Article Text

Abstract
Background: Uric acid lowering therapy (UALT) is considered a chronic treatment for gout. Relatively little is known about adherence to UALT.
Methods: We assessed adherence with UALT over a 1-year study period among 9823 older adults enrolled in a pharmacy benefit program. Two adherence measures were calculated, the percentage of days covered (PDC) and the time until an extended break (at least 60 days) in treatment. A PDC <80% was considered poor adherence and its predictors were examined in multivariable logistic models.
Results: The mean (SD) PDC was 54% (36%) with 64% of patients considered poorly compliant over the study period. A total of 56% had experienced an extended break in UALT. Predictors of poor adherence included younger age (odds ratio (OR) 1.50, 95% CI 1.33–1.69 for ages 65–74 compared with 85 and above) and African–American race (OR 1.86, 95% CI 1.52–2.27 compared with Caucasian race). Most patients (93%) received their initial UALT prescription from a non-specialist and this also predicted poor adherence (OR 1.15, 95% CI 0.96–1.38 compared with rheumatologists or nephrologists).
Conclusion Adherence with UALT is poor. While uric acid levels were not measured in this study, poor adherence with UALT is likely to reduce attainment of goal uric acid levels.
Statistics from Altmetric.com
Gout is characterised by acute and/or chronic arthritis related to hyperuricemia. Complications of gout include tophi, interstitial nephritis, and nephrolithiasis. Recent studies have also suggested a link between hyperuricemia and cardiac disease, possibly resulting in congestive heart failure.1–3 There is general agreement that uric acid lowering therapy (UALT) should be reserved for patients with acute gout attacks, chronic gouty arthritis, tophi, interstitial nephritis, or uric acid containing nephrolithiasis.4 5 Most experts recommend that once treatment with UALT has begun it should be continued for life, or at least for a year after uric acid levels are in the low normal range.5 6
While other investigators have pointed out that not all care of gout is optimal, relatively little is known about patterns of use of UALT.7 One prior study among a US managed care population found that approximately half of patients diagnosed with gout receive UALT.8 Moreover, once UALT has begun few patients in managed care remain on treatment chronically.9 10 We examined the patterns of adherence with medications used to lower uric acid among a group of older adults participating in a pharmacy benefits program.
METHODS
Design
We assembled a cohort of patients who were simultaneously enrolled in the US Medicare system and a pharmacy benefit for older low-income adults in the state of Pennsylvania, the Pharmacy Assistance Contract for the Elderly (PACE). Patients must have been new users of allopurinol, probenecid, or sulfinpyrazone (any of the three UALTs available in the US). The cohort was then followed for 12 months after initiating a UALT to assess adherence with the regimen, dosing of UALTs, and use of concomitant anti-inflammatory drugs.
The Partners Institutional Review Board approved the study protocol. The analyses and manuscript were reviewed by the study sponsor. All final decisions regarding analyses and manuscript preparation were made independently by the authors.
Study population
Patients 65 years of age or older who were simultaneously enrolled in Medicare and PACE were eligible for this study. We required patients to have system use in Medicare and PACE in two consecutive 6-month periods prior to filling a prescription for a UALT. To better assess adherence with UALT, we restricted our analyses to patients who initiated treatment with one of these drugs. Thus, patients were required to not have used any UALTs for 12 months prior to cohort entry. Since UALT can be indicated in patients at risk of tumour lysis syndrome, those with a history of a lymphoma or leukaemia were excluded. The study period began with the first filling of a UALT medication and ended after 12 months, or the first of any of the following events: loss of PACE eligibility, nursing home admission, or death.
Adherence measures
We assessed the daily use and persistence of use for UALT. Daily use was measured as the percentage of days covered (PDC), a measure almost identical to the Medication Possession Ratio (MPR).11 This was calculated as the days with available UALT divided by the total number of days of follow-up. We determined the days with available UALT based on the pharmacy filling records, including the number of days supplied and number of pills dispensed fields. As has been peformed in many prior studies, the PDC was dichotomised at 80% for multivariable analyses, with <80% PDC considered non-adherence. Persistence with UALTs was assessed as the time until an extended break in treatment. This was measured as the number of days with available medications until the first 60-day period without any UALT available.
