Article Text

Abstract
Objective: To analyse the treatment response to etanercept in patients with polyarticular course juvenile idiopathic arthritis (JIA).
Methods: 22 patients with polyarticular course JIA (19 females, three males; mean age 13.9 years; mean disease duration 6.3 years; 15 with polyarticular onset, seven with systemic onset, one with residual systemic activity; eight rheumatoid factor positive; eight with erosive disease) were treated with etanercept for up to 24 months. Etanercept was given subcutaneously at 0.4 mg/kg twice a week. Treatment response was ascertained in an open prospective study.
Results: All patients showed impressive clinical improvement, with a decrease in swollen joint count by an average of 10.1 joints (mean of 49% decrease), a decrease in tender joint count by 9.3 joints (mean of 94%), and decrease in total joint count by 11.2 joints (mean of 48%). Duration of morning stiffness decreased to less than 10 minutes. Furthermore, haemoglobin concentration increased on average by 14 g/l (mean of 15.3%) and packed cell volume increased by 0.035 (mean increase of 12%), and erythrocyte sedimentation rate decreased on average by 42.8 mm/1st h (mean decrease of 64%). No major side effects were noted.
Conclusion: Etanercept continues to be clinically effective and well tolerated in patients with polyarticular course JIA over a two year period.
- juvenile rheumatoid arthritis
- juvenile idiopathic arthritis
- tumour necrosis factorα
- etanercept
- ANA, antinuclear antibody
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- JIA, juvenile idiopathic arthritis
- NSAID, non-steroidal anti-inflammatory drug
- RF, rheumatoid factor
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- ANA, antinuclear antibody
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- JIA, juvenile idiopathic arthritis
- NSAID, non-steroidal anti-inflammatory drug
- RF, rheumatoid factor
- TNF, tumour necrosis factor
Biological response modification directed against inflammatory cytokines has become a fascinating option in the treatment of patients with polyarticular course juvenile idiopathic arthritis (JIA).1–3 Tumour necrosis factor (TNF) blockade in particular is a highly targeted therapeutic intervention as it plays a central role in the pathogenesis of JIA.4,5 TNFα is largely responsible for the degree of synovial inflammation.6–9 It causes proliferation of synoviocytes and production of other proinflammatory cytokines such as interleukin 1, 6, and 8, and granulocyte-macrophage colony stimulating factor10; TNFα also induces production of metalloproteinases, such as collagenase and stromelysin, and prostaglandins, and increases expression of adhesion molecules. It also leads to upregulation of the transcription factor NF-κB, and induces apoptosis.6,7
The two TNF receptors p55 and p75 occur both membrane bound and in a soluble form. The soluble TNF receptor can neutralise TNF activity.11 Etanercept has been developed to achieve therapeutic application of the TNF blockade. It is a dimeric fusion protein consisting of the extracellular portion of the human p75 TNF receptor linked to the Fc portion of human IgG1.12
Etanercept has been shown to be safe and effective in the treatment of patients with rheumatoid arthritis13–15 and JIA.1–3 Lovell et al1 first reported on the safety and efficacy of treatment of polyarticular course JIA with etanercept. We subsequently reported on 10 patients with JIA treated for one year with etanercept.3 Over the last 24 months, we have treated with etanercept 22 patients with polyarticular course JIA, and here report our results.
PATIENTS AND METHODS
Twenty two patients were included in this open prospective observational study (table 1). Nineteen were females and three were males, with current ages of 5–32 years. Ages at onset of JIA were 10 months to 15.5 years, with a mean of 7.1 years. The duration of JIA was one to 18 years (mean 6.8 years). Baseline clinical assessment and laboratory evaluation were performed before treatment initiation. Clinical examination at screening included swollen joint counts (10–46, mean 22), tender joint counts (1–25, mean 10.1), and total joint counts (10–49, mean 24). Morning stiffness consistently lasted for more than two hours in all patients. All patients had active polyarthritis, and one girl had mild residual systemic features of systemic onset JIA in addition to polyarthritis. Limiting fatigue was a consistent complaint in all patients.
Patients with juvenile idiopathic arthritis treated with etanercept
The baseline laboratory data showed various degrees of anaemia, with haemoglobin levels of 72–123 g/l (mean 100 g/l), packed cell volume of 0.25–0.37 (mean 0.31), and erythrocyte sedimentation rates (ESRs) (modified Westergren method) of 17–140 mm/1st h (mean 60.55 mm/1st h). Ten patients had a positive antinuclear antibody (ANA) profile (with a negative ANA profile), and eight had a positive rheumatoid factor (RF) profile. On radiographic imaging, eight had erosive changes, and periarticular osteopenia was present in most patients. Two patients with a severe longstanding systemic course had developed avascular necrosis of the hip as a complication of steroid treatment requiring total joint replacement.
