Article Text

Abstract
Objectives: To assess whether smoking is a risk factor for developing rheumatoid arthritis (RA).
Design: Meta-analysis.
Method: Data sources were observational studies that examined the association between smoking history and the risk of developing RA identified through Medline and EMBASE (from 1966 to December 2006), relevant books and a reference search. Two authors independently extracted the following: authors’ names, publication year, sample size, participant characteristics, odds ratios (OR) or relative risks, adjustment factors, study design and area where the study was conducted. Data syntheses were based upon random effects model. Summarised syntheses effects were expressed by OR.
Results: Sixteen studies were selected from among 433 articles. For men, summary OR for ever, current and past smokers were 1.89 (95% CI 1.56 to 2.28), 1.87 (1.49 to 2.34) and 1.76 (1.33 to 2.31), respectively. For rheumatoid factor-positive (RF+) RA, summary OR for ever, current and past smokers were 3.02 (2.35 to 3.88), 3.91 (2.78 to 5.50) and 2.46 (1.74 to 3.47), respectively. Summary OR for 20 or more pack-years of smoking was 2.31 (1.55 to 3.41). For women, summary OR for ever, current and past smokers were 1.27 (1.12 to 1.44), 1.31 (1.12 to 1.54) and 1.22 (1.06 to 1.40), respectively. For RF+ RA, summary OR for ever, current and past smokers were 1.34 (0.99 to 1.80), 1.29 (0.94 to 1.77) and 1.21 (0.83 to 1.77). Summary OR for 20 or more pack-years of smoking was 1.75 (1.52 to 2.02).
Conclusion: Smoking is a risk factor for RA, especially RF+ RA men and heavy smokers.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a major autoimmune disease, with typical clinical features of chronic inflammation in joints and the development of bone destruction.1 Although the aetiology of RA is unknown, it is thought that the interaction of environment, genetics and the immune system may lead to the development of this disorder.1
Smoking is thought to be a risk factor for the development of several autoimmune diseases, including systemic lupus erythematosus,2 primary biliary cirrhosis,3 Graves’ disease4 and RA.5 6 7 8 9 10 11 12 Smoking modulates the immune system13 by reducing natural killer cells, depressing hormonal cells and cell-mediated immunity, and leading to dysfunction of T lymphocytes.14 15 16 17
Epidemiological studies of the past 20 years have investigated smoking as an important risk factor for RA and have reported several key findings.1 3 4 5 6 7 8 9 10 The first is a stronger influence of smoking on developing RA in men, and the second is the association of smoking with rheumatoid factor (RF) positive RA in men, but not in women.7 18 However, the findings for women of various studies have been inconsistent.7 18 19 20 21 22 Moreover, although several reviews have dealt with the relation between smoking and the development of RA, no systematic analyses have been conducted.23 24 25 26 27 28
We therefore conducted a meta-analysis to assess whether smoking habits affect the development of RA.
Methods
To report our meta-analysis, we followed the Moose checklists, the proposal for reporting meta-analysis of observational studies.29
Data sources and searches
An article search was conducted through Medline and EMBASE from 1966 to December 2006 using the keywords “Rheumatoid Arthritis” and “Smoking.” We used both the Medline MeSH term (“Arthritis, Rheumatoid”) and text words (“Rheumatoid Arthritis” and “smoking”) for our Medline search. In addition, we performed a search of the references cited in each paper and a book that reviewed the relationship between RA and nutritional or environmental risk factors.1 For study selection and data extraction, we also examined what other possible confounding factors (such as age, social class, body mass index, education, coffee consumption and menopause status), affect developing RA generally.
Study selection
Inclusion criteria: studies included in our meta-analysis comprised the following minimum requirements: (1) any type of observational study (case–control or cohort study) investigating the relationship between the development of RA and smoking habits, with no limit for smoking status (ever, current and past); and (2) effect size data (odds ratio (OR) or relative risk (RR) and CI) related to RA development among smokers compared with non-smokers were estimated. For different studies of the same populations (eg, the Nurses’ Health Study), we used the results of the most recent study.
Excluded studies: case reports, basic medical reports about RA and smoking, and studies concentrating on other environmental factors (eg, coffee intake) or severity of RA.
Data extraction and quality assessment
Data extraction was independently performed by two authors. We extracted the following data from each paper: author’s name; publication year; sample size; effect size data (OR or RR) for risk of development of RA; study design (case–control or cohort); area where the study was conducted; adjustment factors (eg, age).
For the sample size, we also extracted subgroup data classified by gender. If we could not obtain effect size data adjusted with other confounders, we estimated the crude OR from sample size data. When mentioned, we also obtained data for RF-positive or RF-negative findings, anti-citrulline protein/peptide (CCP) positive or negative and effect size by pack-years of smoking for subgroup analyses. The quality of the selected studies was assessed with the checklist proposed by Rushton.30 This check list contains 14 items answered by “Yes” or “No”, and we used the number of “Yes” answers to determine the study quality with a score between 0 and 14, and these scores were used for meta-regression analysis.31 If results were significantly affected by study quality scores, we weighted study quality scores on data syntheses. We resolved any item discrepancies through discussion and adopted the more conservative results.
Data synthesis and analysis
Statistical models and software
All data syntheses were based upon a random effect model,32 which allowed us to compare the effect of factors other than smoking on the development of RA in any of the studies. Forest plots were used to express the effect size data of each study and summary OR with 95% CI estimated from each study. We used R version 2.60 (R Development Core Team, Vienna, Austria), S-Plus version 7.0 (Insightful Corp, Seattle, Washington, USA), and Comprehensive Meta Analysis version 2 (Biostat Inc, Englewood, California, USA).
Main outcome for evaluation
For the main outcome, the influence of any type of smoking (ever, current and past) on the development of RA in men and women was evaluated separately. The results were stratified by whether the study design was case–control or cohort. Weighted analysis of variance was used to evaluate differences between smoking status and study design.
