Article Text

Abstract
Objectives To summarise existing evidence on a target oriented approach for rheumatoid arthritis (RA) treatment.
Methods We conducted a systematic literature search including all clinical trials testing clinical, functional, or structural values of a targeted treatment approach. Our search covered Medline, Embase and Cochrane databases until December 2008 and also conference abstracts (2007, 2008).
Results The primary search yielded 5881 citations; after the selection process, 76 papers underwent detailed review. Of these, only seven strategic clinical trials were extracted: four studies randomised patients to routine or targeted treatment, two compared two different randomised targets and one compared targeted treatment to a historical control group. Five trials dealt with early RA patients. All identified studies showed significantly better clinical outcomes of targeted approaches than routine approaches. Disability was reported in two studies with no difference between groups. Four studies compared radiographic outcomes, two showing significant benefit of the targeted approach.
Conclusion Only few studies employed randomised controlled settings to test the value of treatment to a specific target. However, they provided unanimous evidence for benefits of targeted approaches. Nevertheless, more data on radiographic and functional outcomes and on patients with established RA are needed.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Many new treatment options make unprecedented outcomes achievable in rheumatoid arthritis (RA).1 2 In parallel, insights on the importance of early effective therapy3 4 and implications of disease activity on function5 6 and joint damage6,–,8 led to paradigmatic changes in therapeutic approaches, such as frequent evaluations of disease activity to allow for timely changes of therapies.9,–,13 Additionally, validated composite disease activity measures have made disease activity assessment easy.14 15 Nevertheless, heterogeneity of therapeutic aims and patient expectations16 characterise daily practice of RA treatment.17 All this suggests a need to provide rheumatologists and patients with pertinent information on therapeutic targets and means to achieve them.18 19
Strict definitions of treatment targets intend to facilitate strategic acting in routine care and require physicians and patients to discuss and adopt therapeutic changes within distinct time frames, ideally following therapeutic algorithms. This approach has been utilised in many diseases, like diabetes,20 21 hypertension22,–,24 or hyperlipidaemia.25 However, this policy needs to be evidence based to the best possible extent.
Here we report on a systematic review of available evidence regarding the effects of treating RA strategically according to defined outcome targets.
Methods
Shaping the systematic literature review
As a first step, the international steering committee of the Treat-To-Target (T2T) project, comprising a group of expert rheumatologists and a patient (MdW), designed a literature search that aimed at ‘treating to target’-strategy trials in RA. The search was then performed by a project fellow (MS), a control search by a second fellow (RK) and by two mentors (DA, DvdH).
The following definitions were made: (1) strategy trial – clinical trial of any RA drug treatment, in which a clear outcome target was the primary end point and therapeutic consequences of failing to reach the target were predefined; (2) targets – a target could be formulated by clinical, serological, patient-reported, functional, or radiographic variables; individual measures (eg, joint counts or acute phase reactants), composite scores (eg, disease activity score or simplified disease activity index), or response criteria (eg, those defined by the American College of Rheumatology (ACR) or the European League Against Rheumatism) were considered alike; (3) outcomes – Clinical, functional, serological and/or radiographic changes, as defined in the respective trials, were compared between treatment groups.
Implementation of the systematic literature review
We searched Medline, Embase and Cochrane databases from their inception until December 2008. Additionally, ACR and European League Against Rheumatism (EULAR) abstracts of 2007 and 2008 were screened. The search was limited to humans, adults and the English language. Detailed inclusion and exclusion criteria and the list of search strings are shown in supplementary tables (tables S1 and S2). We did not exclude studies based on quality.
From the identified strategy trials, data were extracted concerning definitions of targets and success rates of applied strategies.
