Article Text

Abstract
Objective To review the cost effectiveness of rheumatoid arthritis (RA) treatments and inform the clinical recommendations by the European League Against Rheumatism.
Methods A systematic literature search and review of the health economic evidence on RA treatment options was performed.
Results Despite diverse methodological approaches, health economic analyses are concordant: at onset of disease, traditional disease-modifying antirheumatic drugs (DMARDs) are cost effective—that is, treatment merits outweigh treatment costs. If DMARDs fail, therapeutic escalation with tumour necrosis factor α inhibitors (TNFi) is cost effective when standard dosing schemes are employed. If TNFi fail, rituximab or abatacept is cost effective. Economic evidence for switching TNFi remains sparse.
Conclusions The costly sequelae of insufficiently controlled RA justify intensive escalations of treatment in this disease. By maintaining function, patients are kept in the work process, reducing indirect costs. Quality of life is improved at an expense commonly accepted for chronic diseases. Effective control of disease activity seems to be a prudent use of societal resources.
Statistics from Altmetric.com
Introduction
Inflammatory rheumatic diseases, in general, have substantial financial implications.1,–,4 Recently, the broadened therapeutic armamentarium with biological antirheumatic drugs has led to marked improvements in disease activity and joint damage, but has dramatically raised direct medical costs.5 Rheumatoid arthritis (RA) often affects people at an age of high work productivity6 and has significant consequences on physical functioning and working capacity.7,–,9 Incorporating indirect costs due to loss of productivity7 allows for a more complete look at the economic implications10 of RA treatments, and is recommended for sensitivity analysis.11 The GRADE recommendations for the development of guidelines12 encourage the incorporation of economic issues. To account for this, we systematically reviewed existing evidence on the cost effectiveness of RA treatment options to inform the recommendations for therapeutic management of RA.
Methods
In November 2008, the European League Against Rheumatism (EULAR) created and charged a task force to develop a guidance document for the use of synthetic and biological DMARDs in RA. The expert panel decided to deal with the cost effectiveness of therapeutic options in one of the five subgroups examining different aspects of the therapeutic management.
To collect and review the evidence, we performed a systematic literature review (SLR) aiming at economic evaluations of RA treatment. The search used Medline, Embase and Cochrane databases to identify publications concerning economic aspects of adult RA, published in English from the year of database inception until December 2008 (Figure 1). In addition, we hand-searched abstracts presented at the 2007 and 2008 ACR and EULAR conferences. To maximise retrieval of all pertinent papers we applied medical subject headings (‘MeSH’ terms), or keyword searches when at all appropriate. Box 1 and table 1 provide the specific details of the search strategies. After scanning all titles and abstracts, we retrieved the full text for all potentially relevant studies. These retrieved articles were also hand searched for further references. We did not exclude studies of poor quality, but did subsequently assess all papers for quality using the Oxford EBM Level of Evidence classification.13 Lastly, to account for potential bias, we extracted the funding source stated in the original publications (table 2).

Search and selection process. (Initial comprehensive search strived for cost-effectiveness analyses and cost of illness studies.)
PICO strategy for the search
Funding as declared in published cost-effectiveness analyses: acknowledgements/grants/affiliations
Box 1 Search terms and strings (initial search aming at cost-effectiveness analyses and cost of illness studies)
*Arthritis, Rheumatoid/co, ec, rh, su, th, dt, sn, co, ec, su, rh, th, nu, px, mo, dt, pc OR *Arthritis, Rheumatoid/ OR rheumatoid arthritis.mp.