Heterogeneity among studies
Meta-regression analysis31 was performed to explore the sources of statistically significant (p<0.05) heterogeneity among studies. Possible sources for heterogeneity were smoking habit rates and study quality in each selected study.
Subgroup analysis
For subgroup analyses, the following three items were evaluated for assessment of the influence of smoking on the development of RA limited to the following three topics: (1) differences in expression of RF in the effect of smoking effect on the development of RF-positive as well as RF-negative RA; (2) differences in expression of anti-CCP; (3) effect of pack-years (years of smoking multiplied by packs of cigarettes per day) of smoking. We also performed a sensitivity analysis based on study quality. For example, if one study was lower in quality than another, we performed data syntheses again after the exclusion of the low quality study and compared the results.
Assessment of publication bias
To evaluate publication bias, Rosenthal’s fail-safe number33 in terms of smoking status was calculated for numbers of the selected studies. This number is a standard for estimating how many “null-effect” studies are needed to increase the p value for the meta-analysis to make the summary OR statistically insignificant. As this number increases, so does the reliability of the study results. If the estimated number of unpublished studies according to Rosenthal’s fail-safe number was larger than five times the number of identified studies plus 10 studies, we decided the influence of publication bias on our findings was minor.2 29 33
Results
Characteristics of included studies
Of the 433 articles screened we obtained data from 18 articles that met our inclusion criteria (fig 1, table 1), including 11 case–control and five cohort studies. The mean age of the total population, weighted by the size of each study, was 52.2 years and 94% were women. Smoking rates of ever, current and past were 50.6%, 26.5% and 26.3%, respectively. In the 11 case–control studies,8 9 11 12 18 19 20 21 22 34 35 36 4764 cases and 13 647 controls were included, and in five cohort studies,5 7 10 37 38 9121 cases were identified from among 566 044 participants. Seven case–control studies and one cohort study of male subjects and nine case–control and five cohort studies of female subjects were included. Only Pedersen et al36 investigated the effect of smoking on the development of CCP-positive RA. Classification of pack-years smoked was very different in each of the articles, but all of them included 20 pack-years. We therefore divided the classification of pack-years into “less than 20” or “20 or more”.

Flow diagram of considered articles. RA, rheumatoid arthritis.
Summary of selected studies
Excluded studies
A total of 321 articles was excluded based on their title or abstract and those focusing on in-vitro or non-human studies; case reports were excluded, but were read in full to make sure the topics were based on experimental data or case reports. Among the excluded items, 15 were studies focusing on other environmental factors (eg, diet), and were thus without enough data for our analysis; 42 were editorials or reviews about smoking and RA; 30 focused on extra-articular manifestations or disease severity of RA; five6 40 41 42 43 were based on the same cohorts as one of the studies already included, and three6 38 43 were based on the same cohort (the Nurses’ Health Study). Because their report was the latest, we extracted data from Costenbarader et al.37 Stolt et al 200541 also used the results of the EIRA study (as did Stolt et al 200320 and Padykov et al22), but we excluded one because it was an analysis of a subgroup. Criswell et al 200239 published two articles40 42 based on the same cohort (the Iowa Women’s Health Study) and both of them were excluded because they were reports of a subgroup analysis. We also excluded one study by Jaakkola et al44 because it examined the effect on children of their mother’s smoking, and one by Silman et al45 because its risk estimation focused on twins rather than on individuals.
Overall analysis and evaluation of publication bias
The mean score of study quality according to the Rushton checklist was 11.4 (SD 2.2) with a maximum score of 13 and a minimum score of 5. The item of adequacy of the sample size was rarely assessed as satisfactory. As study quality scores of the selected studies did not have a significant effect as determined by meta-regression analysis, we did not adopt any weighting for our analyses. See supplemental file (published online only).
The summary OR for all of the selected studies were 1.40 (95% CI 1.25 to 1.58) for ever smokers in 14 studies, 1.35 (1.17 to 1.55) for current smokers in 15 studies and 1.25 (1.10 to 1.40) for past smokers in 11 studies. As for the evaluation of publication bias, estimated fail-safe numbers for the selected studies were 403 for ever smokers, 210 for current smokers and 76 for past smokers, suggesting the influence of publication bias was small.
