Article Text

Abstract
Studies of disease outcomes have not produced an explanation or an intervention for the symptoms and complaints that some women have attributed to breast implants. Reviews of the literature have found no increased risk of specific systemic disease, and no treatment recommendations have emerged. However, similar symptoms in fibromyalgia, chronic fatigue, and other contexts have been considered to be stress or behaviourally mediated, and a number of promising behavioural interventions have been developed. Aetiological, research, and treatment implications may follow from the consideration of such symptoms within a behavioural medicine model that allows for the interaction of physical and psychological influences. In the case of implants, a mass somatisation model may also help to discern the potential effects of litigation and other social influences.
- silicone
- breast implants
- somatisation
Statistics from Altmetric.com
Since the beginning of the breast implant controversy, a host of symptoms have been attributed to implants. Concerns have included (a) systemic diseases and conditions such as cancer or connective tissue disease, (b) non-specific complaints such as fatigue and pain, and (c) local complications such as capsular contracture, rupture, or infection. It has not been disputed that local complications can occur. However, systematic studies have found no consistent risk of systemic disease associated with implants (see example studies and reviews1-8). Some women with breast implants have systemic diseases, but epidemiological research suggests that the same proportion of women without implants have these diseases. This conclusion has been supported by summary comments of the American Academy of Neurology,9 the Institute of Medicine,10 and an expert panel convened by United States Judge Pointer.11
None the less, many women continue to complain of symptoms that they attribute to implants. Reviews of symptom complaints are scarce. Most epidemiological studies have focused only on systemic disease outcomes, providing limited published information on individual symptoms or complaints. The symptoms investigated have varied widely with the type of disease studied and method of study. Tugwell's review12 is especially helpful, as it examined symptom complaints from studies of women with implants who did not meet the criteria for specific connective tissue diseases. It also summarised symptoms from anecdotal case reports. Table 1 shows that a wide range of complaints have been reported by women with implants, though no consistent differences between women with implants and controls have been found.
Symptoms reported by women with implants in Tugwell's review12
Overlap of non-specific symptoms
Several researchers have noted that complaints of women with breast implants appear to overlap with a pool of symptoms common among disorders, such as fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome.13-15 Barsky and Borus postulated that side effects attributed to breast implants are one of several related functional somatic syndromes characterised by symptom amplification, suffering, and disability in the absence of, or disproportionate to, demonstrable tissue abnormalities.13 They propose that this spectrum of syndromes includes sick building syndrome, repetitive stress injury, Gulf War syndrome, and chronic whiplash. Similarly, Winfield suggested that most women with breast implants complaining of silicone induced atypical connective tissue disease actually have fibromyalgia and that fibromyalgia is not a disease, but part of a spectrum of related conditions with similar aetiologies and pathologies.14
It is instructive to compare the symptoms of fibromyalgia, for example, with the complaints commonly identified by women with implants noted in table 1. Widespread pain, multiple tender points in specified locations around the body, persistent sleep disturbance, and fatigue are also considered central to the diagnosis of fibromyalgia.16Many other symptoms may be associated—for example, allodynia, hyperalgesia, subjective weakness, dysaesthesias, paraesthesias, complaints of memory and concentration problems, auditory, vestibular, and ocular complaints, chronic rhinitis, complaints of allergies, heart palpitations, superimposed regional pain syndromes, such as headache, atypical chest pain, pelvic pain, dyspareunia, temporal mandibular disorder, or myofascial pain, irritable bowel symptoms, subjective joint swelling,14 Raynaud's phenomenon, premenstrual tension, irritable bladder, migraine headaches,17 and symptom aggravation by stress.18 Considerable overlap with table 1 is apparent.
Behavioural medicine and somatisation
In this spectrum of disorders with overlapping symptoms and no specific known cause psychological contributions are often suggested and behaviourally based symptomatic treatments commonly applied.1 ,19 However, until recently, psychological models have received little attention in conceptualisation of the complaints reported by women with breast implants. The present hypothesis is that somatisation may be an important factor in understanding and treating a portion of the complaints reported by individual women with implants. Mass somatisation, in turn, may further explain the social phenomenon of large numbers of people reporting similar symptomatic shifts and changes in tandem with public events, mass media coverage, mass litigation, and public policy changes.
Somatisation is a common term but one used in varied ways. It has often implied that symptoms are psychological or imaginary rather than physical and real. The present view of somatisation refers to:
Psychological initiation of actual physical symptoms or dysfunction
Psychological intensification of actual physical symptoms
Psychological magnification or perception of benign sensory phenomena as distressing or symptomatic
Reattributions of the cause and meaning of physical and psychological symptoms
Altered response to physical symptoms at an emotional, social, behavioural, and cognitive level
Reciprocal interactions of all of the above.
This assumes that one may affect many physical symptoms and sensations through stress, classical conditioning, operant conditioning, and other cognitive and behavioural mechanisms. In this broader sense it is likely that all people experience some elements of somatisation.
Drawing heavily upon the integrative model of Kirmayer and Taillefer,20 there appear to be eight primary facets of the somatisation process, all of which may occur simultaneously and interactively.
BASELINE
The individual begins with a pool of various sensory input and perceptual interpretations at various levels of subclinical intensity, as well as specific medical symptoms and diffuse or unexplained medical symptoms. Raised baselines of diffuse or vague symptoms or sensory phenomena may represent an initial risk factor for somatisation.
BASELINE CHANGE
Emotional arousal, psychological disturbance, medical illness, stress, psychiatric disorder, or other factors may change baseline response by increasing symptoms, changes in thresholds, hypersensitivity to sensory phenomena, hypervigilance, or other changes in the physiology itself. A common end point is increased attention to bodily sensations. As focused attention alters the signal to noise ratio in sensory phenomena, the result may be an actual increase in the perceived intensity of various sensory inputs.
ATTRIBUTION
The perceived meaning of symptoms and any changes in physiology, sensation, or perception are critical. Most often with somatisation there is an attribution of sensations and changes to disease or illness. Other cognitive variables may play a part in this initial attribution process, such as predictability of and perceived control over threat.
INTERNAL MEDIATION
Individual coping responses further shape the response to sensory phenomena and symptoms. People inclined more toward worry, catastrophising, depression, or demoralisation may have more adverse responses. Those with a history of somatoform disorders may be at higher risk. Comorbid maladaptive personality characteristics, personality disorders, or other specific disorders, such as post-traumatic stress disorder, may pose added risk.
SOCIAL MEDIATION
The social context has an important role, including the response of family, healthcare providers, employers, litigation environments, the media, and the insurance or compensation system. In the case of implants, individual and social aspects of cosmetic surgery and body image may be particularly relevant.21
WIND UP
Somatisation is prone to feedback loops, where responses in any one facet of this cycle may fuel changes in others. For example, stress may cause new physical symptoms or intensify existing ones. Increased symptoms, in turn, add more stress and increased wariness of normal physical sensations, affecting the judgment of normal versus abnormal sensory input.
CONSOLIDATION
Although normal somatisation phenomena are likely to be transient, those that lead to illness, suffering, and disability become entrenched. An array of consolidating factors may be important in this entrenchment process: (a) There may be contingencies that interfere with resolution, such as litigation, other counterincentives, or face saving issues. For example, people who have become convinced that their suffering and symptoms are due to a certain medical cause may be reluctant to reconsider these as attributable to their own coping skills and response to stress. (b) The reciprocal influences of wind up may perpetuate the process and reinforce sustained hypersensitivity or hypervigilance. For instance, Okifuji and Turk have suggested that patients with fibromyalgia develop a generalised hypervigilance that promotes generalised somatic symptoms as well as related elements such as doctor shopping, inconclusive diagnostic results, increased emotional distress, symptom magnification, feelings of hopelessness, change in social dynamics, and abnormal illness behaviours.19 (c) Help seeking responses and coping skills are likely to be pertinent. Changes may begin to develop over time in one's basic approach to the problem. Avoidance of cognitive dissonance may lead individual subjects to disregard alternative explanations. Once disease conviction reaches a certain level, reassurance becomes more difficult or paradoxical. For example, it has been suggested that participation in support groups and access to inflammatory patient information may make non-specific complaints worse.22
ADAPTATION AND TERTIARY IMPACT
Some people are inclined towards problem solving and others towards adaptive coping styles, which probably helps them to move forward and away from the cycle of somatisation and entrenchment. Others may be more vulnerable to progressive disability or persistent suffering and disease preoccupation. Persistent somatisation may actually alter physical symptoms and create new medical problems—for example, the immobilisation and progressive physical decline characteristic of patients with long term chronic pain.
Mass somatisation
Jones, Craig, and colleagues define mass psychogenic illness as widespread subjective symptoms attributed to presumed toxic exposure in the absence of objective evidence of a specific cause.23As we have suggested with somatisation generally, Wessely has noted that mass psychosomatic symptoms “Are physiologic experiences that are based on identifiable physiologic processes that cause pain and suffering” (p 129), with the potential to develop into long term chronic illness.24 Winfield suggested that complaints associated with implants, as well as disorders such as fibromyalgia, chronic fatigue syndrome, sick building syndrome, and multiple chemical sensitivity syndromes, are at least partly attributable to social and attributional factors commonly associated with mass somatisation, such as media attention, hype, suggestible fears, and the effects of product liability and litigation.14
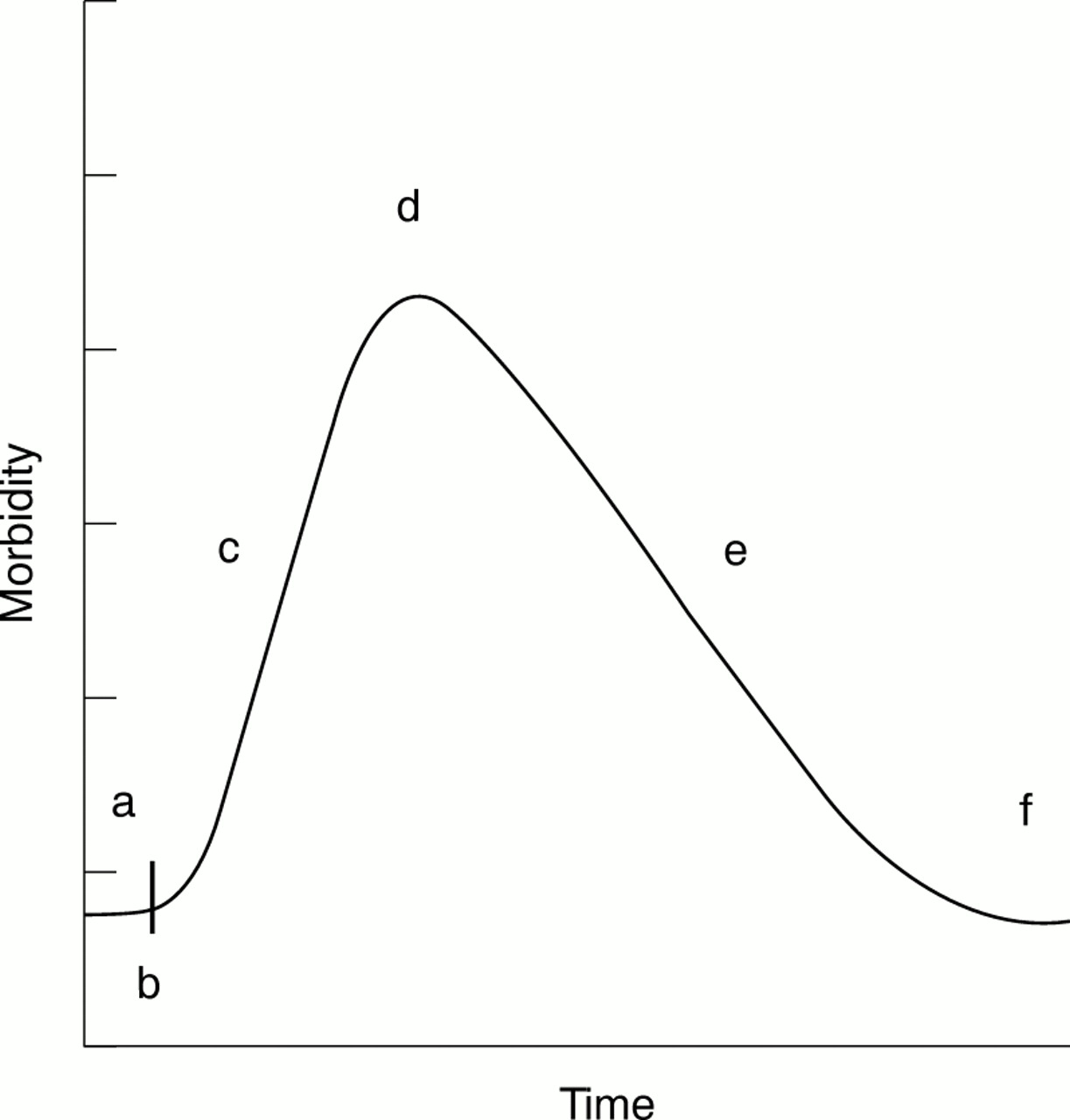
Although there have long been reports of mass psychogenic illness,25 ,26 such social phenomena are difficult to study under controlled conditions. Careful case studies do suggest a natural history that follows a somewhat predictable course (fig 1): (a) Initially, some people appear to be more susceptible, and may share one or more risk factors at baseline.26 These may include stressful life circumstances, low control over the perceived threat, a higher than normal baseline pool of initial physical symptoms of unknown origin (particularly symptoms that are stress related or sufficiently ambiguous to allow reinterpretation or reattribution), personal traits and circumstances that favour emotion focused rather than problem solving strategies, low or dysfunctional social support, and higher rates of pre-existing health, interpersonal, and psychological problems. (b) An initial threat and possible set of symptoms is identified. (c) Concern and awareness spreads, and the prevalence and severity of symptoms escalate. This may be accelerated if authorities pronounce these as a new syndrome or disease. (d) Diffusion of threat and incidence of complaints peak. (e) Complaints diminish in a recovery process as potential threatening causes are credibly eliminated. In smaller communities, it has often been the trusted, well informed family doctor who has a key role in this reassurance and reattribution. (f) Eventually, concerns return to baseline.

{kind=link}
Mass psychophysiological phenomena are assumed to affect large groups and share key features: In the normal course (a) a baseline of diffuse symptoms and risk factors, (b) initial perceived health threat, (c) diffusion, with increased incidence and severity of symptoms as concern spreads, (d) point of maximum diffusion and average morbidity, (e) trend reversal with decreasing prevalence and severity in response to decreased threat and reassurance, and (f) return to baseline.
Some aspects of the response to implants may reflect mass somatisation, and there are several points that might have particular relevance: (a) The baseline pool of diffuse physical symptoms might have been larger than average for women with complaints attributed to implants. Medical devices and procedures may represent extra risks for mass somatisation by nature of the high invasiveness and low personal control involved. Recent studies have also suggested that women, in general, may have a higher rate of diffuse baseline medical symptoms and complaints—for example, higher incidences of diffuse muscle pain, irritable bowel syndromes, and chronic fatigue.18 ,27 Also, the medical and psychological histories of women who seek breast augmentation appear to differ from those of other women, and cosmetic surgery, generally, may alter social support, coping, and information seeking mechanisms.28(b) Spread of concern about implants might have been accelerated and prolonged by mass media and early high profile litigation. (c) Modern media distribute concerns so broadly, geographically, so quickly, that normal self limiting or corrective forces may be less effective, and perceived threat more difficult to define and contain. (d) The United States Food and Drug Administration moratorium placed upon silicone gel-filled implants might have increased the atmosphere of potential threat. (e) As a result of all of the above the return to baseline might have been more sluggish and frequently interrupted. (f) As large numbers of people enter litigation, certain psychological factors become more salient. Litigation adds counterincentives to recovery, though these are probably subconscious rather than deliberate.2 Claimants are likely to be evaluated by plaintiffs' experts who may reaffirm their fears of disease and threat. Claimants may also be counselled by attorneys and support groups who further stimulate their fears. We have also found, in samples of patients with chronic pain, that those in litigation tend to (a) report more symptoms, particularly obvious rather than subtle clinical symptoms used for differential diagnosis, or (b) favour physical rather than psychological explanations for symptoms.29 These may be selectively symptoms that are more easily reattributed to injury related concerns.
