Article Text

Abstract
OBJECTIVE To evaluate ultrasonographic methods, including the Doppler technique, as measures of synovial inflammation in finger joints of patients with rheumatoid arthritis.
METHODS Ultrasonography was performed with a high frequency transducer (13 MHz).
Evaluation of the sonographic data was conducted by two independent observers and included measurement of synovial area and thickness (grey tone ultrasound), vascularisation (power/colour Doppler), and indices of the intra- and extrasynovial arterial flow (spectral Doppler). The flow pattern was estimated by the indices of pulsatility (PI) and resistance (RI).
RESULTS The sonographic measurements of joint space were reproducible with intraobserver, intraclass correlation coefficients (ICC) 0.82–0.97 (p<0.0001) and interobserver ICC 0.81 (p<0.0001). The mean (SD) fraction of the synovium vascularised in the patients was 0.15 (0.15). The synovial blood flow was characterised by a diastolic flow—that is, the flow persisting during the diastole. The mean (SD) PI was 1.92 (1.18) and RI 0.70 (0.13). The estimated vascular fraction correlated with the erythrocyte sedimentation rate (ESR) (r s=0.53, p=0.03). The relative Pi (rPi), an estimate of an abnormally low resistance to vascularisation, correlated with both ESR (r s=−0.557, p<0.05) and Health Assessment Questionnaire score (r s=−0.584, p<0.05). After an injection of contrast Levovist the vascular fraction increased, while no difference in PI and RI was observed.
CONCLUSION Ultrasonography is a reliable tool for estimating the size of the joint space and the synovial activity measured by the degree of vascularisation and pattern of flow. Ultrasonography may be useful in monitoring the synovial inflammation in rheumatoid arthritis.
- Doppler ultrasonography
- rheumatoid arthritis
- inflammation
Statistics from Altmetric.com
To monitor treatment in rheumatoid arthritis (RA) a precise measure of the disease activity should be obtained by both clinical and paraclinical parameters.1
The disease activity of a joint is correlated with the synovial vascularisation,2 ,3 which can be estimated by magnetic resonance imaging (MRI) measurement of synovial membrane volumes after intravenous gadolinium injection. This examination is relatively expensive and time consuming. It would be of advantage for both patient and therapist if a similar estimate could be obtained by ultrasonography directly in the outpatients' clinic.
Ultrasonography has proved to be valuable in the morphological and structural assessment of soft tissue in patients with arthritis.4 With modern high quality sonographic equipment, colour/power Doppler can be used to determine the flow even in small blood vessels. This, again, may give an estimate of the presence and extent of inflammation.5 ,6
The purpose of this study was to evaluate the sonographic technique, including the Doppler technique, as a supplement to the clinical evaluation of synovitis in RA.
Moreover, the value of ultrasound contrast media was tested in the quantification of vascularisation of the synovial membrane in patients with RA.
Patients and methods
A total of 18 patients with RA according to the American College of Rheumatology criteria agreed to participate in the study. Their mean age was 60 years (range 30–78) and mean duration of RA 7.6 years (range 2–10). The patients were receiving stable treatment with a disease modifying antirheumatic drug or Enbrel in the three months before the investigation, and during this period the patients had had no injections of glucocorticosteroids.
The patients were evaluated clinically with the Health Assessment Questionnaire (HAQ) score, number of tender and swollen joints, and blood tests were drawn for measurement of erythrocyte sedimentation rate (ESR) and C reactive protein (CRP).
ULTRASONOGRAPHY
The patients were scanned with an Acuson Sequoia (Mountainview, California, USA) using a near-focused transducer with a centre frequency of 13 MHz.
Scanning was run on the joint perceived by the patient as being the most inflamed, either the metacarpophalangeal, proximal interphalangeal, or the wrist joint. In this joint the synovial membrane was visualised and maximal area and thickness were determined in two dimensions. The blood flow in the region was visualised by colour Doppler and an image with maximal colour activity was selected for analysis.