Subgroup analysis by study design (fig 2)
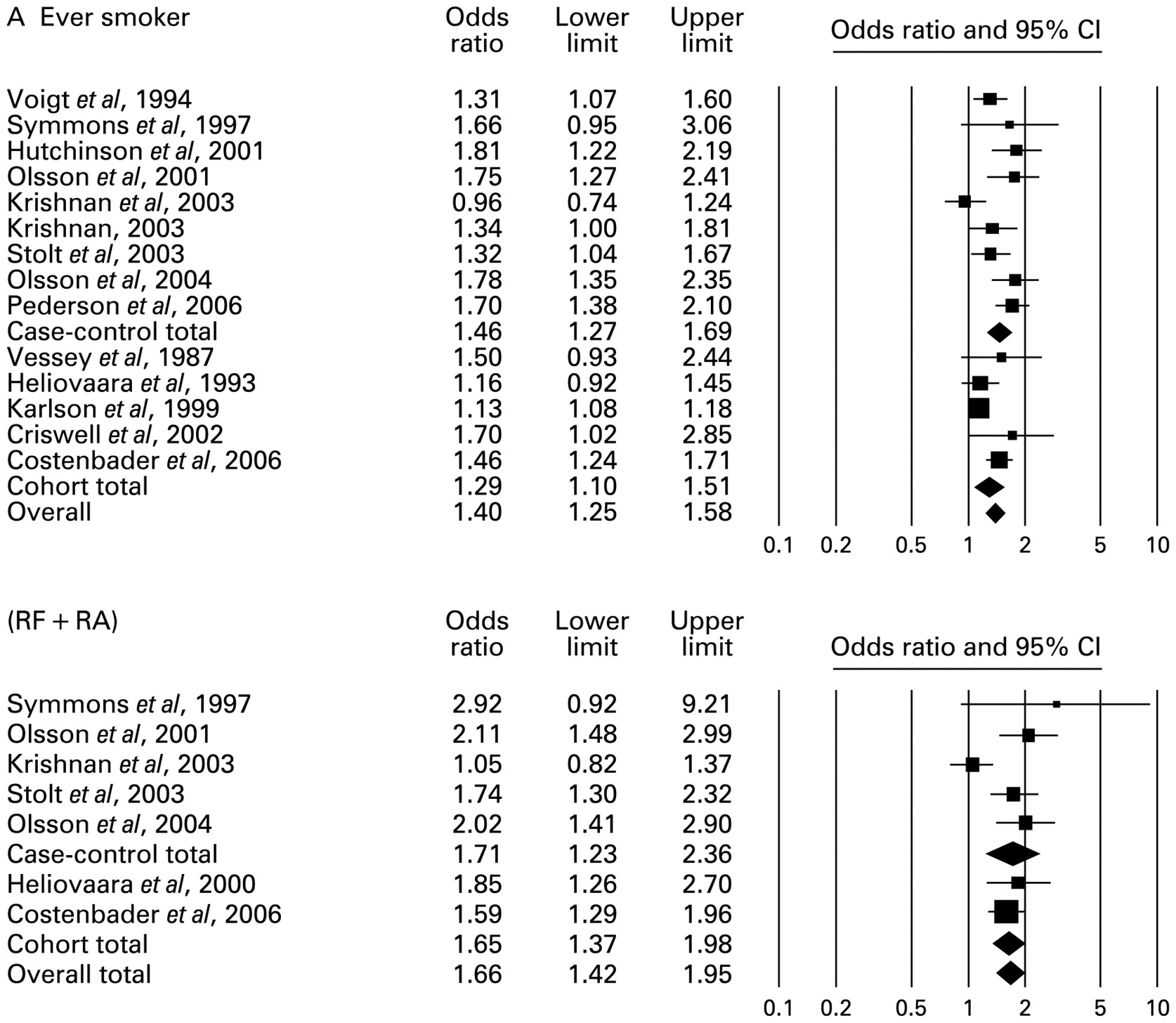
Forest plots of the odds ratio for the risk of developing rheumatoid arthritis (RA) and rheumatoid factor (RF)-positive RA.

Forest plots of the odds ratio for the risk of developing rheumatoid arthritis (RA) and rheumatoid factor (RF)-positive RA in men.
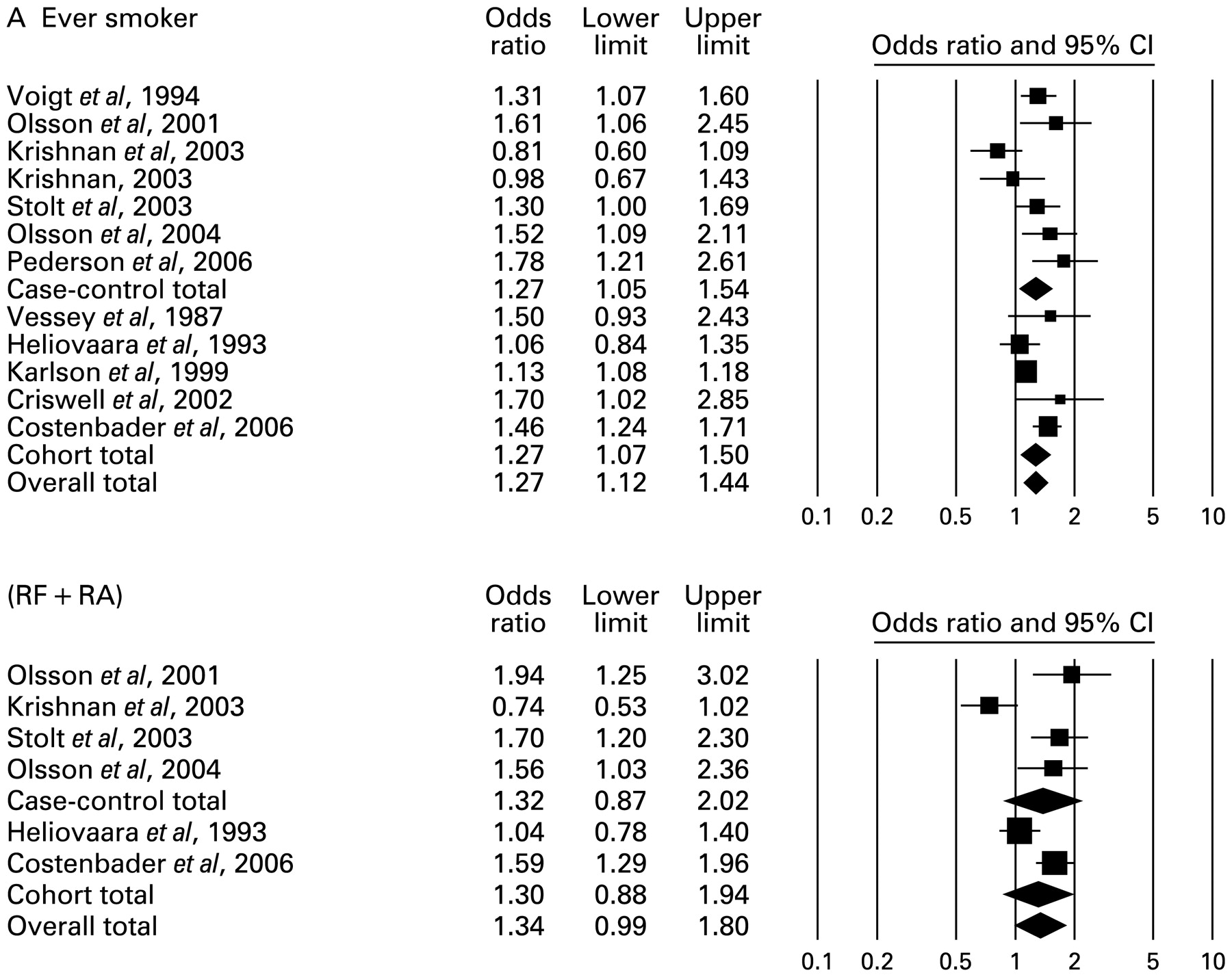
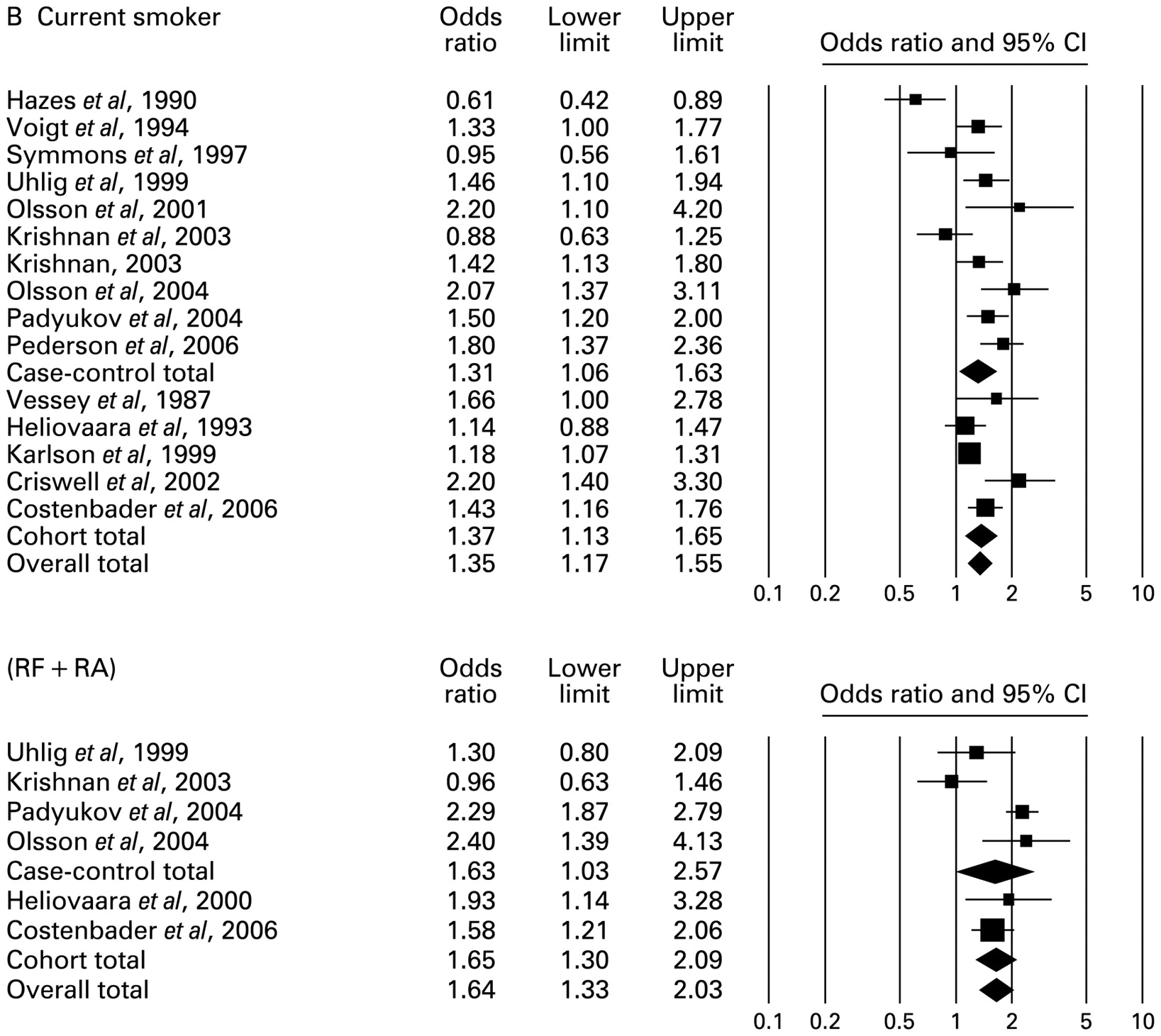
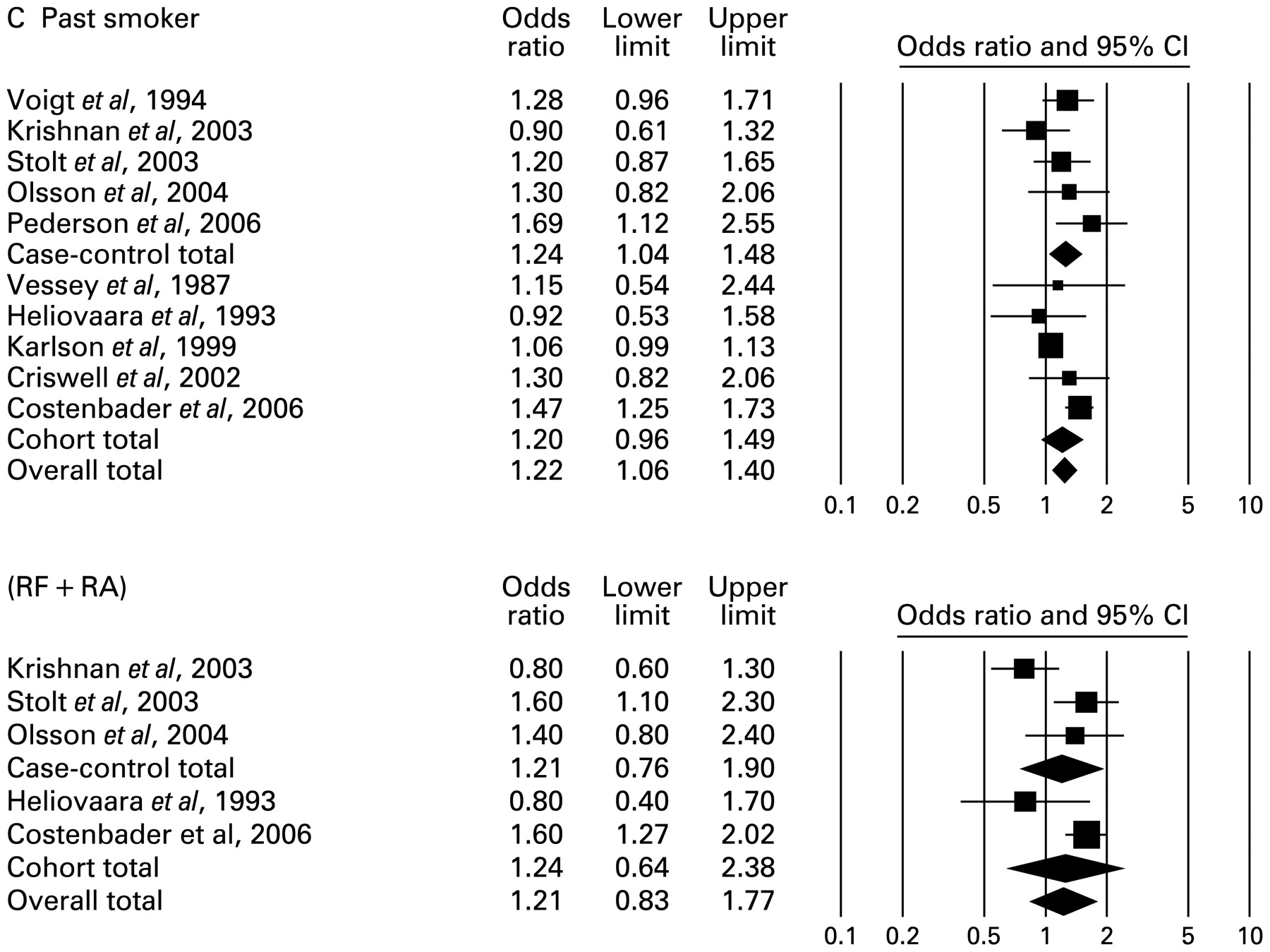
Forest plots of the odds ratio for the risk of developing rheumatoid arthritis (RA) and rheumatoid factor (RF)-positive RA in women.
The summary OR for all the selected case–control studies were 1.46 (1.27 to 1.69) for ever smokers in nine studies, 1.31 (1.06 to 1.63) for current smokers in 10 studies and 1.26 (1.21 to 1.41) for past smokers in six studies.
