Article Text

Abstract
Background: Antibodies targeting citrullinated antigens are specific for rheumatoid arthritis (RA). Citrullination is catalysed by the peptidylarginine deiminase (PAD) enzyme family. Critical enzymes are often targeted by disease-specific antibodies in complex immune-mediated diseases. Here, we have tested for autoantibodies against human recombinant PAD4 (hPAD4) in Caucasian RA patients.
Methods: A time-resolved fluorometric immunoassay based on hPAD4 was developed to analyse sera from two RA cohorts (n = 237 and n = 177), one systemic lupus erythaematosus (SLE) cohort (n = 84) and 148 healthy controls. Simple and multiple analyses were performed to examine possible associations between anti-hPAD4 and disease variables.
Results: Raised levels of anti-hPAD4 IgG were found in both RA cohorts compared to the controls, and 23% of the RA patients were anti-hPAD4 IgG positive. Anti-hPAD4 was associated with anti-cyclic citrullinated peptide (CCP) and rheumatoid factor (RF), as well as increased physical disability. Anti-hPAD4 was also associated with higher longitudinal radiographic damage scores and increased clinical joint pathology, but weaker than anti-CCP. No associations were found between anti-hPAD4 and selected Human leukocyte antigen (HLA)-DRB1 variants.
Conclusions: Approximately 23% of Caucasian RA patients have serum IgG antibodies against hPAD4.The presence of serum anti-hPAD4 IgG was in simple analyses associated with a more severe disease phenotype, and the association with physical disability was maintained in multiple analyses.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) has a multifactorial aetiology, and is typically classified as a complex immune-mediated disorder. The distinct immunological features of RA include clear Human leukocyte antigen (HLA)-associations, T cell infiltration of the target organ and disease-specific antibodies against citrullinated proteins generated in vivo by the peptidylarginine deiminase (PAD) enzyme family.1
The disease-specific antibodies against citrullinated proteins are routinely detected by the cyclic citrullinated peptide (CCP) assay. Studies using anti-CCP suggest that anti-citrullinated protein antibodies (ACPA), rather than being a consequence of inflammation, is directly involved in the disease process: Anti-CCP may precede development of RA, is associated with severe RA and is linked to the HLA-association in RA (reviewed in Zendman et al).2 Many endogenous proteins have been put forth as candidate ACPA targets, but the real in vivo antigens remain unidentified.
Currently, five human PAD isoforms (PAD1–4 and PAD6) are identified.3 Recent data suggest PAD4 as an isoform involved in RA. First, PAD4 is expressed in synovial immune cells.3 Second, PAD4 co-localises with citrullinated proteins in the inflamed joints.4 Third, a genetic association between RA and PAD4 is observed in different populations.5 Fourth, disease-specific serum antibodies against human recombinant PAD4 (hPAD4) were recently identified in Japanese RA patients.6 Interestingly, a similar immune-targeting of enzymes involved in disease pathogenesis is also seen in other complex immune-mediated disorders.
In this study we aimed to: (1) develop a sensitive and accurate assay for the detection of anti-hPAD4 IgG in RA sera and compare responses to systemic lupus erythaematosus (SLE) and control sera; and (2) evaluate if anti-hPAD4 is associated with HLA-DR, rheumatoid factor (RF), anti-CCP, disease activity and outcome, and investigate if such associations provide new clues about the role of PAD4 in the RA pathogenesis.
MATERIALS AND METHODS
Patients and sera
Serum samples were obtained from two previously described Norwegian RA cohorts (RA1 and RA2). RA1 is the previously described European Research on Incapacitating Diseases and Social Support (EURIDISS) cohort,7 consisting of 237 patients. Serum was analysed for anti-CCP2 by an INOVA diagnostics kit (San Diego, California, USA), with a maximum value of 251 U/ml and 25 U/ml as positive cut-off. Radiographic damage was scored at baseline and at 1, 2, 5 and 10 years according to the van der Heijde modified Sharp (vdH Sharp) method.8 RA2 consists of 177 patients (aged 24–70 years, mean 56 years) with a disease duration up to 41 years (mean 13.5 years), selected from the Oslo RA register,9 based on Modified Health Assessment Questionnaire (MHAQ) scores ⩾1.5 at sampling time. Anti-CCP2 was detected with the DIASTAT kit (Axis-Shield Diagnostics, Dundee, UK), with a maximum value of 100 U/ml and 5 U/ml as positive cut off. HLA-DRB1 genotyping was available for 208 and 150 patients in RA1 and RA2 respectively.