With the aid of spectral Doppler the quality of flow was determined (fig 1) and the indices of pulsatility (PI) and resistance (RI) were measured in three arteries within the synovial membrane and in a neighbouring muscle as control. PI was defined as (maximum systolic velocity − end diastolic velocity)/maximum velocity. To characterise the relation between flow inside and outside the joint, the ratio between indices was calculated: rPI=PIs/PIx and rRI=RIs/RIx. Both PI and RI correlate with an increased peripheral resistance, indicating a decrease in perfusion of the tissue.7 ,8
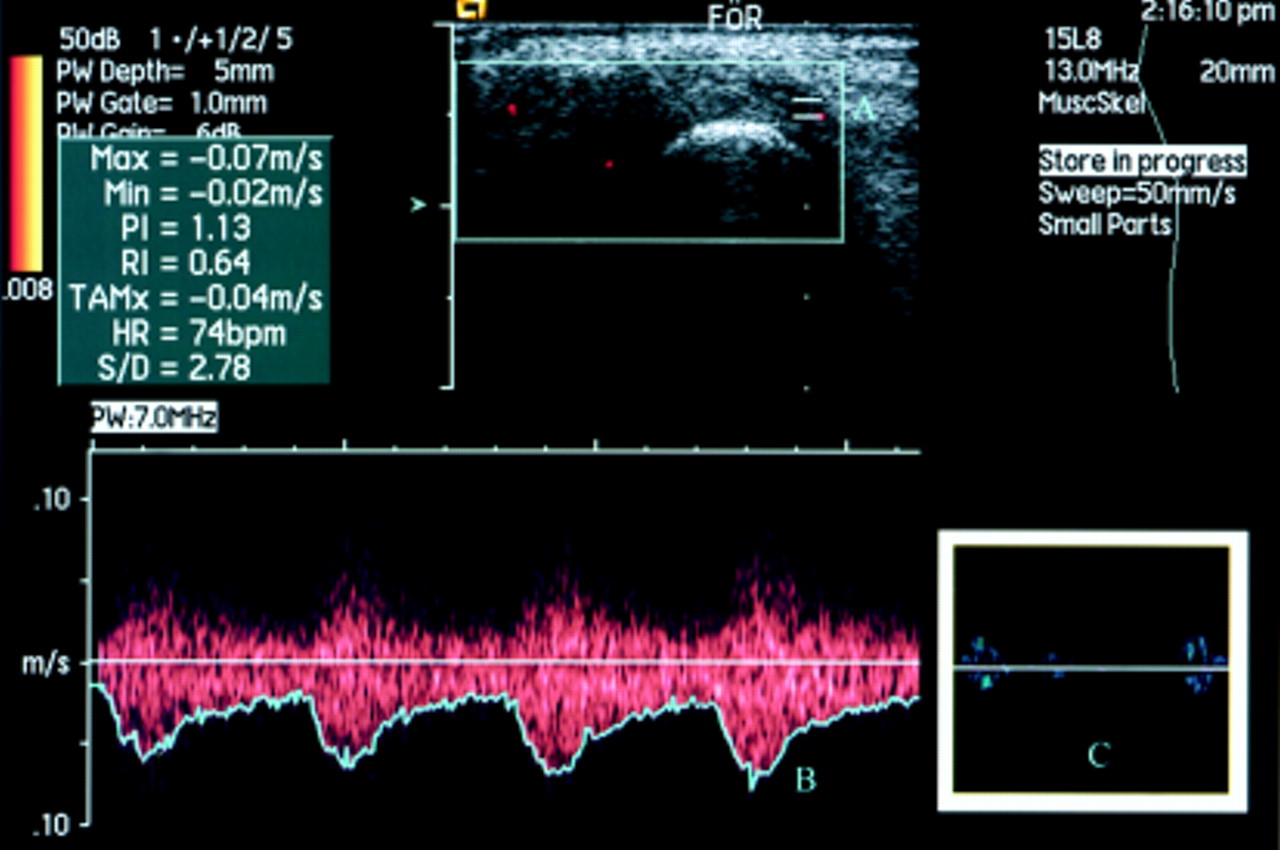
Analysis of the flow pattern with spectral Doppler utility. A = vessel chosen for the analysis; B = blood velocity. Note the persistent flow in the diastole. Pulsatility (PI) and resistance (RI) are calculated automatically by the program. C = an example of normal musculoskeletal flow. Note the absence of diastolic flow.
An intravenous injection of ultrasound contrast agent (Levovist, Schering) was given and synovial flow was monitored with unchanged colour Doppler settings until maximum effect was judged to be present (fig 2A). An image was selected for analysis and spectral Doppler measurements were repeated.


{kind=link}
{kind=link}
{kind=link}
(A) Longitudinal scan of two metacarpophalangeal joints after injection of contrast (Levovist). (B) All coloured fields are replaced with a monochrome colour (white). Using a histogram facility, it is possible to assess the area of the outlined synovial membrane and blood vessels within the limits chosen.
DATA EVALUATION
The quantitative estimation of the vascularisation in the synovial membrane was performed in the following way: the digitally stored UL pictures were read with a DICOM-compatible program. The unchanged pictures were then transferred to a processing program (Corel photo-paint 7).
All the coloured pixels on the Doppler sonographic picture correspond to motion. When noise has been reduced to a minimum they may be interpreted as blood flow (fig 2A). The colour recognition function was used to change all marked pixels to a reference colour. The total number of pixels was finally depicted using a colour histogram (fig2B).
Clinical evaluation included the HAQ, pain on a 100 mm visual analogue scale, the doctor's global assessment, and patient's global assessment. Global inflammatory activity was assessed by ESR and CRP.