The summary OR for the selected cohort studies were 1.29 (1.10 to 1.51) for ever smokers in five studies, 1.37 (1.13 to 1.65) for current smokers in five studies and 1.20 (0.97 to 1.49) for past smokers in five studies. Differences in smoking status between the case–control group and the cohort group were not statistically significant.
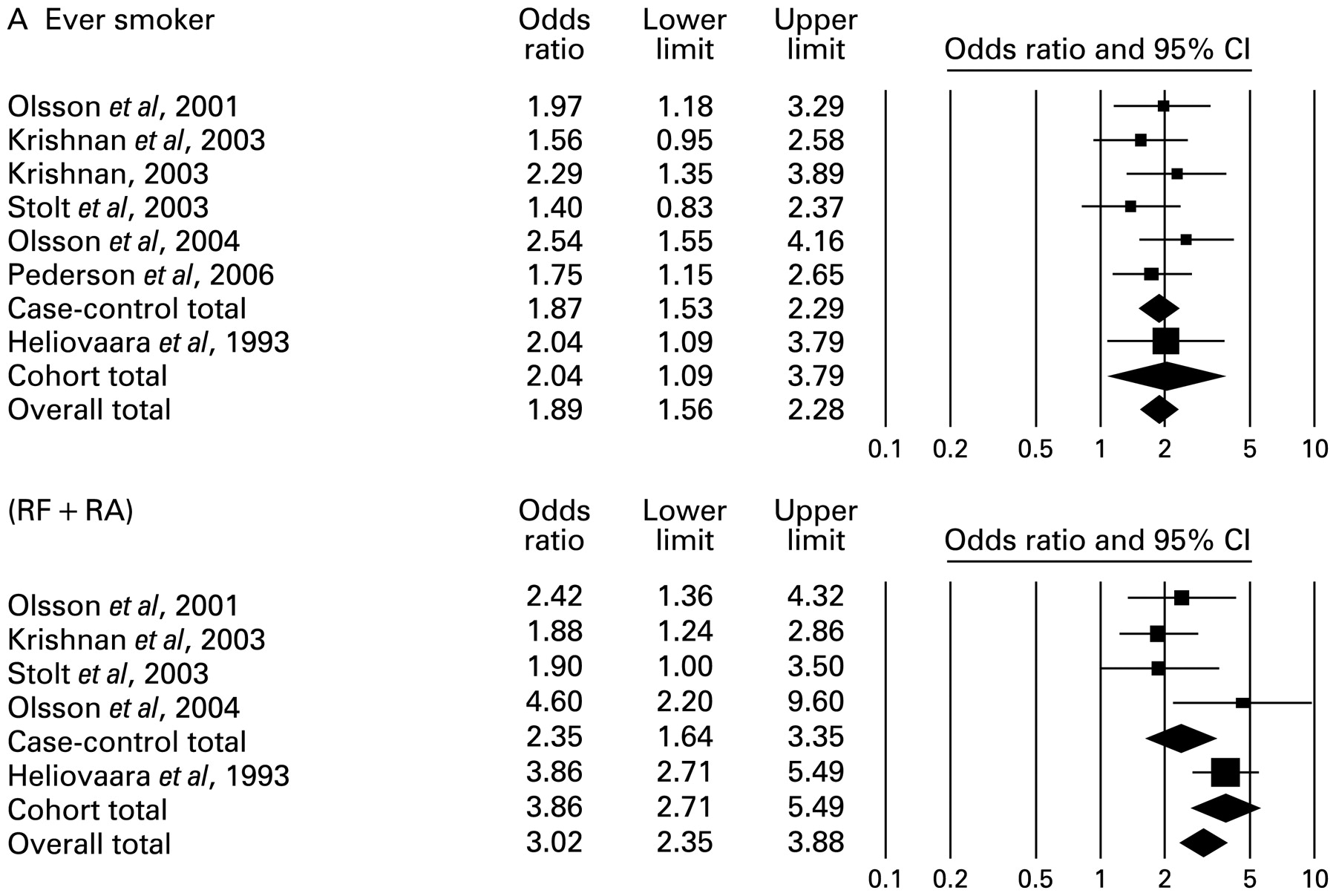
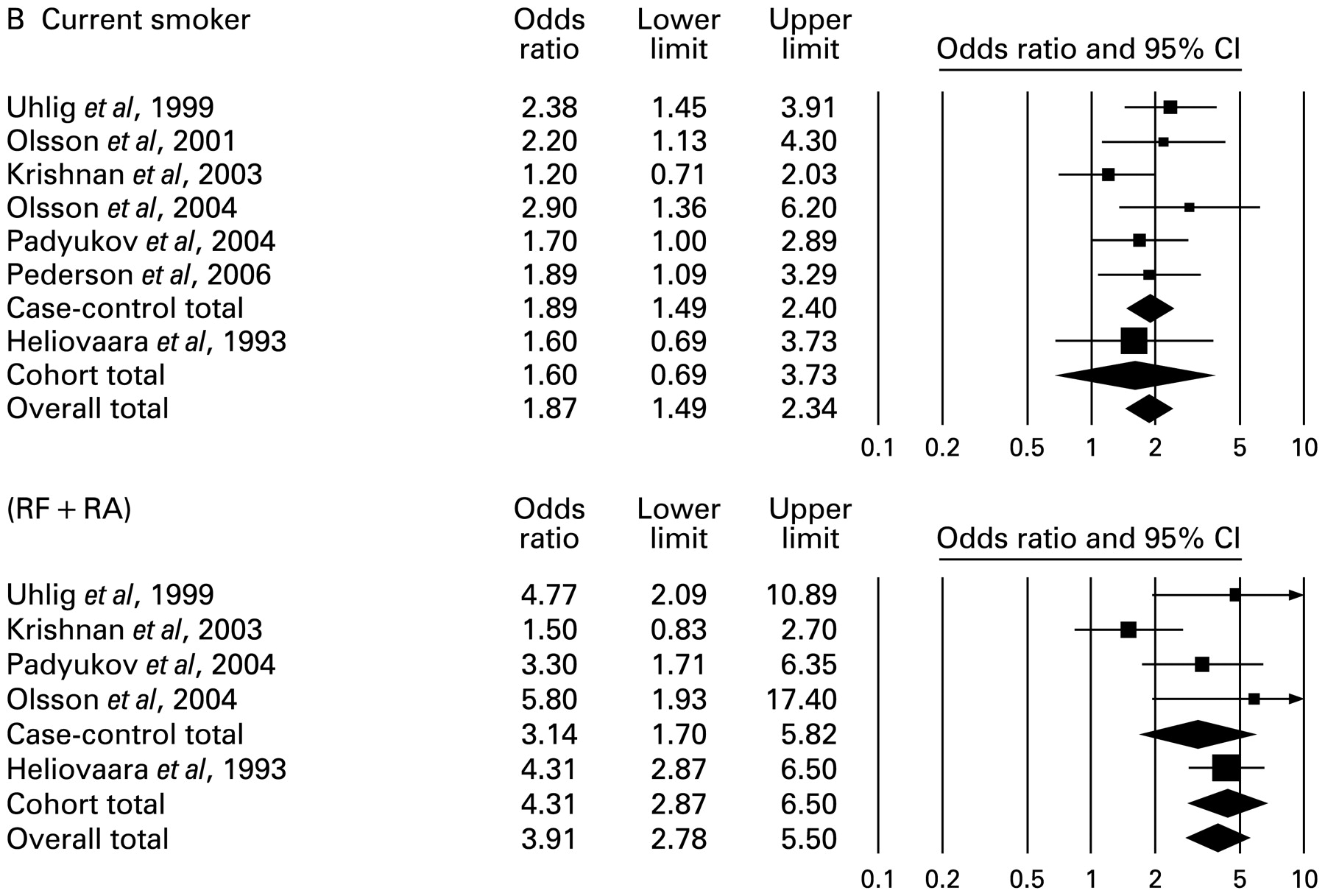
Subgroup analysis for male population (table 2A, fig 3)

Continued.

Summary of results
The summary OR for ever, current and past male smokers were 1.89 (1.56 to 2.28), 1.87 (1.49 to 2.34) and 1.76 (1.33 to 2.31), respectively. For RF-positive RA, the summary OR for ever, current and past smokers were 3.02 (2.35 to 3.88), 3.91 (2.78 to 5.50) and 2.46 (1.74 to 3.47). The summary OR for 20 or more pack-years of smoking compared with non-smokers was 2.31 (1.55 to 3.41).