The treatment regimens showed that 21 of 22 patients were receiving methotrexate (18 orally and three subcutaneously; at least 10–15 mg/m2 body surface area). Duration of methotrexate treatment ranged from six months to 16 years. It was maintained at the same dose during treatment with etanercept. All patients were receiving full anti-inflammatory doses of non-steroidal anti-inflammatory agents (NSAIDs) including naproxen at 15–20 mg/kg, tolmetin sodium 20–30 mg/kg, ibuprofen 30–40 mg/kg, sulindac 4–6 mg/kg, nabumetone 20–30 mg/kg, or fenoprofen 40–50 mg/kg. Thirteen patients were receiving hydroxychloroquine at 5–7 mg/kg, one was receiving sulfasalazine (in addition to methotrexate), five were receiving low dose systemic corticosteroids, and nine additional patients had previously been receiving corticosteroids. All patients were receiving folic acid only in the case of clinical side effects of methotrexate. Recognising the unsatisfactory response to the conventional regimens outlined above, we decided to add etanercept, administered subcutaneously twice a week at a dose of 0.4 mg/kg. In one 5 year old girl with recent onset polyarticular JIA, etanercept was introduced as the initial disease modifying antirheumatic drug (DMARD) without concomitant methotrexate. The patients were seen at a follow up clinic. Evaluation included a detailed history, especially of the joints, and constitutional symptomatology and functional impairment. Joints were examined by the same clinicians. Laboratory monitoring included complete blood count, ESR, liver function tests, creatinine, electrolytes, and a urine analysis.
RESULTS
The mean duration of treatment with etanercept in our patient group is now 16.7 months (range 4–26). The median is now 21 months, with eight patients having been treated for 24 months or longer.
Evaluation of our patients at clinical follow up showed an impressive response to etanercept treatment. The swollen joint count decreased on average by 10.1 joints (range 1–19) from 22 to 11.9, with a mean individual percentage decline in swollen joints of 49%. The tender joint count decreased on average by 9.26 (range 1–24) from 10.1 to 0.84, with a mean percentage decline in tender joints of 94% (fig 1). Patients are depicted in figs 1 and 2 according to disease severity before treatment with etanercept; individual positions therefore do not refer to the identical patient. The total joint count decreased on average by 11.2 joints (range 1–22) from 24 to 12.8, with a mean percentage decline of 48.1%.
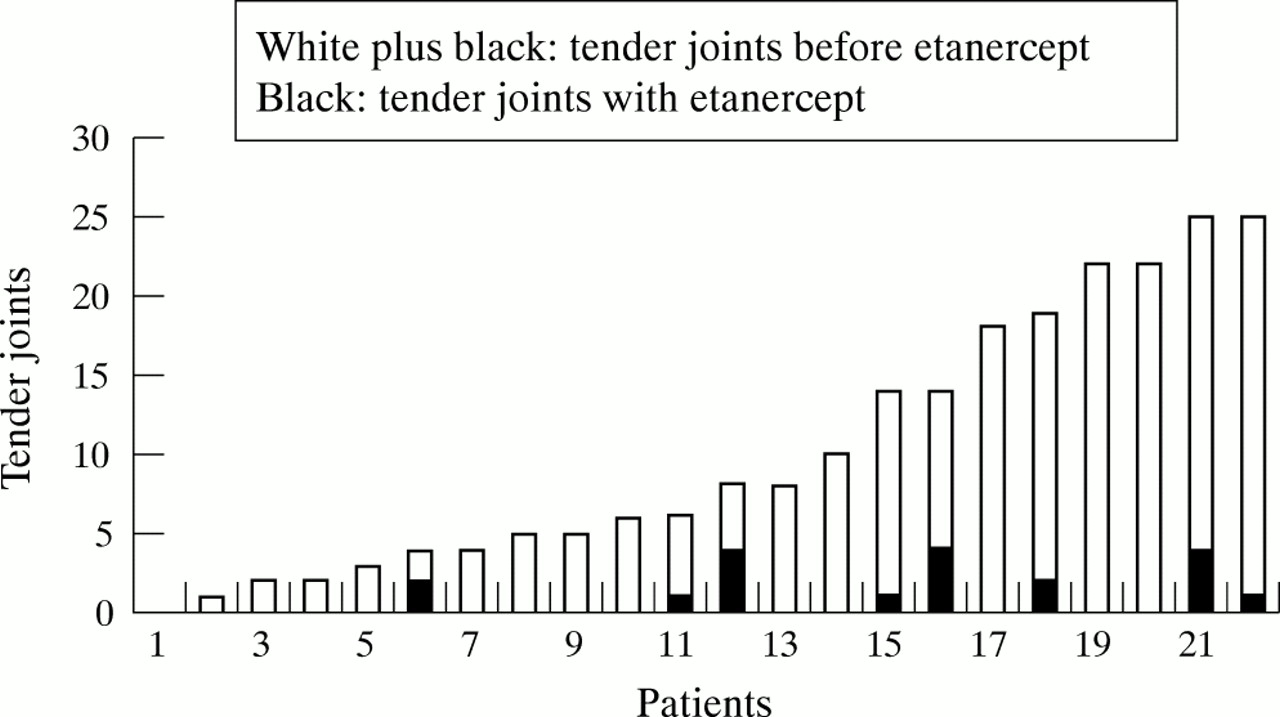
Decrease in tender joint count in patients with polyarticular course juvenile idiopathic arthritis treated with etanercept.