Results
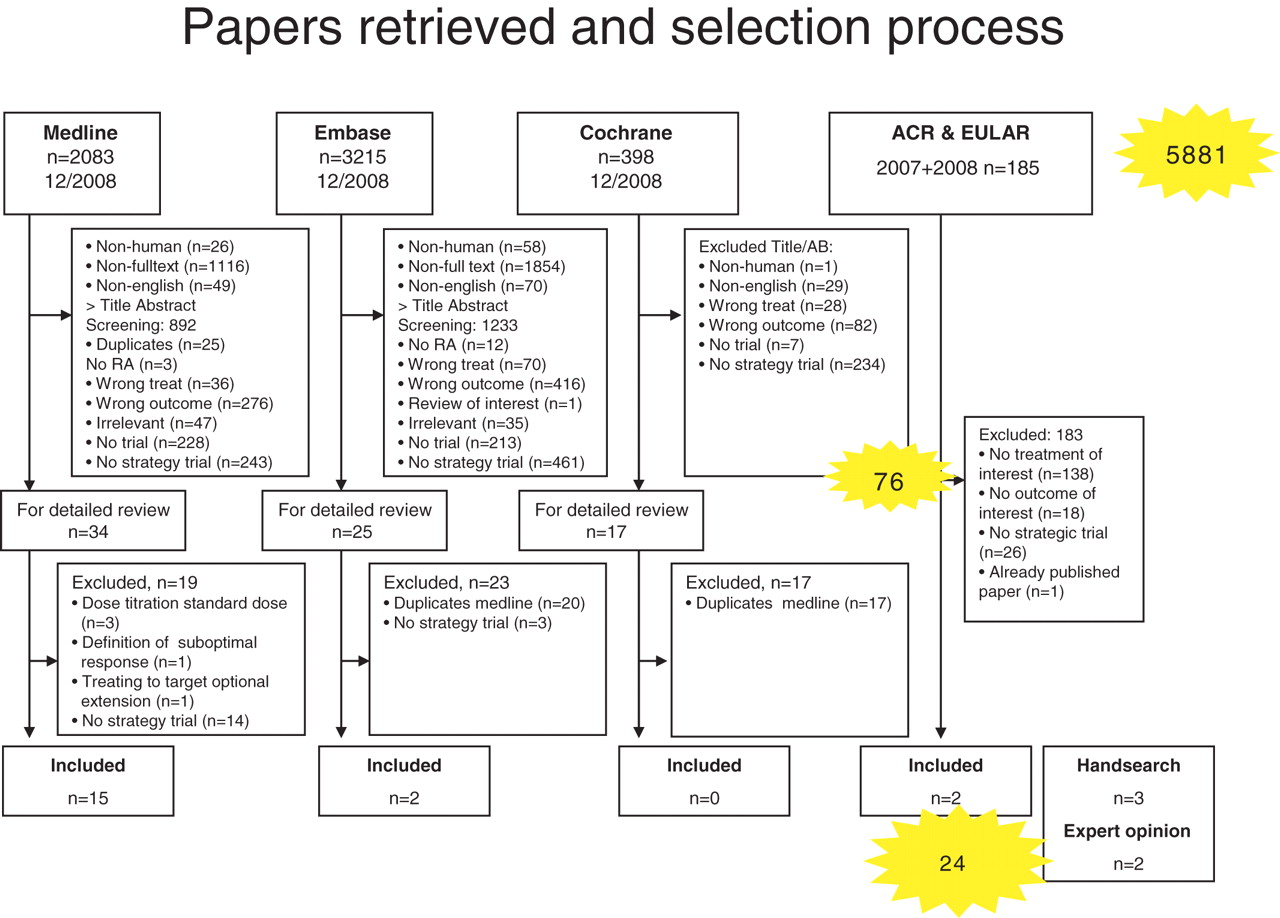
We retrieved 5881 citations for further evaluation (figure 1). Title and abstract screening according to our selection criteria (supplementary table S1) left 76 papers for detailed review. Among those, 17 trials published in full and 2 abstracts addressed direct assessment of treating to target. By hand search of references, we identified three additional papers; further, one full paper and one abstract were included based on expert opinion. This gave a total of 24 publications for this review (figure 1), of which only 7 were strategic trials: 4 trials randomised patients to routine or targeted treatment,26,–,29 two compared different randomised targets30 31 and one compared targeted treatment to historical control.32
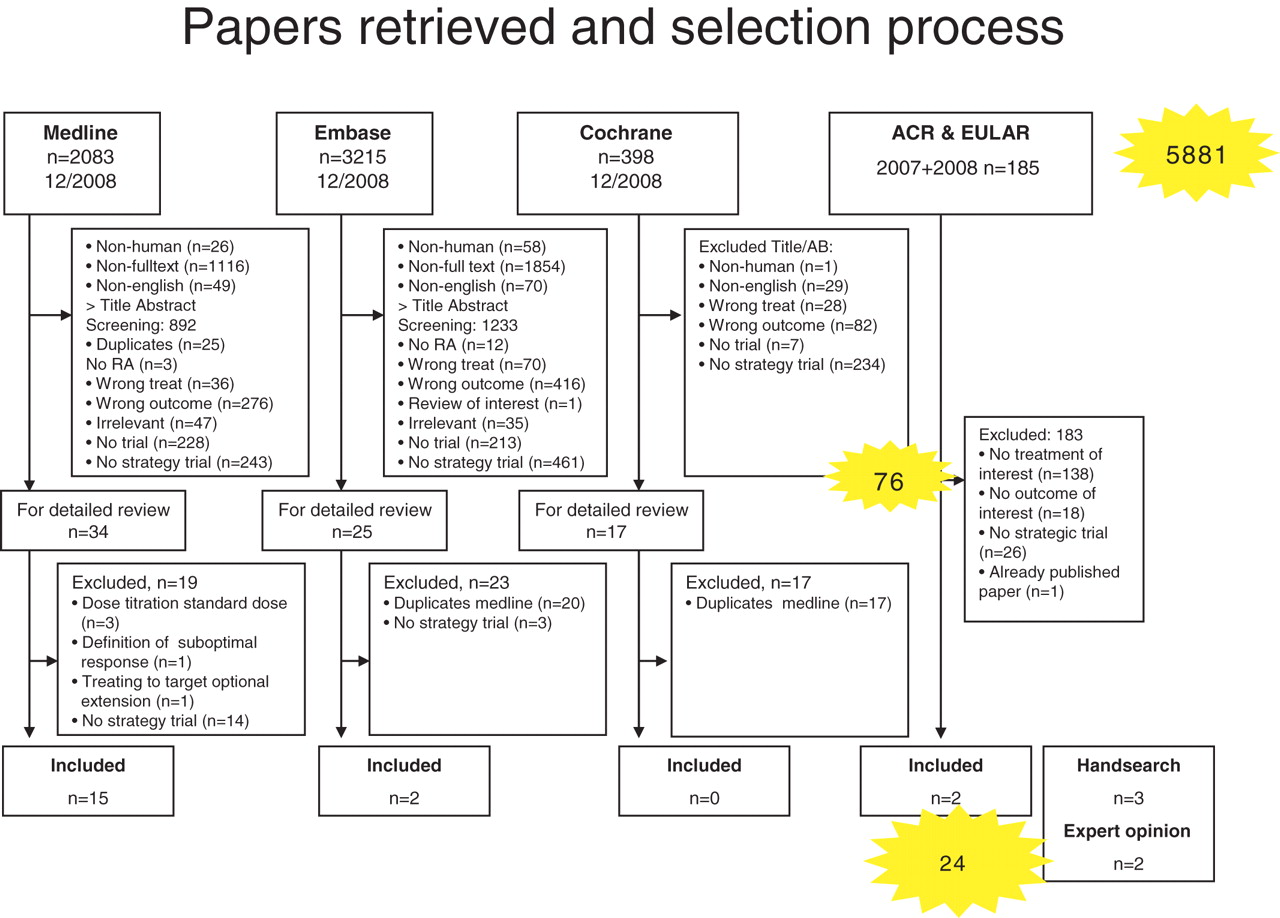
Flow chart of the systematic literature search. Illustrated are the results of the initial search and the selection process of abstract screening, full text review and hand search. AB, abstract; ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; RA, rheumatoid arthritis.