*Rheumatoid Arthritis/dt, rh, si, th, co, dm, su, dr OR rheumatoid arthritis.mp. OR *Rheumatoid Arthritis / OR rheumatoid adj arthritis(*”Costs and Cost Analysis”/td, mt, st, ut, ec, og, cl) OR (*Economics/ or *Economics, Medical/ or *Economics, Hospital/ or *Economics, Pharmaceutical/) OR ($economic$ or COI$ or CEA$ or cost$ or QUALY$ or (quality$ adj2 adjust$) or $financial$ or (willingness adj2 pa$) or (purchas$ adj power$ adj parit$) or PPP$ or (monte adj carlo$) or markov$ or (standard$ adj gambl$) or SG or trade-off$ or TTO$ or (rating adj scale) or RS$ or utility or utilities or (preference$ adj bas$) or HUI$ or EQ-5D or SF-6D or MAUT$ or model$ or ICER or (piggy adj back) or (discret$ adj event$ adj simulation$) or DES or (friction$ adj2 cost$) or $capital$ or productivit$ or (health$ adj year$ adj equivalent$))
(*”Health Care Cost”/ or *”Cost Effectiveness Analysis”/ or *”Drug Cost”/ or *”Cost Control”/ or *”Hospital Cost”/ or *”Hospitalization Cost”/ or *”Nursing Cost”/ or *”Cost Utility Analysis”/ or *”Cost Benefit Analysis”/ or *”Cost Minimization Analysis”/ or *”Cost”/ or *”Cost of Illness”/) OR (*Health Economics/ or *Economic Aspect/) OR ($economic$ or COI$ or CEA$ or cost$ or QUALY$ or (quality$ adj2 adjust$) or $financial$ or (willingness adj2 pa$) or (purchas$ adj power$ adj parit$) or PPP$ or (monte adj carlo$) or markov$ or (standard$ adj gambl$) or SG or trade-off$ or TTO$ or (rating adj scale) or RS$ or utility or utilities or (preference$ adj bas$) or HUI$ or EQ-5D or SF-6D or MAUT$ or model$ or ICER or (piggy adj back) or (discret$ adj event$ adj simulation$) or DES or (friction$ adj2 cost$) or $capital$ or productivit$ or (health$ adj year$ adj equivalent$))
($economic$ or COI$ or CEA$ or cost$ or QUALY$ or (quality$ adj2 adjust$) or $financial$ or (willingness adj2 pa$) or (purchas$ adj power$ adj parit$) or PPP$ or (monte adj carlo$) or markov$ or (standard$ adj gambl$) or SG or trade-off$ or TTO$ or (rating adj scale) or RS$ or utility or utilities or (preference$ adj bas$) or HUI$ or EQ-5D or SF-6D or MAUT$ or model$ or ICER or (piggy adj back) or (discret$ adj event$ adj simulation$) or DES or (friction$ adj2 cost$) or $capital$ or productivit$ or (health$ adj year$ adj equivalent$))
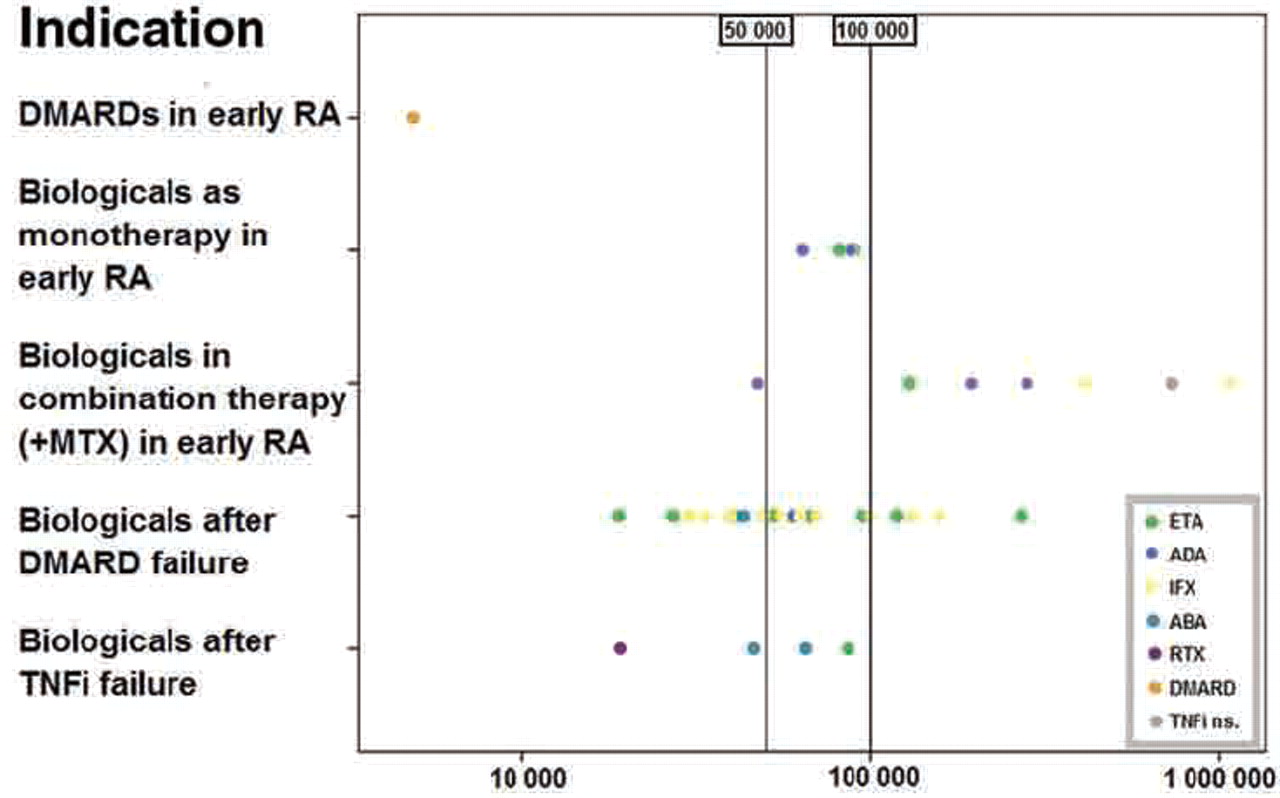
Where possible, we collected cost effectiveness results as an incremental cost-effectiveness ratio (ICER), the most frequently reported outcome in cost-effectiveness analyses (CEAs) reflecting the additional cost per quality-adjusted life-year (QALY) gained by a particular treatment. Although the exact societal willingness-to-pay threshold remains controversial, based on ICERs of other commonly accepted medical interventions, we defined ICERs below US$50 000–100 000 per QALY, as being cost effective.