{kind=link}
{kind=link}
Decrease in erythrocyte sedimentation rate (ESR) in patients with polyarticular course juvenile idiopathic arthritis treated with etanercept.
The duration of morning stiffness consistently decreased to less than 10 minutes or was absent. Patients also reported dramatic improvement in symptoms of fatigue. Improved control of joint symptoms and increased energy levels enabled many patients to resume academic and leisure activities that they had stopped because of their active disease.
In the 5 year old girl with systemic onset JIA, not only the joint symptoms but also the systemic features (fevers and rashes) were resolved, and she is successfully being weaned off corticosteroids. In two further patients, corticosteroid doses could be decreased, and three patients discontinued steroid treatment all together. Four patients no longer required NSAIDs. One female adolescent patient with seropositive polyarticular JIA tried to reduce the etanercept injections to once a week, but developed inflammatory activity with new joint swelling and morning stiffness and a corresponding increase in ESR.
The laboratory evaluation showed that anaemia improved, with an average increase in haemoglobin of 14 g/l (range −11 to +53) from 100–114 g/l, with a mean individual percentage increase of 15.29%. Packed cell volume increased on average by 0.035 (range −0.041 to +0.13) from 0.31 to 0.34, with a mean percentage increase of 12%. The ESR decreased on average by 42 mm/1st h (range 2–124) from 60.55 to 18.55 mm/1st h (fig 2), with a mean percentage decline of 64%.
All patients tolerated the etanercept injections well. Minor reactions did occur at the injection site but did not require discontinuation of the treatment. No severe infections were observed.
DISCUSSION
Our treatment options for severe polyarticular course JIA have been greatly expanded by the availability of drugs that specifically target inflammatory cytokines. TNFα blockade has introduced a new dimension to our treatment concept. Whereas in the past we had to be satisfied with symptomatic improvement relying on conventional treatments including NSAIDs, DMARDs such as methotrexate and sulfasalazine, antimalarial drugs, and intra-articular and low dose systemic corticosteroids, we may now realistically hope for a greater clinical response, prevention of erosions, and actual arrest of the disease. There have been early encouraging reports of convincing responses in adults with rheumatoid arthritis13–15 and children with JIA,1,3 which have given rise to enthusiasm for this treatment.
Some concerns and open questions remain with regard to TNFα blockade. Will the response last over a longer period and will there be long term side effects or complications, particularly autoimmune processes or malignancies? The cost of TNFα blocking agents has led to concerns about the economic burden and insurance coverage.
We report our observations on 22 patients with polyarticular course JIA treated with etanercept over a two year period. Our patient group was heterogeneous with regard to age and disease duration. All patients had severe disease with uncontrolled inflammatory activity plus various degrees of chronic impairment. Etanercept was added to the pre-existing therapeutic regimen, which in almost all patients consisted of DMARDs such as methotrexate and hydroxychloroquine and an NSAID.
We have been very impressed with the clinical response with regard to both the decrease in joint symptomatology and resolution of constitutional features such as fatigue and malaise. The improvement in joint symptoms, particularly the dramatic decrease in joint pain, has enabled the patients to increase physiotherapy exercises for muscle strengthening and conditioning. We have consistently gained the impression that etanercept has had a more positive effect on the patients' lives than any previous treatments. It seems to have alleviated the subjective sense of illness, producing a happier, more active, productive, and integrated life. The positive response to treatment continued over the whole observation period. We noted no intolerance, side effects (except mild injection site reactions), or features suggestive of a developing connective tissue disease. We have been able to decrease or stop systemic corticosteroids in most cases, and some patients no longer require NSAIDs. We did not attempt to reduce the dose of methotrexate or etanercept after control of active joint symptoms was achieved. One girl with systemic onset JIA who still had systemic activity at the time etanercept treatment was started, now has excellent control of articular symptoms and is free of fevers and rashes. This may have been the “natural course” of the systemic phase in her case rather than a response to etanercept, but she had not responded previously to standard treatment. In parallel with the clinical improvement, dramatic declines in ESR and moderate improvement in anaemia were observed. Ten of the patients were ANA test and positive with a negative ANA profile before treatment with etanercept. None developed any symptoms of a connective tissue disease or autoimmune process during treatment. We are planning to re-evaluate the patients serologically with an ANA test and ANA profile. We have also found no infectious complications that could be attributed to TNFα blockade.
In conclusion, this observational study of 22 patients with severe polyarticular course JIA shows very convincing evidence of the continuing safety and efficacy of etanercept over a two year period.