Covariates
Patient and physician characteristics were assessed as potential correlates of adherence. Patient covariates were defined using health care utilisation data from the 12 months prior to the index date. These included sociodemographic factors (age, gender, race), medical care intensity (number of physician visits, number of different medications used, number of acute care hospitalisations), comorbid conditions,12 and gout specific factors. These factors consisted of: the number of acute gout arthritis diagnoses; a diagnoses of nephrolithiasis; a diagnosis of tophi; a diagnosis of interstitial nephritis; the use of selective or non-selective non-steroidal anti-inflammatory drug (NSAID), colchicine, or glucocorticoids (oral, intra-articular, or intra-muscular); and uric acid measurements.
In addition, using the medical license number on the index prescription, we identified the physician who prescribed the first UALT to determine if s/he was a specialist (defined as rheumatologist or nephrologists) or a non-specialist. This field has been found to accurately identify the prescribing physician.13
Analysis
We first described the study characteristics of the study population. This was done for the whole cohort as well as by gender. The dosing for allopurinol was examined in detail, comparing starting and maximum daily dosages for specialists and non-specialists. The PDC was examined by medication. We then dichotomised the percentage of days covered at 80% and assessed correlates of non-adherence (<80% of days covered) using adjusted logistic regression. A backward selection routine was used to determine the variables to include in the multivariable models. All covariates were considered potentially important and initially entered in the models. Only variables with p values <0.10 remained in the final models. Finally, persistence of use was examined using Kaplan–Meier survival plots, stratified on key factors, including gender, age, gout or any of its complications (tophi, nephrolithiasis, or interstitial nephritis), specialty of the index prescriber (the physician who wrote the initial UALT prescription), and type of UALT. Restricted analyses were run in the cohort of patients with a diagnosis of gout. All analyses were run using SAS (Cary, North Carolina, USA).
RESULTS
Among the 9823 patient studied, the mean age was 79 years and 72% were female (table 1). This reflects the gender distribution of PACE, which is approximately 84% female. The vast majority of patients were Caucasian. On average, patients had 11 visits to any physician in the 12 months prior to the study year and received 11 different medications. The minority of patients received a diagnosis of acute gout in the year prior and few patients were noted to have tophi, uric acid nephrolithiasis, or interstitial nephritis. Almost half of these patients had received a prescription for a selective or non-selective NSAID, approximately 10% received colchicine, and 12% received glucocorticoids. These characteristics did not differ by gender.
The UALT was prescribed by a non-specialist in 93% of patients and almost all prescriptions were for allopurinol. Two-thirds of the index prescriptions were for monotherapy while one-third was for combination of UALT with an NSAID, colchicine, or glucocorticoids. The dosing of allopurinol was similar between specialists and non-specialists (table 2). The vast majority of patients started with dosages between 100–400 mg/day. Maximum dosages were slightly higher than starting dosages suggesting upward dosage titration. Few patients were given 400 mg or higher of allopurinol on a daily basis.
The PDC was on average 54% (SD 36%). A total of 64% of patients had a PDC of less than 80%, 56% had less than 65% of days with a UALT, and 46% had less than 50% of days covered. These analyses were re-run in the 1391 patients with a known history of acute gout and the mean (SD) PDC was also 54% (35%). As well, it was re-run in the 10 124 patients who started allopurinol and, again, it was 54% (36%).
We examined the correlates of non-adherence (percentage of days covered <80%; see table 3). Gender was not an important correlate of non-adherence, but younger age (OR 1.50, 95% CI 1.33–1.69 for ages 65–74 compared with 85 and above) and African–American race (OR 1.86, 95% CI 1.52–2.27 compared with Caucasian race) significantly increased the probability of non-adherence. Fewer prior acute care hospitalisations, fewer concomitant prescriptions, and fewer comorbid conditions were also correlated with non-adherence. No record of tophaceous gout was the only gout factor associated with non-adherence. In addition, no prior colchicine was associated with non-adherence. Patients who received their UALT prescription from a generalist had a higher probability of becoming non-adherent (OR 1.15, 95% CI 0.96–1.38) compared with rheumatologists or nephrologists.