Randomised strategic trials comparing targeted versus routine care
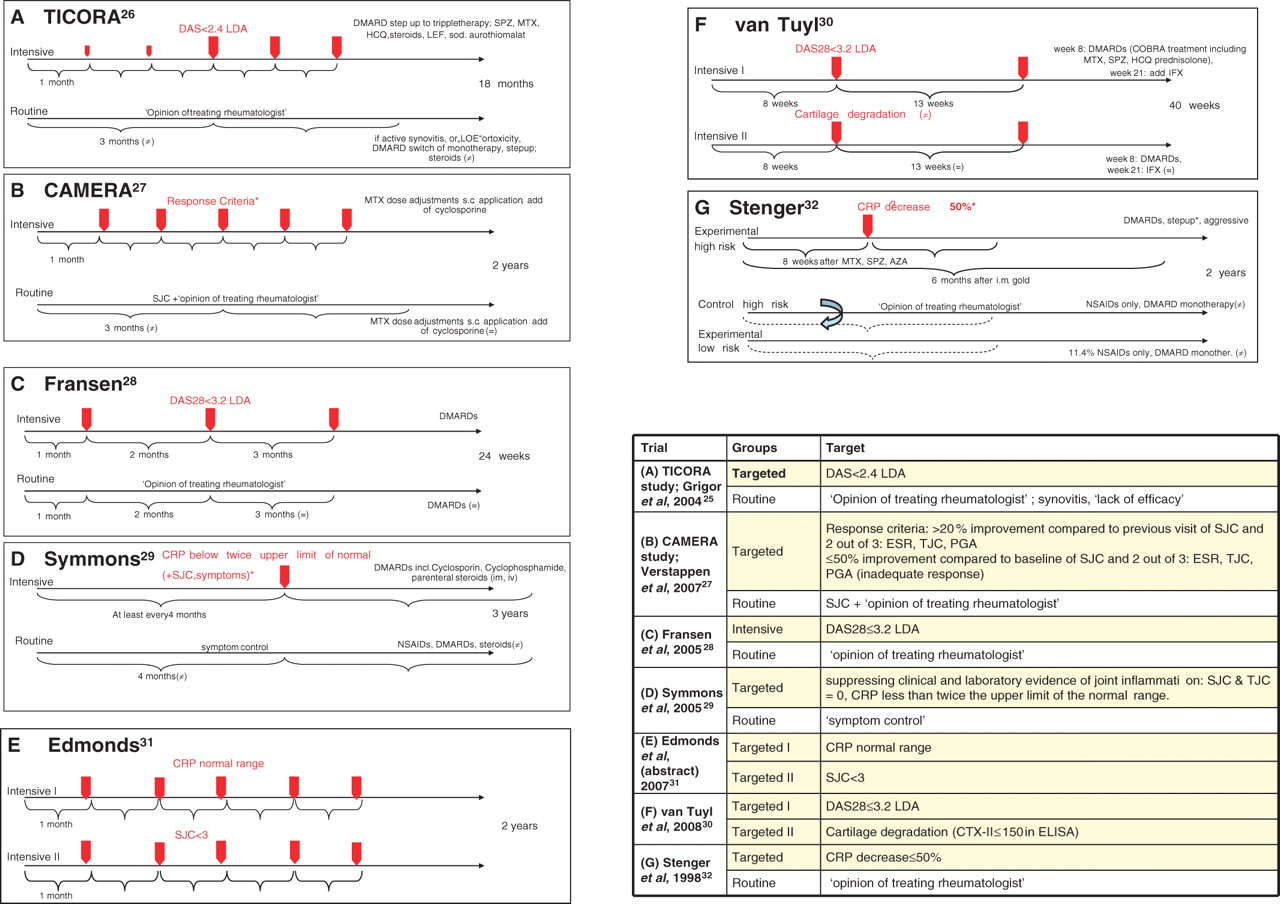
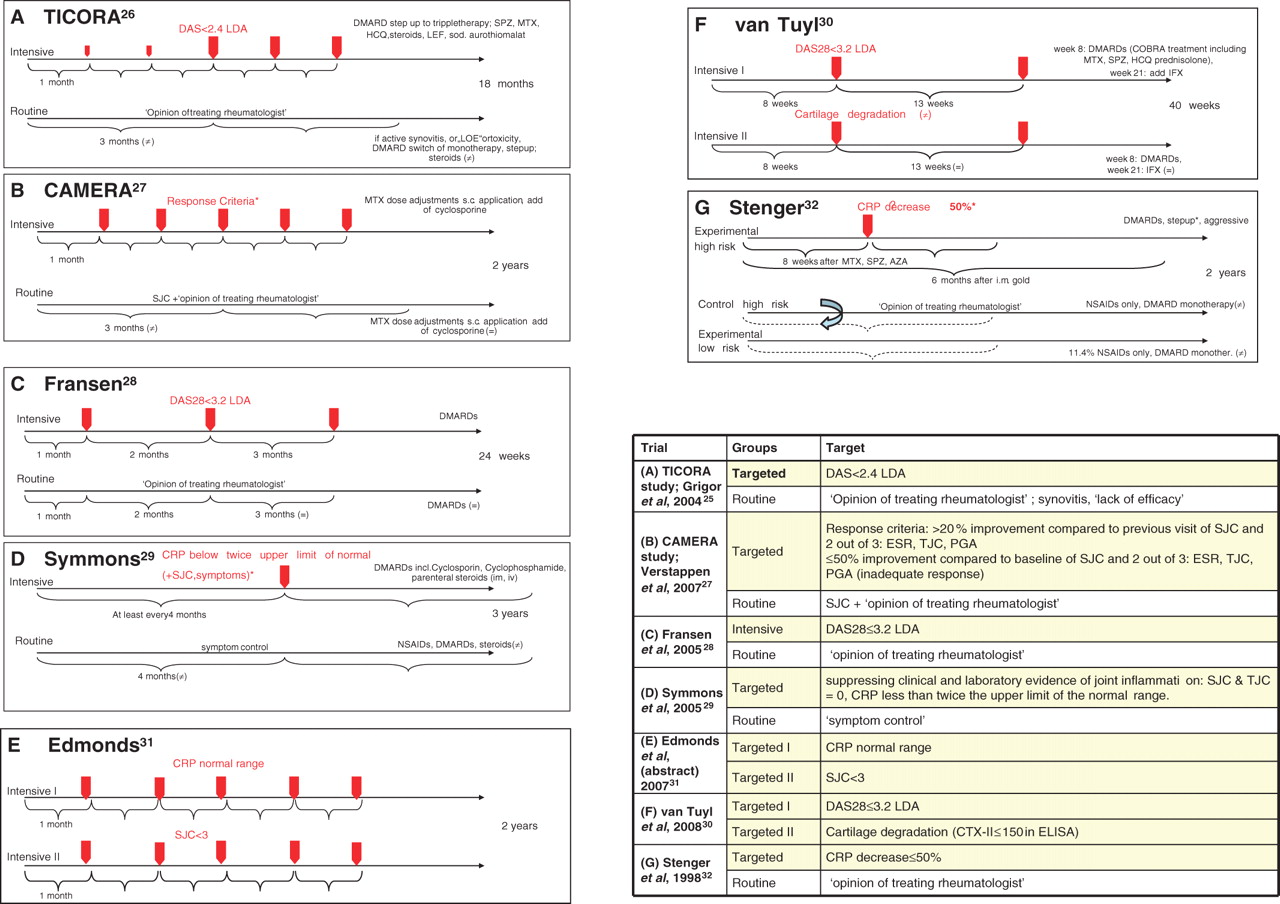
Only four trials had randomised patients to a targeted treatment algorithm versus routine care. In Tight Control of Rheumatoid Arthritis (TICORA),26 treatment of early RA aimed at low disease activity (LDA) by Disease Activity Score (DAS), comparing DAS-driven treatment adaptations upon monthly assessments with 3-monthly routine care. Computer Assisted Management in Early Rheumatoid Arthritis (CAMERA)27 aimed at remission of early RA, comparing monthly treatment adaptation by computerised decision if >20% (50%) reduction of several variables was not attained with 3-monthly routine care. A cluster randomised trial by Fransen et al 28 compared the proportion of patients reaching LDA at the end of follow-up and the number of disease-modifying antirheumatic drug (DMARD) changes during 24 weeks (co-primary end points) in outpatient centres using systematic, DAS28-steered treatment protocols with centres providing routine care. The treatment decision in the DAS28-driven group depended on a threshold of 3.2, indicating LDA. Finally, Symmons et al29 tested the effect of aggressive versus symptomatic therapy on physical outcome (Health Assessment Questionnaire (HAQ)) in established RA. Decisions for treatment adaption were driven by joint count- and C reactive protein (CRP) thresholds. Designs of these trials are depicted in figure 2; baseline characteristics are tabulated in supplementary table S3.