The SLE cohort consisted of 84 patients (aged 18–83 years, mean 45 years),10 whereas the control group contained 148 healthy individuals (124 females and 24 males, aged 51–76 years, mean 64 years), randomly selected from the population register after matching for age, sex, and residential area with patients in the Oslo RA register.
Expression of human recombinant PAD4
The full-length hPAD4 cDNA was provided by Dr M. Yamada (Graduate School of Integuated Science, Yokohama City University, Yokohama, Japan), expressed as a fusion protein with the 26 kDa glutathione S-transferase and purified as described previously.11 PAD activity was assessed by a colourimetric assay.11
Anti-PAD4 antibody assays
100 μl active hPAD4 (5 µg/ml) in Tris buffered saline (TBS) with 5 mM CaCl2, pH 7.5 were incubated over night at 4°C on microtitre plates. After blocking with 1% BSA (1 h, 37°C), 100 μl serum diluted 1:2000 in TBS-T (TBS with 0.1% Tween 20) was added to duplicate wells (1.5 h, 37°C) before rabbit anti-human IgG (1:10000) was added (1 h, 37°C). Next, biotinylated goat anti-rabbit IgG (1:8000) was added (1 h, 37°C). Plates were washed with TBS-T between each step. Finally, Europium-labelled streptavidin was added and the assay developed according to the manufacturer’s instructions (Wallac, Turku, Finland). Anti-hPAD4 responses were calculated by subtracting the mean background signal (buffer only) from the mean anti-hPAD4 signal.
Liquid-phase inhibition assays
Pooled sera from five RA patients with high levels of anti-hPAD4 IgG were pre-incubated with liquid-phase hPAD4 before applying to microtitre plates. Binding of anti-hPAD4 IgG to solid-phase hPAD4 was inhibited >80% by 50 µg/ml of soluble hPAD4 (see Supplementary data).
Statistical analyses
Analyses were performed with SPSS v14 (SPSS Inc., Chicago, Illinois). Due to skewed distribution of the anti-hPAD4 responses, logarithmic transformation was performed before analyses by Student t test. Anti-hPAD4 positive and negative samples were compared by Pearson χ2 test, Student t test or Mann–Whitney U test. Marginal modelling by generalised estimating equations (GEE)12 was used to study longitudinal radiographic damage and the annual progression as dependent variables, and RF, anti-CCP and anti-hPAD4 as independent variables. Multiple regression analyses were performed to evaluate independent effects on C-reactive protein (CRP), MHAQ and joint counts. p Values <0.05 were considered statistically significant.