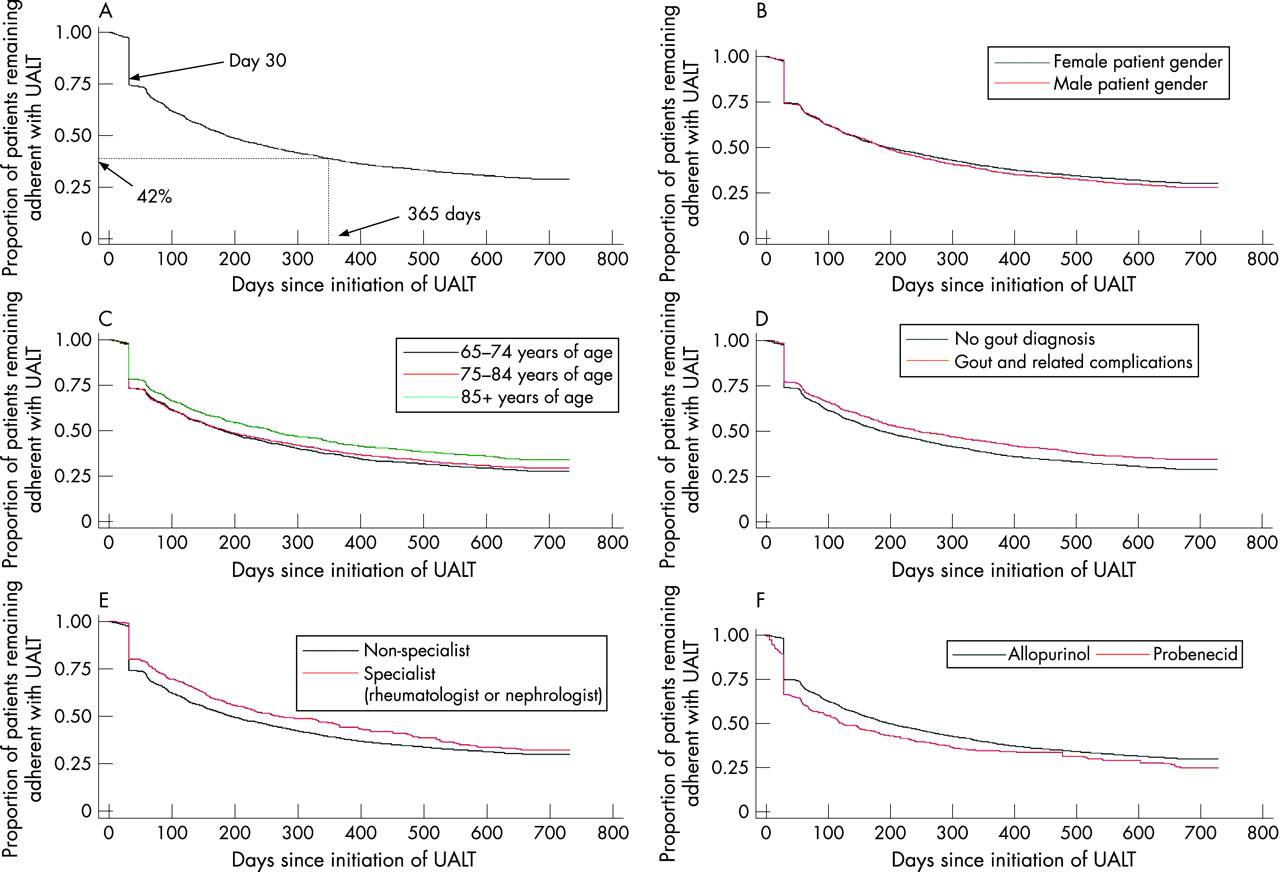
We plotted the survival distribution of the time until an extended break occurred for all patients and by subgroups (fig 1A–F). These plots show that about one-quarter of patients have an extended break in treatment after their first prescription and by 365 days, 56% have had an extended break in therapy. The gender stratified plot (fig 1B) showed no difference between men and women. When stratified by age, older patients had greater long-term persistence than younger patients (log rank p value <0.05; fig 1C). We also observed that patients with a history of gout or its complications (such as tophi) had better long-term persistence than those without such complications (log rang p value <0.05; fig 1D). A similar trend existed for patients receiving their first prescription for a UALT from a specialist compared with a generalist (log rank p value <0.05; fig 1E). Finally, we examined allopurinol separately from probenecid and found similar patterns of adherence (fig 1F).