Treatment implications
If even some of the symptoms associated with the complaints of people with implants can be attributed to somatisation, stress, mass somatisation, or other psychophysiological responses, then there may be important implications for treatment. Little in the way of intervention has emerged, to date, from the focus of epidemiological studies upon disease outcomes. Because these studies conclude that there is no reliably increased risk of specific diseases for women with implants, there generally is no next step proposed for intervention. However, somatisation, as presently proposed, produces real symptoms, interacts with other real symptoms, and may produce high levels of morbidity.24 Clearly, a careful study of possible intervention models is needed.
Barsky and Borus suggest guidelines for medical management of potential somatisation phenomena13:
Approach patients presenting with these types of complaints with careful medical examinations to rule out specific disease, yet avoid tests solely for the purposes of reassuring the patient, to avoid iatrogenics that may enhance the sick role or reinforce the conviction that the patient has some unknown biomedical disease
Evaluate for the presence of psychiatric disorders and yet reassure the patient that this does not mean that the cause of symptoms is imaginary
A collaborative therapeutic relationship is crucial, in which the patient feels that their suffering is understood
The emphasis should be upon coping and rehabilitation to improve functioning and reduce impairment. Reilly similarly emphasises that patients must be helped to become more active in managing their symptoms by efforts such as exercising, losing weight, or practising stress management22
The process of symptom amplification should be explained, as well as the interactive roles of psychological factors and symptoms more generally
If problems persist, formal cognitive behavioural treatment should be prescribed.
Review of related publications is encouraging about the potential benefit of application of cognitive behavioural psychological interventions. These interventions generally include a combination of structured, directive techniques targeting relaxation training, stress reduction, facilitation of more normalised activity, and alteration of negative or anxiety promoting thinking patterns. Barsky and Borus cite considerable reports that show potential benefit from cognitive behavioural treatment for various somatic symptoms, including those associated with irritable bowel, fibromyalgia, and chronic fatigue syndrome.13 Similarly, a review of 49 treatment outcome studies of behavioural interventions for fibromyalgia concluded that the combination of drug treatment, cognitive behavioural therapy, and exercise produced the most favourable outcomes,30 and a recent review of treatments for chronic fatigue syndrome found that cognitive behavioural interventions have been shown to increase patients' level of functioning.31 In view of the symptom overlap, effective intervention protocols from these related publications may hold promise for treatment of complaints associated with implants.
Conclusions
Several concerns should be acknowledged. Firstly, there are essentially no direct tests of the presumed effect or treatment of somatisation processes in women with breast implants. I am relying heavily upon comparisons of symptoms with those of other disorders and other circumstances. Controlled studies to test these assumptions are clearly needed. Secondly, there are likely to be symptoms that fall outside this model—for example, the specific local complications of breast implants that occur in a proportion of cases. There are also clearly women with implants who have a variety of coincidental specific diseases not caused by implants.
None the less, we may be able to reduce distress and morbidity among women with implants by taking a broader viewpoint. Large scale health related fears, accusations, and litigation have substantial psychological aspects. Psychological aspects may even be suspected to be the dominant forces when there is no specific physical cause or when the morbidity exceeds what might be expected from a specific physical agent. This is especially true in disorders that have a strong social component, such as those cases in which a large group of people begin to present with similar new patterns of subjective complaints, or when mass tort or mass media hype is involved. In such instances, a model of mass somatisation effects may help to guide towards timely intervention, research, and prevention.
Litigation over breast implants may continue, but regardless of the presence, absence, or size of settlements, there are women who continue to struggle with unexplained symptoms and worry about the implications for their health and their future. Reassurance is often not sufficient, and the litigation climate surrounding implants may counteract reassurance efforts that otherwise would be sufficient. Residual complaints, psychological and psychophysiological, should not be dismissed as imaginary, unimportant, or factitious without evidence. Existing methods of treatment for the broader spectrum of somatisation and stress related disorders, combined approaches to behavioural and medical rehabilitation, and the development of new interventions tailored to women with implants, warrant serious consideration.
Acknowledgments
Based upon a paper presented at the annual meeting of the Society for Behavioral Medicine, San Diego, USA, 1999. I thank Dow Corning Corporation for its support. Dr Laura Perkins, Dr Ralph Cook, Dr Patti Klein, Dr Susan Hoshaw, Dr Steve Bowlin, and their associates have provided helpful comments on earlier versions of this work.