RESULTS
Serum anti-hPAD4 IgG in RA, SLE and controls
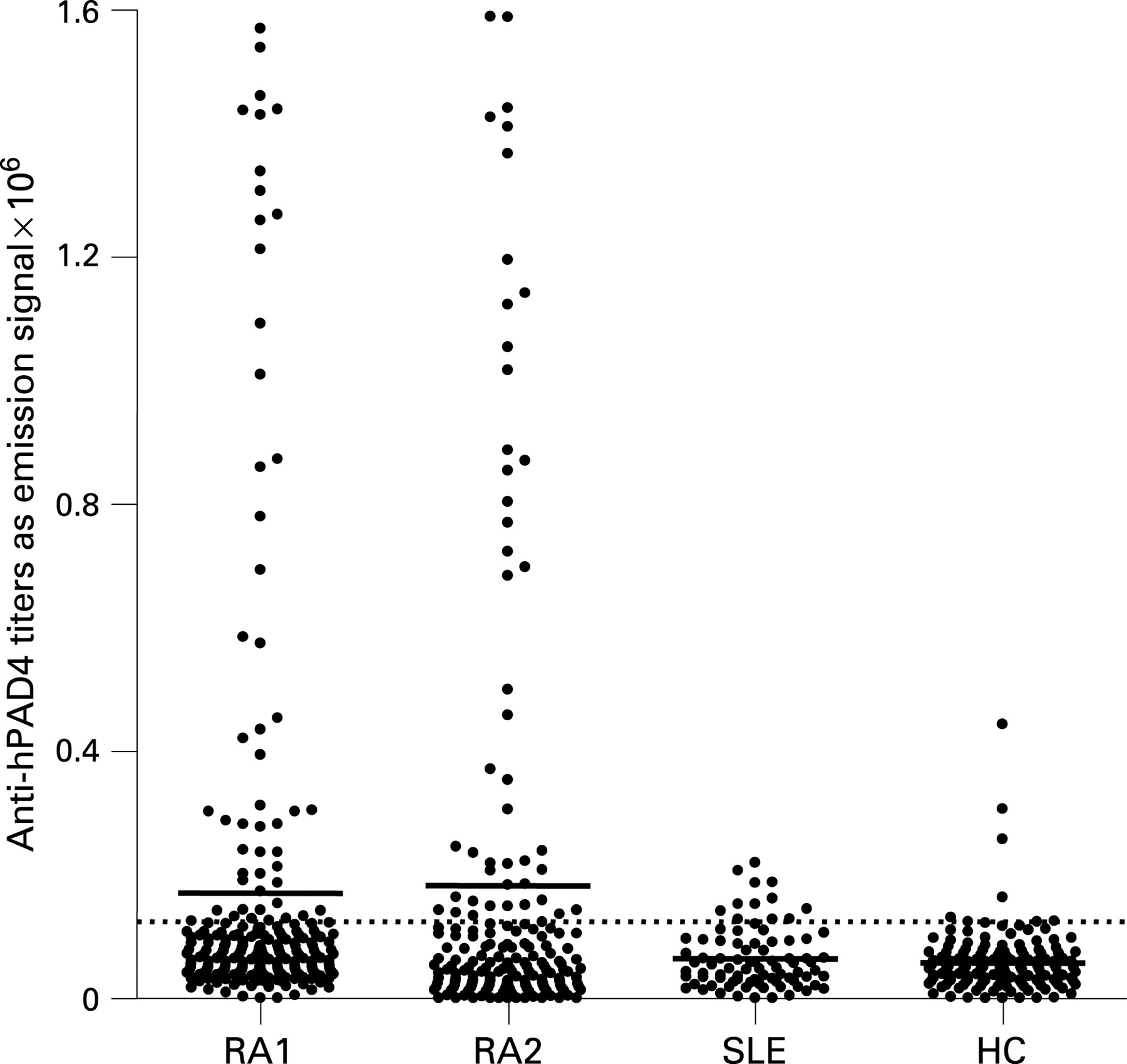
Serum anti-hPAD4 IgG was detected in 51 patients (22%) in RA1 and 45 patients (25%) in RA2 (fig 1). Anti-hPAD4 IgG levels were higher in RA1 and RA2 than in the controls and in the SLE cohort. Although 12 SLE patients (14%) were anti-hPAD4 positive, the mean emission signal in the SLE cohort did not differ from the controls. In RA1, anti-hPAD4 was associated with longer disease duration at baseline (table 1).
Associations with other variables and radiographic joint damage
Anti-hPAD4 IgG was positively associated with anti-CCP and RF in both RA cohorts (table 1). The anti-hPAD4+ patients also had higher CRP levels than anti-hPAD4– patients (table 1), but multiple regression analysis showed that this association was secondary to anti-CCP (data not shown).
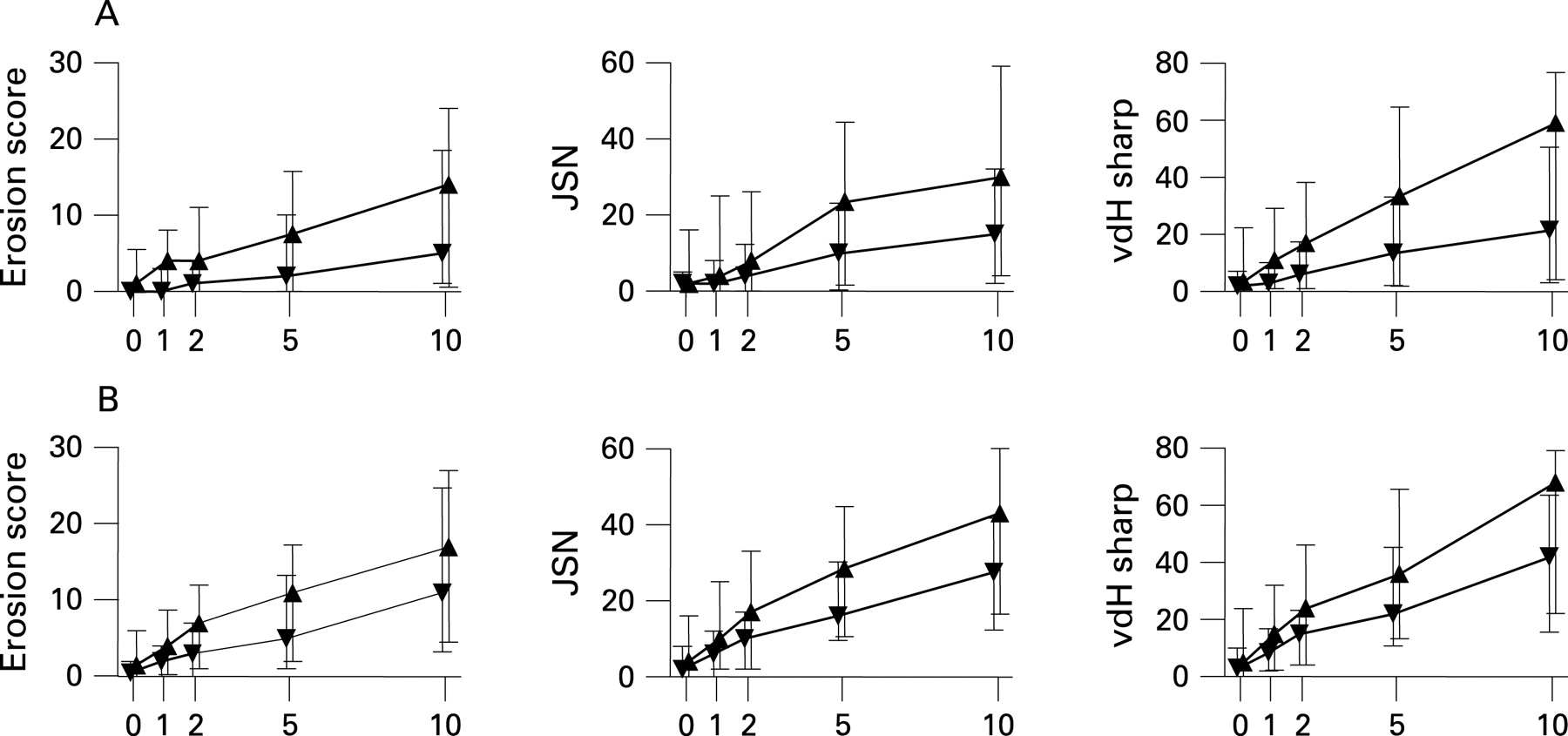
Radiographic damage scores were calculated by GEE and expressed by subgroups positive and negative for RF, anti-CCP or anti-hPAD4 in RA1. Anti-CCP was recently found to predict radiographic progression in RA1.13 Anti-hPAD4 was associated with higher average longitudinal radiographic damage, but weaker than RF and anti-CCP (see Supplementary data). We observed that anti-hPAD4+ patients had a trend towards higher radiographic damage scores over time, even in the presence of anti-CCP (fig 2). In contrast to anti-CCP, anti-hPAD4 was not positively associated with the shared epitope or negatively associated to HLA-DRB1*0301 (see Supplementary data).
{kind=link}
{kind=link}
Associations with physical disability and clinical joint pathology
Increased MHAQ scores and higher swollen and deformed joint counts were associated with anti-hPAD4 in RA2 (table 1). Multiple regression analyses using disease duration, RF, anti-CCP and anti-hPAD4 as independent variables confirmed an independent association between anti-hPAD4 and increased MHAQ scores and borderline significant associations between anti-hPAD4 and higher swollen and deformed joint counts (see Supplementary data).
DISCUSSION
Here, we have tested whether hPAD4, an enzyme implicated in the generation of citrullinated epitopes in RA, is in itself a target for RA-specific serum antibodies. Our data show that RA patients have higher anti-hPAD4 IgG levels than SLE patients and controls, and that anti-hPAD4 was positively associated with anti-CCP, RF and physical disability in RA.
In the previous study on anti-hPAD4 in RA serum, anti-hPAD4 IgG was reported in 21 out of 42 Japanese RA patients.6 The higher frequency of anti-hPAD4 in that study may be due to differences in disease phenotype or genetic background. Two publications have reported high frequencies of serum antibodies to purified rabbit PAD2 in RA patients.14 15 In our opinion, these studies are difficult to judge since rabbit PAD2 is not sequenced and therefore cannot be compared with the human isoforms.
Although our data does not allow for conclusions about anti-hPAD4 and clinical phenotype, some observations indicate an association with severe RA. First, anti-hPAD4 was associated with disease severity in patients with MHAQ ⩾1.5. Second, anti-hPAD4 was associated with longitudinal radiographic damage, but weaker than RF and anti-CCP.
Anti-hPAD4 proved to be strongly associated with anti-CCP. This association possibly reflects the possibility that the production of both antibodies could be driven by the same CD4+ T cell. Complexes of PAD4 and its substrate could act as hapten-carrier complexes and bind to the Ig-receptor of B cells either specific for PAD4 or the citrullinated substrate. Both these B cells would process the PAD4/citrullinated substrate complex and present the same epitope to a specific CD4+ T cell. It is also possible that anti-PAD4 IgG may increase the load of citrullinated B cell epitopes, either by increasing the citrullinating activity of PAD4 or by inducing apoptosis and thereby citrullination in synovial cells. In addition, PAD4 released from dying cells may act as a danger signal affecting innate immunity.
Although mean anti-hPAD4 IgG levels in the SLE cohort was similar to the controls, 14% of the SLE patients were anti-hPAD4 positive. It is possible that this finding reflects that SLE patients in general generate autoantibodies to a wide range of nuclear constituents.
This study is the first to assess anti-hPAD4 in Caucasian RA patients and associations with disease variables. Our results show that serum anti-hPAD4 is rather infrequent, but that it may contribute to a more severe disease phenotype in RA. It is possible that the low frequency of serum anti-hPAD4 IgG reflects that these autoantibodies, as others,16 primarily bind their substrate locally and never reach the bloodstream. Further studies are clearly required to unravel the roles of PAD4 and the significance of anti-hPAD4 in RA.
Acknowledgments
We thank Ludvig M Sollid, Benedicte A Lie and Silje W Syversen for critical reading of the manuscript.
REFERENCES
Supplementary materials
web only appendices 67/3/414
Files in this Data Supplement:
- view PDF 7 KB -
Supplementary figure 1
Dose-dependent inhibition of serum anti-hPAD4 IgG binding to solid-phase hPAD4 by incubation with liquid-phase hPAD4. Human albumin was used as a control inhibitor. A pool of five anti-hPAD4 positive RA sera diluted 1:2000 in TBS-T was incubated for 1 hour at 37�C with equal volumes of hPAD4 (▲) or human albumin (▼) in increasing concentrations. Serum pools were then applied to the microtiter plate after the blocking of the plate with 1% BSA. - view PDF 1 KB
- view PDF 7 KB -
Supplementary figure 1
Footnotes
Additional data are published online only at http://ard.bmj.com/content/vol67/issue3
Funding: This work was supported by grants from Rikshospitalet University Hospital and the Research Council of Norway. EHH was financed by a PhD stipend from the University of Oslo
Competing interests: None.