The costs considered for QALY derivation in CEAs included direct costs (ie, cost of the drug, drug monitoring and adverse events, hospital visits, etc) in all publications, while heterogeneous approaches were taken for the inclusion of indirect costs (generated by loss of patient productivity). Where available, we report on how the QALYs were calculated.
Results
Presumably because biological treatments are far more expensive than traditional DMARDs or glucocorticoids, the majority of published cost-effectiveness studies examined biological treatments (40 of 54) while few considered synthetic disease-modifying antirheumatic drugs (DMARDs).14,–,21 The following sections present the CEA results for different treatment options according to their treatment indications with results specified as ICERs if available.
DMARD naïve early RA
Although synthetic DMARDs in early RA are generally assumed to be cost effective because of their low cost, published data are limited. CEAs have been carried out for methotrexate (MTX),20 ,21 sulfasalazine (SSZ)20 and leflunomide (LEF).22 LEF appears to be cost effective in comparison with SSZ.15 When comparing the efficacy of LEF and MTX, results of published randomised controlled trials (RCTs)23 ,24 are not consistent, which is consequently reflected in the CEAs modelled on basis of these RCTs.15 DMARD use in early RA is cost effective in comparison with a pyramid strategy that is based on non- steroidal anti-inflammatory drugs and steroids for 1 year before starting DMARDs in non-responders.21
Tumour necrosis factor α inhibitors (TNFi)
TNFi have been investigated in DMARD naïve early RA. Infliximab (IFX) has been investigated in combination with MTX in early disease,25 whereas etanercept (ETA) has been randomised as monotherapy against MTX,26 and adalimumab (ADA) has been investigated as monotherapy and in combination with MTX in early disease.27 Three full study reports20 ,28 ,29 and one abstract30 ,31 dealt with cost effectiveness of TNFi use in DMARD naïve patients. Updating the SLR based on expert opinion yielded two additional full-text publications.21 ,32 (Table 3 and figure 2 summarise and illustrate published ICERs, table 4 lists all treatment options considered in CEAs.)

{kind=link}
{kind=link}
Published incremental cost-effectiveness ratios. x-Axis=incremental cost-effectiveness ratio in US$ per quality-adjusted life-year gained (log scale); y-axis=indication for the use of biological agents; dots represent reported ICERs of the drugs investigated. Values to the left of the vertical lines at US$50 000 and US$100 000 are commonly considered to be cost effective. Note, that comparing ICERs between trials is inappropriate. ABA, abatacept; ADA, adalimumab; DMARD, disease-modifying antirheumatic drug, ETA, etanercept; ICER, incremental cost-effectiveness ratio; IFX, infliximab; RTX, rituximab; TNFi ns., tumour necrosis factor α inhibitor, not specified.
ICERs of biological agents published in cost-effectiveness analyses
Modelled treatment sequences in cost-effectivenes analyses investigating first-line TNFi use
First-line monotherapy with TNFi in DMARD naïve patients
Cost-effectiveness of ADA or ETA monotherapy when compared with MTX monotherapy in DMARD naïve patients depends on where cost-effectiveness thresholds are set.20 ,28 ,29 In a CEA presented by Spalding and Hay,29 starting treatment with ADA monotherapy produced a high ICER (US$63 769) than with MTX monotherapy, and starting with ETA monotherapy was calculated to produce an even higher ICER of US$89 772. When sensitivity analyses on ETA were performed that also accounted for productivity outcomes, ETA use resulted in lower ICERs, but still ranged above the US$50 000 threshold (US$78 691). Choi et al20 compared several treatment options in MTX naïve patients, among them ETA monotherapy. In this study, the ICER was calculated by use of probabilities of achieving ACR20 or ACR70 weighted response (WR) instead of QALYs, which makes outcomes difficult to compare. The authors conclude that whether this option is cost effective when compared with MTX monotherapy depends on whether >US$40 000 per additional 6 month ACR20 or ACR70 response is considered acceptable.20 Chen et al28 calculated ICERs in the cost-effective range for ADA and ETA monotherapy used as first-line agents (figure 2, tables 3 and 4).