{kind=link}
DISCUSSION
We studied the patterns of use of UALT among a cohort of older US Medicare beneficiaries, most of whom are female. During a 1-year study period, we observed poor adherence and more than half experienced an extended break in treatment. There were several strong correlates of non-adherence including younger age and African–American race. Patients receiving their index prescription from a non-specialist also appeared less likely to remain adherent. The dosing of allopurinol appeared to be titrated upward after initiation, but few patients received over 400 mg daily. These trends were consistent across genders in our study cohort.
Our study cohort was primarily comprised of women, not typical for a study of gout. However, the source population for this study is approximately 84% female and thus our female predominance would be expected. The gender-specific analyses argue that the trends in adherence were similar across genders. Moreover, recent data suggest that women make up a large portion of the older age gout population.8 Also, many subjects in our cohort did not have a known diagnosis of gout. Since hyperuricemia without gout is not an indication for UALT, treatment discontinuation would not be a problem in such a group. However, in analyses restricted to patients with a diagnosis of gout, we also found very low adherence.
The poor adherence with UALT is concerning in light of the recommendations by many experts that once begun, most patients should continue treatment for life if they have gout.5 6 The pattern of use that we observed suggests that a minority of patients are consistently using these medications by 1 year after initiation. The degree of non-adherence to UALT is worse than what has been observed for several other chronic conditions, including hypertension, depression, and hyperlipidaemia.14–16 The low degree of adherence observed in our study suggests that effectiveness of UALT as used in usual care settings may be considerably less than the efficacy demonstrated in RCTs. However, our reliance on a PDC of less than 80% is arbitrary and may not correlate with disease control in gout.
It is useful to compare these results with those of prior studies of gout medication adherence.9 10 While the three studies used slightly different definitions of adherence, all three found that approximately 50% of patients remained adherent with UALT during follow-up and that older age was associated with a higher likelihood of being adherent. None of the studies identified patient characteristics that accounted for much of the variation in adherence. One, but not both, of the prior studies found that men were less likely to be adherent.9 The present study did not find that gender was an important correlate of adherence. We also did not find that the gout related factors were important predictors of adherence, while one prior study found that a gout flare prior to measurement of a uric acid level correlated with poor adherence.10
While some of the patients in our cohort may not have had a prior diagnosis of gout, clinicians treating patients for gout should be aware that adherence to UALT is often poor. Prior to initiating UALT for gout, physicians should stress to their patients the need for continuous medication use and inquire about regular UALT use during follow-up appointments. Furthermore, factors like race and age that are correlates of poor adherence are easily identified markers that might be used to alert physicians and health care systems that a patient is at particular risk of non-adherence. Interventions designed to improve UALT adherence should be broad-based as well as targeting the at-risk patients we identified.
Our study is limited by the types of information we have regarding patient correlates of adherence. In health care claims data there is not good information on many social and psychological issues that are related to medication adherence.17 In addition, our study population is mostly women. However, the gender-stratified analysis suggested that there was little difference in adherence by gender. Since gout is considered a disease affecting men more frequently than women, this limitation is important to note. It would also be important to understand whether gout-related symptoms are associated with adherence. Our study database does not allow for assessment of symptoms, uric acid levels, or synovial fluid crystal examinations. We also cannot determine whether patients become non-adherent because of adverse events or other patient-related factors. However, all patients in this study cohort are beneficiaries of a generous drug benefit and thus financial access is unlikely to be a major reason for non-adherence. The goal of UALT is to lower the uric acid to the normal range for a prolonged period. The study database does not contain uric acid levels, so we are unable to determine whether the goal uric acid was achieved. However, it appears that few patients underwent follow-up uric acid testing during the study period. Finally, a major limitation of our study database is that some patients may not have gout but only an elevated uric acid level. The indications for UALT in such patients is unclear, possibly contributing to low adherence rates. However, subgroup analyses focused only on patients with a prior gout diagnosis showed results very similar to the parent analysis.
While poor adherence is not a new issue, the extremely low levels of long-term adherence with UALT we observed were surprising. Chronic gout with hyperuricemia is treatable in most patients. However, the majority of patients in our study sample, if they have gout, do not remain on UALT long enough to achieve adequate uric acid reduction. There has been at least one observation that patients who remain adherent with UALT have improved outcomes.8 Future research should explore the benefits of uric acid lowering in long-term randomised controlled trials. Long-term uric acid reduction will likely reduce the known complications of gout.
REFERENCES
Footnotes
Funding: Savient Pharmaceuticals Inc. supported this study.
Competing interests: None declared.