The examiner was unaware of the clinical status and treatment of the patients.
STATISTICS
Non-parametric statistical methods were applied with a level of significance of 0.05.
OBSERVER VARIATION
The data processing was performed by two independent investigators evaluating the randomly numbered pictures. They were unaware of the name of the patient, the time of investigation, and the treatment given. The procedure was repeated after one month by the two investigators using the same pictures.
Results
ULTRASONOGRAPHIC EVALUATION
In most cases the synovial membrane could clearly be depicted from the surrounding tissue by the sonographic examination. It was subsequently possible with the aid of power Doppler to choose arteries both intrasynovially and extrasynovially for measurement by spectral Doppler. Joint effusion was rarely seen and the amount of fluid in these cases was of no importance for the area measurements.
The profile of the arteries measured with spectral Doppler was qualitatively determined to be from areas with a low vascular resistance—that is, with a persistent flow present during the diastole. The ESR correlated with the vascularisation of the synovial membrane, both when measured as a vascular fraction (n=16,r s=0.53, p=0.03) and as a vascular pixel area (n=16,r s=0.48, p=0.05). No other correlations were found between the clinical data and synovial or vascular pixel areas (table 1).
Correlation between the vascular fraction at baseline measured by investigator 1 and the variable listed below
The ratio indices rPi also correlated with the ESR (n=13,r s=−0.557, p=0.048) and HAQ (n=13, r s=−0.584, p=0.036).
After the intravenous injection of contrast there was an increase in vessels depicted by the power Doppler. However, no further significant changes in rPI and rRI were found.
RELIABILITY
The two investigators measured the pixel area of the synovial vessels twice. The intraclass correlation coefficient (ICC) of 74 evaluable double measurements was for investigator 1, 0.97 (p<0.0001) and for investigator 2, 0.82 (p<0.0001).
Intertester reliability was tested in the first evaluation of the pictures and the ICC between investigators 1 and 2 was 0.81 (n=75, p<0.0001).
Discussion
This study showed a consistent and reproducible delineation of the inflamed synovial membrane in the small joints of the hands or fingers of patients with active RA. The grey tone ultrasonographic pictures gives an overview of the amount of swelling of the tissue around the joints. However, in our study this was not related to clinical data. This observation is in accordance with other studies, which have found a lack of correlation between clinical parameters and similar determinations of synovial area and volume by ultrasound and MRI.3 ,9 An explanation for this apparent inconsistency may be the varying amount of fibrous tissue in the synovial membrane. In almost all patients an abnormal presence of arteries could be demonstrated by colour Doppler, and by measuring the area of these arteries, an estimate could be obtained of the perfused part of the synovial membrane corresponding to the activity of the RA in the joint. By the same argument, areas without signs of vascularisation may represent dormant synovium or fibrous tissue from previous healed attacks of synovitis. It must be realised, however, that the ultrasonographic measurement is only representative of the perfusion at the precise moment and variations during the day should be clarified in future studies.
Our method of determining colour pixels through a simple picture-handling program allowed a quantitative analysis of the degree of vascularisation, and the clinical relevance was indicated by the correlation with the ESR. It remains to be seen whether this quantitative measure offers a better way of monitoring the outcome of treatment than the semiquantitative tests proposed in former studies.10 ,11 In our patients, and in accordance with other studies, several erosions were seen that were non-discernible, or barely discernible, on conventional radiography. However, there was no indication of specific areas of the synovium being vascularised more often than others, and we found no preponderance of blood flow near the erosions of the joints.
The synovial perfusion was not only abnormal owing to its increased number of arteries, as evidenced by the colour Doppler, and when spectral Doppler was used the arterial perfusion of the tissue showed persistent flow during the diastole. The flow curve of the vessels in the rheumatoid synovial membrane may be altered by the inflammation; the diastolic perfusion, in particular, being unusual in resting musculoskeletal tissue. A high diastolic flow is normal in, for example, renal, cerebral, and umbilical arteries, where a low peripheral resistance assures a permanent and high perfusion. In other parts of the body resting tissue has a high peripheral resistance and a deviation from this indicates inflammation, malignancy, or arteriovenous malformations.7 Also, measurements of the pulsatility and resistance indices are used to characterise perfusion. In our study calculation of the indices was based on extrasynovial control arteries in the tissue immediately surrounding the joint. These arteries might have been affected by the presence of inflammatory tissue nearby, and for future, more sophisticated calculations muscle tissue distal from the joint should be chosen for the purpose of comparison with the synovial vessels .
It may be noted that the disclosure of small synovial arteries for such measurements requires highly sensitive sonographic equipment. The use of ultrasound contrast agents may increase sensitivity in the event of diminished synovial vascularisation and may also be of value in situations involving the use of suboptimal equipment.