In the seven case–control studies11 18 19 20 21 22 35 36 the summary OR for ever, current and past smokers were 1.87 (1.53 to 2.29), 1.89 (1.49 to 2.40) and 1.79 (1.34 to 2.38). Differences in smoking status were not significant.
For only RF-positive RA, the summary OR for ever, current and past smokers were 2.35 (1.64 to 3.35), 3.14 (1.70 to 5.82) and 2.35 (1.58 to 3.51), and for RF-negative RA only, the summary OR for ever, current and past smokers were 0.90 (0.52 to 1.27), 1.31 (0.62 to 2.76) and 0.96 (0.61 to 1.51).
Only one cohort study7 was identified in the male subgroup population.
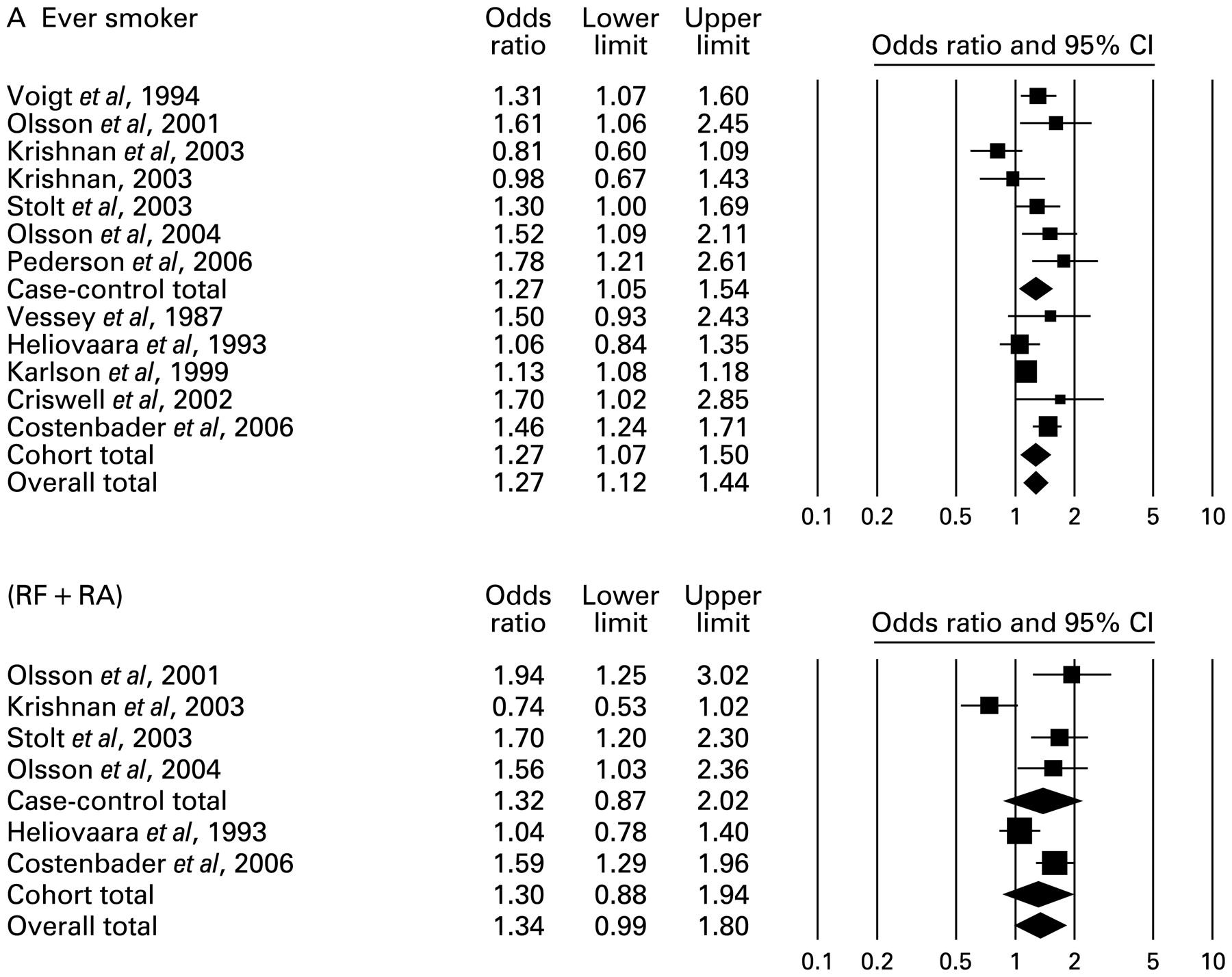
Subgroup analysis for female population (table 2B, fig 4)

Continued.

Continued.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The summary OR for ever, current and past female smokers were 1.27 (1.12 to 1.44), 1.31 (1.12 to 1.54) and 1.22 (1.06 to 1.40), respectively. For RF-positive RA, the summary OR for ever, current and past smokers were 1.34 (0.99 to 1.80), 1.29 (0.94 to 1.77) and 1.21 (0.83 to 1.77). Summary OR for 20 or more pack-years of smoking was 1.75 (1.52 to 2.02). Heterogeneities were statistically significant,but meta-regression analyses findings for smoking rate and study quality were not significant.
For the nine case–control studies,8 11 18 19 20 21 22 34 35 36 the summary OR for ever, current and past smokers were 1.27 (1.05 to 1.54), 1.19 (0.88 to 1.61) and 1.24 (1.04 to 1.48). Differences among the three categories of smokers were not significant. For RF-positive RA, the summary OR for ever, current and past smokers were 1.32 (0.87 to 2.02), 1.15 (0.57 to 2.31) and 1.21 (0.76 to 1.90). For RF-negative RA, the summary OR for ever, current and past smokers were 0.89 (0.64 to 1.21), 1.47 (0.87 to 2.49) and 0.87 (0.63 to 1.21).