Using first-line combination of MTX and TNFi as initial treatment in early RA resulted in high ICERs in several studies.21 ,28 ,29 This strategy precludes initial MTX monotherapy, and subsequent escalation with TNFi if necessary. Even though initial combination therapy including biological agents has shown clinical superiority over monotherapy,27 there is currently no evidence supporting this strategy with regards to cost effectiveness. MTX is comparably cheap,28 yet efficient, in many patients. There are currently no effective ways to predict poor treatment success with MTX alone, therefore, also from the cost-effectiveness perspective, a course of MTX should be encouraged in all patients without contraindications, and an initial combination of TNFi with MTX cannot be considered cost effective.28 ,29 The lowest ICER was generated for ETA plus MTX, but this still amounted to £78 000 (year of pricing 2004).28 A few CEAs showed relatively lower ICERs: in one abstract30 ,31 from 2008, first-line use of ETA in combination with MTX had an ICER of €24 655 for severe disease and €30 199 for highly active disease, respectively, when compared with a strategy of second-line ETA added to MTX. Similarly, ADA plus MTX32 in early RA had an ICER of US$23 377 per QALY based on effectiveness data from registration trials25,–,27 sponsored by industry (see table 2).
Consequently, an initial combination of TNFi with MTX was not felt to be consistently cost effective in comparison with initial MTX monotherapy.
Apart from CEA publications, there is currently also no definite evidence from subanalyses and follow-up data of clinical trials that indicates a preference for initial combination therapy. In a recently published subanalysis of the BeSt study,33 whether IFX costs could be largely compensated by productivity increases depended on the value attached to productivity gains. When using the so called friction method to calculate productivity costs, a similar effect on productivity could also be achieved by the much less expensive strategy that included an initial combination therapy with high-dose prednisone.33 The authors note, that longer follow-up data should be gathered to correctly evaluate patterns of IFX use. Indications for cost effectiveness of an initial TNFi combination therapy come from subanalyses of the Premier trial34 and the PROWD study,35 which found significantly better outcome for indirect costs (work loss, performance and sick leave) with early combination therapy including ADA versus MTX alone. These studies did not investigate the potential effect of higher-dose steroids.
In summary, biological agents in early RA have not been investigated as thoroughly as after DMARD failure, mainly owing to a paucity of evidence on effectiveness in this indication from RCTs. Consequently, economic evaluations also provide sparse information. A first-line combination of a TNFi with MTX in early disease must be applied judiciously, with most studies finding early TNFi and MTX not cost effective in comparison with a schedule of initial MTX monotherapy with the option to add a biological agent in the absence of a sufficient response. MTX monotherapy provides a satisfactory strategy at a low price for many patients. Therefore, until and unless higher-risk groups with non-response to MTX can be readily identified, TNFi for now appear to be most cost effective when used after DMARD failure.28
DMARD failure
DMARDs after DMARD failure
Given its higher price, only LEF has been investigated intensively among synthetic DMARDs.22 ,36 ,37 Studies argued, however, that a strategy including LEF might be worthwhile by potentially postponing the initiation of biological agents. In short, ICERs reported for this strategy when compared with TNFi are above acceptable thresholds.36 Use of LEF after DMARD failure, followed by a switch to ETA only if LEF proved insufficient after 3 months, was considered to be more cost effective than using ETA earlier,36 but still an ICER of £163 556 was reported. However, indirect costs were not incorporated. The efficacy data used38 reported LEF outcomes in comparison with MTX (ie, investigating MTX naïve patients). In the absence of direct comparison trials for patients qualifying as candidates for TNFi, in the model LEF was arbitrarily assumed to be 25% less effective when following MTX failure36 than when used in MTX naïve patients.
Biological agents after DMARD failure
Considering society's willingness to pay ICER thresholds of US$50 000–100 000, a combination of TNFi plus MTX as a group is cost effective after synthetic DMARD failure,28 ,39 with thorough analyses of ADA,40 ,41 ETA40,–,45 and IFX.44 ,46,–,49 For IFX, a limitation has been raised and confirmed in cost-minimisation analyses50 ,51—namely, that the doses of IFX have to remain constant over time,28 ,40 although this analogously will apply to the use of higher doses of other TNFi, which has, however, not been investigated. With the exception of one study, which was based on a comparison of non-head-to-head trials and therefore different trial populations,28 there is no strong evidence that one TNFi is better than another. With increasing functional disability at baseline, lower ICERs are observed in this indication (Health Assessment Questionnaire (HAQ) <0.6: ICER=€128 500, year of publication 2002; vs HAQ >2.1: ICER=€43 00044).
Some criticism has been raised of these TNFi cost-effectiveness results,36 ,46 ,52 ,53 specifically arguing that high ICERs depend on the methods used to determine utility46 or objecting to generally higher ICERs36 ,52 ,53 (table 3). For some of these studies, there has been a re-evaluation of the publications by newer data published by the same group (Jobanputra et al52 published updated papers in 200454 and 200628). The exceptionally high ICERs reported by Welsing et al36 did not incorporate indirect costs.
A Canadian study53 also presented ICERs above the US$100 000 threshold but in sensitivity analyses considered a higher impact on indirect costs. However, this study did not specify how ICERs were derived. Choi et al55 again used an ACR20 and ACR70 WR making ICER comparisons problematic (table 3). Anakinra has not been considered cost effective in two CEAs,40 ,56 essentially because of its low efficacy in RCTs.56 Abatacept (ABA) after MTX failure has been investigated recently and was suggested to be cost effective57 based on efficacy data from the AIM trial.58 For this indication, our search also retrieved one abstract presented at the EULAR 2008 conference,59 but specific results and data are unavailable.
After failure of one or more TNFi
Rituximab (RTX) has been shown to be cost effective60,–,62 based on modelling of REFLEX trial data.62 ,63 In this indication, ABA was also reported as cost effective64,–,66 (models were based on ATTAIN trial data,67 the latter studies were sponsored by Bristol-Myers Squibb; table 2), although it has initially been rejected by the National Institute for Health and Clinical Excellence report68 because it exceeds the £30 000 threshold. To date, there are no randomised head-to-head comparisons of RTX and ABA available. In an abstract report, ABA was postulated to be more cost effective than RTX64 in a model derived from AIM58 and REFLEX.63 Comparison of the two has also been undertaken and reported by Gossec et al69 as an abstract.
Sequential TNFi use
There is little evidence on this treatment option, reflecting again the absence of RCT data. Chen et al28 found ETA, unlike ADA and IFX, to be cost effective when used as the second, and even as the third TNFi (table 3), but in their models, sequential TNFi use was compared with the treatment option of returning to DMARD treatment only. A treatment sequence of ETA following ADA plus MTX had a calculated ICER of US$19 663,32 and similarly Brennan et al39 reported favourable ICERs for use of a second TNFi, when investigating TNFi as a class versus DMARD treatment (table 3).
Cost effectiveness of treatment strategies
In the TICORA70 study, aggressive versus conservative treatment was also analysed for cost effectiveness: at 18 months, higher costs had accrued in the group treated aggressively (due to a larger number of outpatient visits, and higher costs for travel, diagnostic tests and prescriptions), but were offset by considerably lower costs in this group owing to lower hospitalisation costs and fewer additional health professional visits. Of note, in a CEA, that compared symptomatic versus aggressive treatment in late RA,71 symptomatic treatment was more cost effective than intensive treatment. In a subanalysis of the FinRA-Co,72 combination DMARD treatment with glucocorticoids was shown to be a protective factor against productivity loss after 5 years of follow-up. Also, two COBRA subanalyses73 ,74 found combined treatment effective at equal or lower costs than monotherapy.
The results of this literature research have been incorporated in guidelines for RA management by use of a set of recommendations as summarised in table 5.
Final results
Conclusions
Despite heterogeneous methods applied in CEAs making it difficult to compare studies,75 ,76 economic analyses support the EULAR RA treatment recommendations. In particular, the economic analyses support the concept of an early start of traditional DMARDs, and rapid treatment escalation when there is insufficient response. In this strategic setting, the considerably more costly biological treatments appear to provide sufficient cost effectiveness. The current EULAR RA treatment recommendations are consistent with prudent use of societal resources. To reflect the long-term functional impairment from RA, productivity losses should be considered in sensitivity analyses.
References
Footnotes
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Competing interests None. Francis Berenbaum was the Handling Editor.