{kind=link}
{kind=link}
Design of the seven core clinical trials. (A) TICORA study (Grigor et al 2004)26; (B) CAMERA study (Verstappen et al 2007)27; (C) Fransen et al 200528; (D) Symmons et al 200529; (E) Edmonds et al 2007 (abstract)31; (F) van Tuyl et al 200830; and (G) Stenger et al 1998.32 Intensive and routine treatment arms are displayed, red arrows mark the scheduled intervals for target assessment. Table 1 specifies the targets of trials A–G. AZA, Azathioprine; CAMERA, Computer Assisted Management in Early Rheumatoid Arthritis; CRP, C reactive protein; DAS, Disease Activity Score; DMARD, disease-modifying antirheumatic drug; HCQ, hydroxychloroquine; IFX, ifosfamide; LDA, low disease activity; LEF, leflunomide; MTX, methotrexate; NSAID, non-steroidal anti-inflammatory drug; sc, subcutaneous; SJC, swollen joint count; sod., sodium; SPZ, sulfinpyrazone; TICORA, tight control of rheumatoid arthritis.
Targets and visit intervals (left columns) and clinical, functional and structural outcomes (right columns) of core trials
Characteristics of the core trials, including treatment targets and visit intervals, as well as clinical, functional and radiographic outcomes are summarised in table 1 and will be detailed below.
Significantly greater DAS reduction and higher likeliness to achieve remission following intensive disease management was evident in all four trials. In TICORA,26 the primary end point, EULAR good response, as well as DAS remission were significantly more frequent upon intensive than routine care. CAMERA27 showed significant benefits of targeted treatment regarding its primary end point, remission for 3 months. Fransen et al28 showed that both the proportion of patients reaching LDA and frequency of DMARD changes during follow-up favoured a DAS28-driven DMARD strategy. Symmons et al29 found significant differences in clinical outcomes in the evaluator global assessment, while other measures, including joint counts, erythrocyte sedimentation rate and patient global visual analogue scale, were not significantly different.
Physical function was the primary outcome in the trial by Symmons et al29; the intensive group failed to show significant differences compared to routine care regarding HAQ changes. Also CAMERA27 did not show significant differences in functional outcomes.
Grigor et al26 reported significantly less progression of radiographic changes26 in the intensive treatment group. In contrast, no significant differences in annual radiographic progression were described in the CAMERA study.27 Two of the studies did not report radiographic data28 29 (table 1, figure 2).