For the five cohort studies,5 7 10 37 39 the summary OR for ever, current and past smokers were 1.27 (1.07 to 1.50), 1.37 (1.13 to 1.65) and 1.20 (0.96 to 1.49). Differences among the three categories of smokers were not significant. For RF-positive RA, the summary OR for ever, current and past smokers were 1.30 (0.88 to 1.94), 1.33 (0.94 to 1.90) and 1.24 (0.64 to 2.38). For RF-negative RA, the summary OR for ever, current and past smokers were 1.15 (0.74 to 1.76), 1.22 (0.93 to 1.56) and 1.29 (0.99 to 1.67).
The study quality of one female cohort study5 was lower than that of the others, but our results remained robust even after the exclusion of this low quality study.
Discussion
This is the first meta-analysis to examine the question of whether smoking is a risk factor for the development of RA, and our analysis clearly showed it is.
Our results indicate the risk of developing RA is approximately two times higher for male smokers than for non-smokers. For women, the risk for smokers is approximately 1.3 times greater than for non-smokers. However, for heavy smokers (20 or more pack-years of smoking), the risk was as high for women as for men. Although the results of previous studies5 7 11 18 20 34 35 did not show a significant relationship between smoking and the development of RA for women, our analysis provides quantitative evidence that smoking is an important risk factor for women in developing RA. We also demonstrated the risk for developing RA by smoking was not different for both men and women ever, current and past smokers. Finally, the difference between study designs was also not significant. We therefore thought the influence of these factors on our results were minor.
We determined that the risk of smoking for RA development is greater among men. Whereas the mechanism of hormonal effects on the development of RA is not clear, several biological and epidemiological studies investigated this issue.
Experimental studies have shown that oestrogen suppresses arthritis in an RA mouse model,46 47 and Salem48 found that oestrogen inhibited the production of T-helper type 1 pro-inflammatory cytokines such as tumour necrosis factor-alpha, which reduce the risk of RA development. In addition, oestrogen was shown to stimulate the production of anti-inflammatory cytokines such as IL-4. These cytokines play important roles in the development of RA by causing inflammation of synovial tissue.49 50
Moreover, epidemiological studies51 52 53 have suggested that factors related to oestrogen production, such as oral contraceptive use, significantly influenced the development of RA.51 52 53
To some extent, the discrepancy by gender may be the result of an artifact in that RA is inherently less common in men than women. However, the attributable risk proportion for men was found to be higher than that for women (2.1% vs 0.7%). The discrepant effect is attributable to gender as such and not to the difference in the prevalence of RA between men and women.
We also showed that the risk of developing RF-positive RA is greater than the risk of developing RF-negative RA and that this effect is modified by gender. Smoking is known to be associated with the production of RF.54 55 Although the molecular mechanisms connecting smoking and the development of RA have not been identified in detail yet, Padyukov et al22 investigated the interaction between smoking and RF and showed that HLA-DRB1 shared epitope alleles were a significant risk factor for the development of RF-positive RA only. In addition, the influence of HLA-DRB1 alleles was greater in the case of smokers. Our findings regarding the relation between smoking and RF-positive RA are compatible with these results. The modification by gender can be explained by the fact that production of RF may be affected by hormonal factors as well as smoking, so that the former may account for the gender-related differences in the effects of smoking on the development of RA.1
Another possible explanation for the discrepancy between genders can be found in occupational factors. For example, Stolt et al41 reported that silica exposure was associated with an increased risk of developing RA in men. However, the mechanisms by which silica affects RA progression have not yet been clearly established, and the overall risk of occupational exposure will need further study.
The difference in smoking intensity between men and women may also explain the risk difference in gender. However, among the studies reviewed, there was no significant difference in the smoking rate between men and women. Moreover, our results for pack-years of smoking suggest that heavy smokers, whether male or female, are at the same risk of developing RA. Therefore, the role of smoking intensity is likely to be minor.
The reason for the difference in the influence of smoking by gender might be due to a complex of several factors such as the hormonal effect, as mentioned above.
Some studies have recently reported anti-CCP was related to smoking habits and shared epitopes.36 56 57 Klareskog et al56 first demonstrated that smoking was a significant risk factor for CCP-positive RA, but not for CCP-negative RA, and that the presence of HLA-DRB1 alleles was linked to the occurrence of CCP-positive RA. These findings were re-confirmed in later studies.36 57 However, we could not conduct a subgroup analysis for CCP-positive RA because of a lack of data.
Westwood et al58 have suggested that RF-positive differ from RF-negative RA patients, and Klareskog et al59 also reviewed the evidence that CCP-positive and CCP-negative RA consists of two subsets of RA.
Our analysis has certain limitations. First, some of the studies selected for our meta-analysis also focused on other factors, such as the menopausal state, not only on smoking habits. These differences resulted in statistical heterogeneity among studies of female populations. Second, the selected studies were regionally restricted. All studies we found were performed in the USA and Europe, so that the validity of extrapolation of the findings to other regions is questionable.
Our results showed that any type of smoking constitutes a significant risk factor for the development of RA, especially for RF-positive RA men and smokers of 20 or more pack-years of smoking. Because RA is associated with a poor quality of life and life prognosis, we recommend cessation of smoking for current smokers, especially heavy smokers to prevent or reduce the risk of developing RA. Smoking is a preventable risk factor for the development of RA.
Acknowledgments
The authors would like to thank Drs Katsuyasu Saigo, Seiji Kawano, Takeshi Sugimoto and Chiyo Kurimoto for their helpful comments.
REFERENCES
Supplementary materials
Web Only Data 69/1/70
Footnotes
▸ Additional supplemental file is published online only at http://ard.bmj.com/content/vol69/issue1
Funding DS is supported by a Hyogo Science and Technology Association grant 18D022.
Competing interests None.