In comparison with MRI, ultrasonography has the advantage of being more readily accessible and far cheaper. In the not too distant future sonographic equipment may be available in many rheumatology departments. Teaching simple procedures, such as estimating local signs of inflammation or finding minor effusions in the joint, will be simplified, thus pointing to yet another application for ultrasonography in the daily clinic.
During the editorial evaluation of this article an observation of Doppler ultrasonography in Raynaud's syndrome has been published.12 In that article a specific computer program was employed for the detection of colour pixels in the region of interest. However, as shown above, an ordinary colour program may be used with reproducible results.
Acknowledgments
We thank Acuson for the loan of the Sequoia ultrasonographic equipment and Schering for the donation of half of the Levovist used in this study.
References
Supplementary materials
Click on the blue hyperlinks to view the image. To return to this page press 'Back' on your browser.
Longitudinal and transversal scan of the left second metacarpophalangeal (MCP) joint of a patient with R.A..
The circumference of the synovial membrane is marked on a 2D mode picture, and the area is instantly calculated by the computer
Longitudinal scan of 2 MCP before injection of contrast. Within the Doppler frame box, blood flow is visualised as colored areas by Color-Doppler technique.
Vascular activity in the synovial membrane is clearly shown here.
Correlation between vascular fraction in the synovial membrane and ESR a/ investigator 1 , b/ investigator 2
Injection of U.S. contrast increases the ratio of colored pixels in a significant way.
P = 0.004 using Wilcoxon signed rank test
Graphical visualization of intraclass variation. Results from examination 1 are arranged in increasing numbers. Results from examination 2 are matched for each picture of the patient.
ICC investigator1 = 0.97 (p< 0.0001). ICC investigator 2 = 0.82 (p< 0.0001)
Graphical visualization of interclass variation. Results from investigator 1 are arranged in increasing numbers. Results from investigator2 are matched for each picture of the patient.
ICC = 0.81 (p< 0.0001)
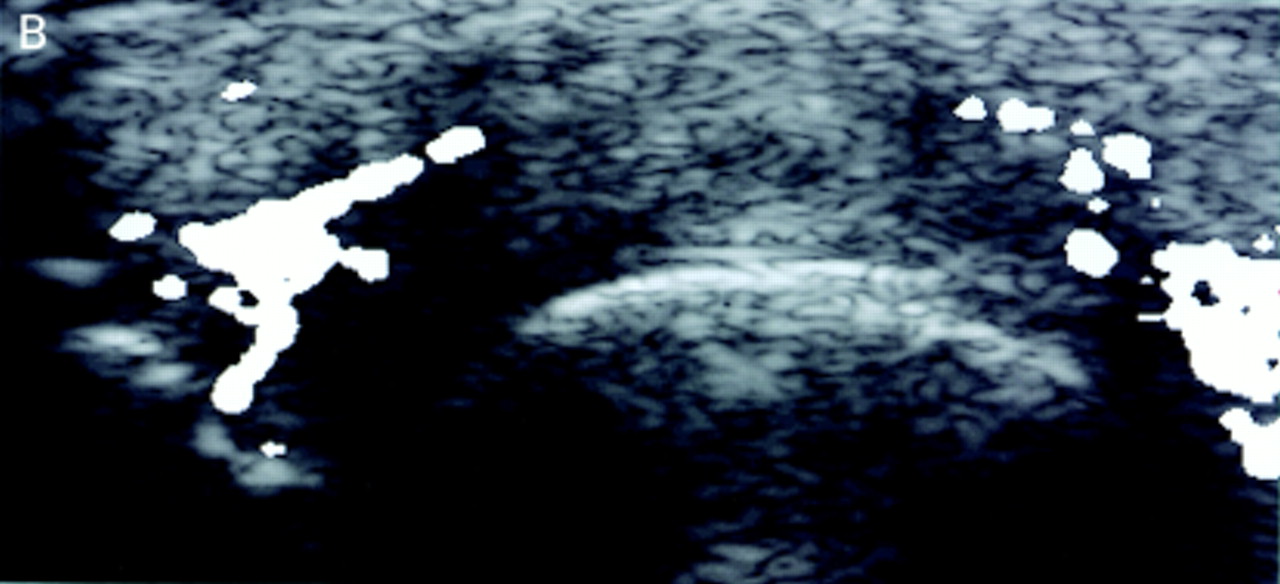
Bilateral longitudinal scan of caput ulnae on patient with R.A (top).
X-ray of left wrist (bottom).
Erosion on the left caput ulnae is seen by ultrasonography. Note the smooth unbroken surface on the contralateral caput ulnae. No erosion was described by the radiologist.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
Additional Doppler images appear on the Annals web site at www.annrheumdis.com
The study was supported by the Oak Foundation.