Randomised strategic trials comparing two targeted strategies
van Tuyl et al30 presented a study protocol randomising early RA patients to different targeted and tight monitoring schedules: one group aiming at DAS28 remission, the other at suppressing cartilage degradation as assessed by measuring urinary C-terminal cross-linking of type II collagen. Results did not differ significantly between the two groups with similar overall remission rates in both arms (figure 2, table 1). However, as the authors concede, this was a very small pilot study. Similarly, Edmonds et al31 reported in abstract form on steering at normal CRP levels versus a joint count targeted approach. Their results suggested that targeting CRP provides better interference with radiographic damage (table 1, figure 2).
Non-randomised cohort studies comparing two targeted strategies
Stenger et al32 compared an aggressive treatment protocol that stipulated change of DMARD therapy if after 8 weeks CRP decrease was less than 50% in patients with a high risk of developing aggressive disease; the comparator arm on regular therapy was a retrospectively assessed group of high risk patients. After 2 years, the area under the curve for CRP was significantly lower in the intensive treatment group than in the historic control. While no functional data were provided, the reported radiographic progression favoured the intensive treatment (table 1).
Additional studies
A number of studies used the treat to target concept, but, in contrast to the mentioned papers, did not have a non-targeted control arm, since all arms pursued the same target with different treatment sequences (supplementary table S4). Likewise, several trials compared step-up with combination regimes, dose titration of agents or different therapies to reach a defined target without directly addressing the efficacy of treating to target. A description of these studies can be found in the supplementary material accompanying this manuscript.
Discussion
Our review revealed that only few controlled studies investigated the value of strategic treatment schedules. Importantly, study designs and evaluated targets were very heterogeneous; for example, the Edmonds and van Tuyl studies are inherently different in design as compared to the others in that their approach compares two T2T approaches while the others compare a T2T approach with the routine approach. Nevertheless, all studies investigating early disease showed significantly better clinical outcomes of the targeted approach. Functional outcomes, reported in two trials, failed to show significant gains.27 29 Four studies compared radiographic outcomes,26 27 29 32 of which two showed a significant benefit of the targeted therapy.26
Five26,–,28 30 32 studies investigated early disease (using different definitions of ‘early’ – see supplementary table S3). Only one trial29 focused explicitly on late disease (duration: >5 years) and found no advantage of tight control on functional outcomes. Thus, patients with established RA seem to be underinvestigated regarding the value of treating to a target. Since longer disease duration impairs treatment outcomes,33 extending results from early RA to the general patient population could be misleading. Furthermore, just focusing on HAQ might also be misguiding, since with increasing disease duration responsiveness of physical function to therapeutic interventions decreases (even to placebo levels).34
Utilised targets showed considerable heterogeneity (table 1, figure 2). Among the randomised trials comparing targeted versus routine approaches, three out of four employed state targets,26 28 29 an approach that has been favoured as being more appropriate than assessing changes from baseline.35 Only in CAMERA,27 the target was formulated as reaching defined improvement criteria. Also, visit intervals were noticeably heterogenous: clinical assessments were performed from monthly26,–,28 31 to every 429 36 months. Two trials randomised patients to different visit intervals.26 37 In both, patients assigned to intensive strategy were seen monthly, those in routine care every 3 months.
In conclusion, only few studies have used a randomised approach to test the value of treatment to a specific target. However, all of them provided compelling evidence of clinical benefits of such an approach. However, more data are needed concerning radiographic and functional outcomes and patients with longstanding RA have not been sufficiently investigated.
References
Supplementary materials
Web Only Data ard.2009.123976
Files in this Data Supplement:
Footnotes
MS and RK Contributed equally to this study
-
Competing interests This study was supported by an unrestricted educational grant from Abbott Immunology. Abbott had no influence on the selection of papers, extraction of data or writing of this manuscript. Francis Berenbaum was the Handling Editor.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous