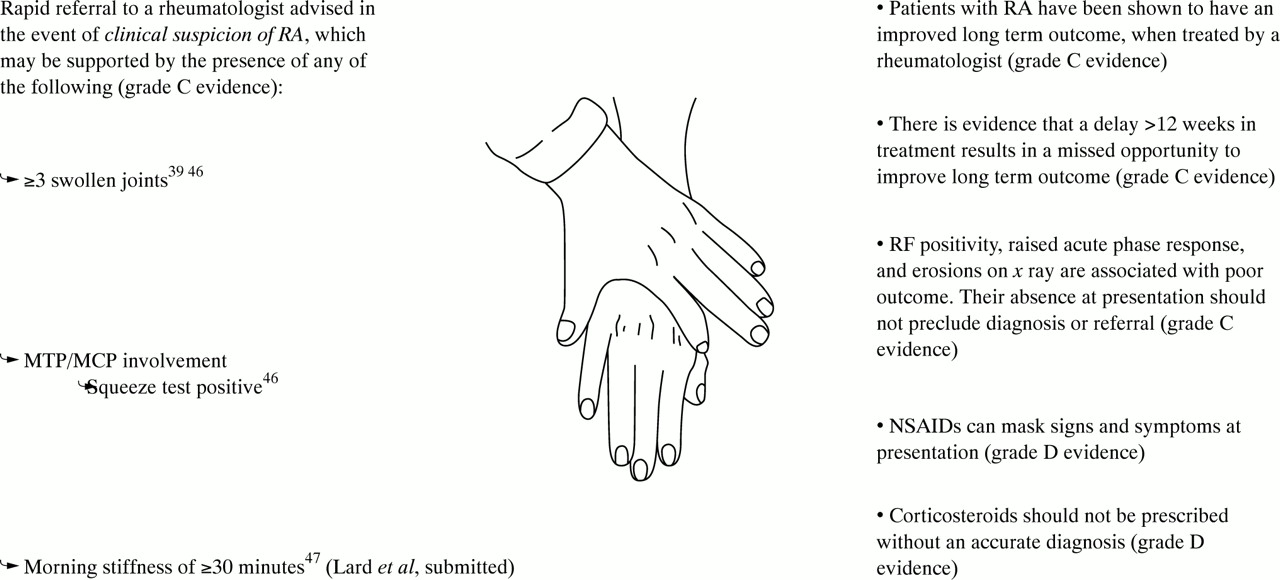
Figure 1 shows the referral recommendation and represents an evidence based tool summarising essential diagnostic criteria derived from prospective clinical investigations of prognostic factors, EACs, and the consensus of the expert panel. Referral is recommended when there is clinical suspicion of RA, with emphasis placed on suspicion, as delay induced by the desire for a confirming diagnosis often results in disease progression before effective treatment is started. This is supported by the observation that serological markers of RA are often negative during the early stages of RA.18 The evidence category supporting the referral tool is predominantly category III, and therefore the recommendation is given a grade C.

{kind=link}
Early referral algorithm for newly diagnosed RA.
The composite compression test or “squeeze” test (fig 1), is a useful technique for clinical evaluation of a group of small, adjacent joints such as the metacarpophalangeal and metatarsophalangeal joints, and the use of this diagnostic test in the assessment of early RA has been recently validated.47 Tenderness in a single joint within the group can be isolated by gentle palpation of the individual joints.48 Summing the number of tender joints in this manner allows the clinician to determine the number of affected joints. The number of affected joints chosen for this referral recommendation is based on the revised ARA criteria40 and recent results from an EAC in the Netherlands,47 which specify swelling of three or more joints.
The qualifying points included in the referral recommendation lend additional support to the criteria. There is clinical evidence (III) indicating that patients with RA tend to maintain functional ability and quality of life over the long term when their RA is managed by a rheumatologist compared with a non-specialist.24 Recent clinical evidence (Lard unpublished data)36 also shows that there may be only a brief opportunity during which early treatment may effectively stall the progression of RA.24
The compiled trials evaluating prognostic factors indicate that disease progression is likely when patients are RF positive and have raised levels of ESR and CRP24. However, because these factors are often negative in patients with active RA during the very early stages, their absence should not preclude referral.
NSAID use often obscures RA progression, significantly masking symptoms49 by reducing inflammation (III, D). Corticosteroids can also mask RA progression, and owing to their potential adverse effects, should not be given without a confirmed diagnosis of RA (IV, D).
CONCLUSION
The evidence based recommendation for early referral of patients presenting with early RA represents a valuable tool for the practising clinician, enabling the identification of the rheumatoid patient with potentially active disease. By recognising the patients who are likely to have persistent disease and by starting DMARD treatment early, the debilitating effects of RA can be reduced, and long term outcome and patient quality of life can be improved.