Article Text

Abstract
Objectives: To compare the efficacy of Disease Activity Score (DAS)-driven therapy and routine care in patients with recent-onset rheumatoid arthritis.
Methods: Patients with recent-onset rheumatoid arthritis receiving traditional antirheumatic therapy from either the BeSt study, a randomised controlled trial comparing different treatment strategies (group A), or two Early Arthritis Clinics (group B) were included. In group A, systematic DAS-driven treatment adjustments aimed to achieve low disease activity (DAS ⩽2.4). In group B, treatment was left to the discretion of the treating doctor. Functional ability (Health Assessment Questionnaire (HAQ)), Disease Activity Score in 28 joints (DAS28) and Sharp/van der Heijde radiographic score (SHS) were evaluated.
Results: At baseline, patients in group A (n = 234) and group B (n = 201) had comparable demographic characteristics and a mean HAQ of 1.4. Group A had a longer median disease duration than group B (0.5 vs 0.4 years, p = 0.016), a higher mean DAS28 (6.1 vs 5.7, p<0.001), more rheumatoid factor-positive patients (66% vs 42%, p<0.001) and more patients with erosions (71% vs 53%, p<0.001). After 1 year, the HAQ improvement was 0.7 vs 0.5 (p = 0.029), and the percentage in remission (DAS28 <2.6) 31% vs 18% (p<0.005) in groups A and B, respectively. In group A, the median SHS progression was 2.0 (expected progression 7.0), in group B, the SHS progression was 1.0 (expected progression 4.4).
Conclusions: In patients with recent-onset rheumatoid arthritis receiving traditional treatment, systematic DAS-driven therapy results in significantly better clinical improvement and possibly improves the suppression of joint damage progression.
Statistics from Altmetric.com
In patients with recent-onset rheumatoid arthritis, several combinations of disease-modifying antirheumatic drugs (DMARDs) or biological agents1 2 3 4 5 6 7 8 9 have proven superiority over initial monotherapy in improving clinical and radiographic outcomes. In the recently performed BeSt study,10 four different treatment strategies were compared in a setting of tight disease control. Patients treated with initial combination therapy with either prednisone or infliximab had a more rapid clinical response than patients treated with sequential monotherapy or step-up to combination therapy. After 1 year, changes in the physical function and the percentage of patients in clinical remission were comparable for all treatment groups. To achieve this, treatment had to be adjusted more often and for more patients in the initial monotherapy groups than in the initial combination therapy groups. We hypothesised that the systematic measurements of disease activity with adjustments to treatment according to a fixed protocol aiming at a Disease Activity Score (DAS) ⩽2.411 are the reasons for the remarkable improvement in the initial monotherapy groups after 1 year of follow-up.
To investigate this further, we compared the results of the patients receiving sequential monotherapy or step-up to combination therapy in the BeSt trial10 with the results of similar patients with rheumatoid arthritis who received routine care.
Patients and methods
Patients
All patients fulfilled the American College of Rheumatology 1987 criteria for rheumatoid arthritis.12 Group A consisted of patients participating in the BeSt study, who were treated with the traditional strategies—that is, sequential monotherapy (group 1) or step-up combination therapy (group 2). Inclusion criteria were as follows: age ⩾18 years, a disease duration ⩽2 years, ⩾6/66 swollen joints, ⩾6/68 tender joints and either an erythrocyte sedimentation rate (ESR) ⩾28 mm/h or a global health score ⩾20 mm on a visual analogue scale of 0–100 mm (0 = best, 100 = worst). Patients in the BeSt study were derived from two university and 18 peripheral hospitals in the western part of the Netherlands between April 2000 and August 2002. Group B consisted of all patients from the databases of the Early Arthritis Clinic of Leiden University Medical Centre (LUMC) and the Jan van Breemen Institute (JBI) in Amsterdam, who were diagnosed with rheumatoid arthritis and met the inclusion criteria of the BeSt study (see above). In the Early Arthritis Clinics, Disease Activity Scores of 28 joints, radiographs of hands, wrists and feet and several questionnaires are collected prospectively at regular intervals. During the inclusion period of the BeSt study, all eligible patients were enrolled in this study. For group B, all patients from the period before (January 1998–March 2000) and after the BeSt study (August 2002–December 2004) were included in this analysis.
Only patients with baseline and 1-year follow-up data of the Dutch version of the Health Assessment Questionnaire (HAQ),13 Sharp/van der Heijde score (SHS) for radiographic joint damage,14 or both, were included in this comparison. The DAS28 was not used as an inclusion criterion.
In total, 247 patients were included in the BeSt study in the initial monotherapy groups 1 and 2. For the current analysis we excluded 10 patients who withdrew within the first year of follow-up and an additional three patients, because of missing change scores for both HAQ and SHS.
Treatment
In group A, treatment adjustments were standardised and based on the DAS, obtained every 3 months, with the goal to achieve low disease activity (DAS ⩽2.4).15 Patients assigned to sequential monotherapy started treatment with methotrexate, followed subsequently, in the case of a persistent DAS >2.4, with sulfasalazine, leflunomide and methotrexate with infliximab. If the DAS was ⩽2.4 for at least 6 months, medication was tapered to the last established drug at a maintenance dose. Patients assigned to step-up combination also started treatment with methotrexate alone, followed subsequently, in the case of a persistent DAS >2.4, with methotrexate with sulfasalazine; methotrexate with sulfasalazine and hydroxychloroquine; methotrexate with sulfasalazine, hydroxychloroquine and prednisone; and methotrexate with infliximab. If the DAS was ⩽2.4 for at least 6 months, the last added drug was tapered first, until monotherapy at a maintenance dose remained. Parenteral corticosteroids were not allowed and low-dose oral corticosteroids were allowed only as described in the treatment protocol for the step-up combination group. A detailed description of the protocol has been published previously.10
In group B, treatment, including the use of corticosteroids and biological agents, was left to the discretion of the treating doctor.
Outcomes
In both treatment groups, assessments were made by research nurses every 3 months during the entire follow-up period. The primary clinical end point was functional ability, measured by the HAQ, with higher scores indicating more severe loss of physical function.13 The secondary clinical end point was the mean disease activity score in 28 joints (DAS28)16 and the remission percentage defined as DAS28 <2.6. The primary radiographic end point was the change from baseline to 1 year in the total SHS, ranging from 0 to 448.14 Radiographs of hands, wrists and feet, at baseline and at 1-year follow-up, were scored independently by two readers (JV and YG) blinded to the patient’s identity, treatment group and sequence of the films. The mean score of the two readers was used for the analysis. The intraobserver coefficients were 0.84 and 0.87 and the interobserver coefficient was 0.96. Erosive disease was defined as a mean erosion score >0.5. Progression of joint damage was defined as a change in total SHS greater than the smallest detectable change,17 which was 4.10. The predicted joint damage progression during the first year was extrapolated by dividing the baseline total SHS by the symptom duration. This extrapolation has been described previously in a study using the Larsen score for joint damage progression.18 Suppression of joint damage progression was defined as the median observed progression minus the expected progression.
Statistical analysis
All available data were used for the analyses. Measurements with a Gaussian distribution are expressed as mean and standard deviation (SD), and measurements with a non-Gaussian distribution are expressed as median and interquartile range (IQR). Outcomes of patients in groups A and B were compared, using the Student t test, Mann–Whitney U test and χ2 test, where appropriate. Linear regression analysis was used to describe the effect of the treatment group on the change in primary outcomes (HAQ and SHS), with 95% confidence intervals (95% CIs) with correction for the baseline differences: symptom duration, rheumatoid factor (RF) positivity, DAS28, baseline SHS and baseline HAQ. The DAS28 was used instead of the separate core set variables (tender and swollen joint count, ESR and visual analogue scale), because the databases provided different total joint scores and not scores per joint.
A subgroup analysis on the primary outcome measurements HAQ and SHS was performed using only the patients from the LUMC and JBI (93 patients in group A and all 201 patients in group B), using the Student t test and the Mann–Whitney U test, respectively.
Results
A total of 435 patients with recent-onset, active rheumatoid arthritis was included (234 in group A, 201 in group B). Group B consisted of 121 patients from the period before the initiation of the BeSt study and of 80 patients from the period after the BeSt study. HAQ scores were available for 228 patients (97%) in group A and 192 patients (96%) in group B, DAS28 scores were available for 232 patients (99%) in group A and 166 patients (83%) in group B, and baseline SHS was available in 229 patients (98%) in group A and 191 patients (95%) in group B.
Data for all other demographic and disease characteristics were available in over 98% of patients. Patients for whom data on DAS28 were missing had a lower median baseline SHS than patients in whom these data were complete (1.5 vs 3.0, p = 0.011). There were no other differences in baseline characteristics between patients with missing and complete data.
At baseline, the average age of patients was 54 years, 72% were female, the mean HAQ was 1.4, the mean DAS28 was 5.9 and the median SHS was 3.0. Patients in group A had a longer median disease duration than patients in group B (0.5 vs 0.4 year, p = 0.016), a higher mean DAS28 (6.1 vs 5.7, p<0.001) and a higher median ESR (39 vs 31 mm/h, p = 0.033). More patients in group A were RF positive (66% vs 42%, p<0.001) and more had erosive disease (71% vs 53%, p<0.001) in comparison with patients in group B (table 1).
Baseline demographic and disease characteristics
Clinical outcomes
Overall, clinical outcomes had improved after 1 year. The mean HAQ improvement was 0.6, the mean DAS28 improvement was 2.4 and the mean ESR decrease was 15 mm/h (table 2).
Change in patient outcomes during 1-year follow-up
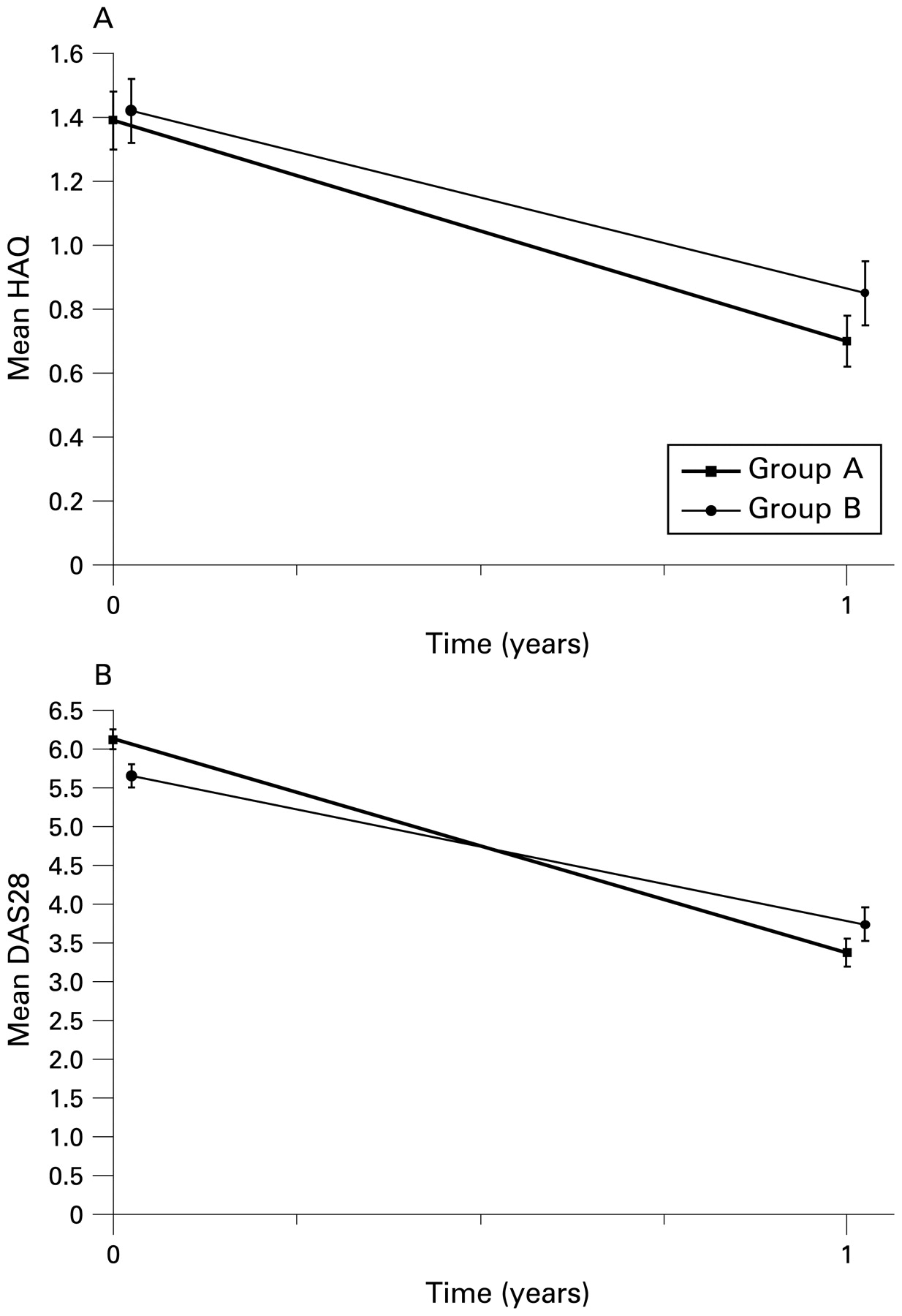
Despite higher baseline scores, patients in group A had better clinical outcomes after 1 year of follow-up than patients in group B. The mean HAQ improvement was 0.70 in group A versus 0.55 in group B (p = 0.029) (fig 1A), the mean DAS28 improvement was 2.7 in group A versus 1.9 in group B (p<0.001) (fig 1B) and the median ESR improvement was 19 mm/h in group A versus 13 mm/h in group B (p = 0.011). The percentage of patients in clinical remission (DAS28 <2.6) after 1 year was 31% in group A versus 18% in group B (p<0.005).

Mean Health Assessment Questionnaire (HAQ) and Disease Activity Score in 28 joints (DAS28) of the patients with DAS-driven therapy (group A) and routine care (group B).
In the linear regression analysis, the difference in HAQ improvement between the groups was 0.155 (0.015–0.294). After correcting for baseline differences in symptom duration, RF positivity, DAS28, SHS and HAQ, the difference in HAQ improvement was 0.143 (0.004–0.282), p = 0.044.
For the subgroup of patients from LUMC and JBI, patients treated with DAS-driven therapy had better clinical outcomes, but owing to the small sample size, no statistically significant differences were seen (data not shown).
Radiographic outcomes
Radiographs of hands, wrists and feet of 410 patients (94%) at both baseline and 1-year follow-up were available for analysis (224 patients in group A and 186 patients in group B). Based on the SHS score at baseline and the duration of symptoms at baseline, the expected progression of radiographic joint damage was calculated for patients in both groups. In group A, the expected progression after 1 year was 7.0, whereas the observed progression was 2.0. In group B, the expected progression was 4.4, whereas the observed progression was 1.0 (p<0.001 for expected progression, p = 0.006 for observed progression) (fig 2). The larger difference between the expected progression and observed progression in group A suggests that the suppression of joint damage progression was better in this group than in group B, although this was not statistically significant (p = 0.126).

{kind=link}
{kind=link}
Expected and observed progression of the Sharp/van der Heijde score (SHS) for radiographic joint damage for Disease Activity Score-driven therapy (group A) and routine care (group B).
In the linear regression analysis, the difference in the mean SHS progression was 2.32 (0.36–4.28) p = 0.020. After correcting for baseline differences in symptom duration, RF positivity, DAS28, SHS and HAQ, the difference in SHS progression was −0.42 (−2.23–1.40), p = 0.652—that is, in favour of the DAS-driven treatment group, but not statistically significant.
At baseline, significantly more patients in group A had erosive disease (group A 71%, group B 53%; p<0.001). After 1 year, the difference in percentage of patients with erosive disease was less distinct (group A 81%, group B 74%; p = 0.091).
Treatment
During the first year, more patients in group A than in group B had received DMARD therapy, including prednisone (100% vs 89%). The median (IQR) number of DMARDs per patient was 2.0 (1.0–3.0) in group A and 1.0 (1.0–2.0) in group B. In group A, all patients started with methotrexate. As dictated by the protocol, patients in group A switched medication if the DAS was >2.4, corresponding with a DAS28 >3.6. The following antirheumatic drugs were prescribed during the first year: sulfasalazine in 58% of patients, leflunomide in 20%, antimalarial drugs in 15%, low-dose prednisone in 7% and infliximab in 11% of patients. In group B, methotrexate had been prescribed in 54% of patients, sulfasalazine in 32%, prednisone in 21%, antimalarial agents in 19%, ciclosporin A in 3%, leflunomide in 1%, gold in 1%, etanercept in 1% and adalimumab in 1% of patients.
Discussion
This comparison of clinical and radiological outcomes in patients with recent-onset rheumatoid arthritis receiving traditional antirheumatic therapy shows that patients benefit from systematic monitoring of disease activity and standardised treatment adjustments compared with routine care. DAS-driven therapy adjustments result in significantly better clinical outcomes than routine management. These results are consistent with previous studies, which demonstrated that intensive management is more effective than routine care19 20 and that adherence to treatment guidelines improves outcome.21
Our observations are the result of comparing treatments for patients with recent-onset rheumatoid arthritis in the BeSt study (initial monotherapy with antirheumatic drugs) with a cohort of patients receiving routine treatment. We included all patients who would have met the inclusion criteria of the BeSt study within a period of 2 years before and after the inclusion period of the BeSt study from the Early Arthritis Clinics databases of the LUMC and the JBI, which were the main contributors of patients for the BeSt study. Nevertheless, when we compared the baseline characteristics, patients in the routine care group had a milder disease at baseline with fewer patients testing positive for RF, a lower disease activity and less radiographic joint damage than the patients in the BeSt study. The differences in baseline demographic and disease characteristics between patients in the BeSt study and patients in the routine care group were smaller when only patients included in the LUMC and JBI were analysed, suggesting selection bias in the BeSt study of patients with worse disease characteristics, which appears to be most common in the other participating (peripheral) centres.
A second important difference between group A and group B is the medication received. Despite the fact that both the LUMC and the JBI are specialised centres for patients with rheumatoid arthritis, patients in the routine care group less often received methotrexate, which is now considered to be the anchor drug in RA treatment.22 In part, this may be explained by milder disease characteristics in the routine group at the time of diagnosis. On the other hand, oral prednisone was prescribed more often, and low-dose steroids are effective in suppressing the rate of joint damage progression.23 24 25 Over time, novel insights might have influenced treatment choices in the routine care group, but the number of patients treated before and after the inclusion period of the BeSt study was too small to find significant differences in drug prescription patterns.
In our opinion, the differences between the two groups only increase the strength of the observation that despite a worse prognosis patients treated in the BeSt study with DAS-driven therapy show more clinical improvement than patients receiving routine care, who had a better initial prognosis and more often received oral corticosteroids.
At baseline, significantly more patients in the DAS-driven group had erosive disease. During the first year, more patients in the routine care group progressed from non-erosive to erosive disease, resulting in a comparable percentage of patients with erosive disease after 1 year of treatment. Furthermore, the rate of progression after 1 year appears to be better suppressed in the DAS-driven group than in the routine care group, although one might argue that this is the result of regression to the mean. The differences in disease severity at presentation and drug prescription probably explain why we did not find a statistically significant difference between the groups.
We conclude that systematic DAS-driven therapy results in better improvement of clinical outcomes and results in good suppression of joint damage progression.
Acknowledgments
We thank all patients, all rheumatologists and trainee rheumatologists who participated in the BeSt study and/or the Early Arthritis Clinic, and all research personnel for their contribution to this article.
REFERENCES
Footnotes
Funding This study was funded by a grant from the Dutch College of Health Insurances (College Voor Zorgverzekeringen) with additional funding provided by Schering-Plough, BV and Centocor.
Competing interests CFA and FCB have received lecture fees from Schering-Plough; BACD has received funds for research and lecture fees from Schering-Plough.
Ethics approval Ethics committee approval from all participating centres.
Patient consent Patient consent received.