Article Text

Abstract
Objectives: To obtain data on the care received by individuals counselled during a public health awareness campaign on painful musculoskeletal conditions (MSC).
Methods: Easy non-formal access to rheumatologists/pain specialists was offered using a mobile unit (Rheuma-Bus) at widely accessible sites. Clients were asked to assess their severity of pain using a 100 mm visual analogue scale (VAS). Age, gender, disease duration, diagnosis if known, current and previous treatment as well as tentative diagnoses assigned and recommendations given to each individual by the counselling physicians were recorded.
Results: Average (SD) VAS pain rating was 59 (20.6) mm. Approximately 40% of clients had never consulted a physician for their condition before, but had lower pain scores than those who had seen a physician. Patients with inflammatory MSC had higher pain scores than those with non-inflammatory conditions. More than 2% of the clients had a newly detected inflammatory rheumatic disease.
Conclusions: Many individuals having painful MSC seek medical help only when a very high threshold of pain is reached. Even while under treatment, the high mean pain scores suggest neglect of MSC that are not adequately recognised as important contributors to disability and decreased quality of life.
- MSC, musculoskeletal conditions
- RA, rheumatoid arthritis
- VAS, visual analogue scale
Statistics from Altmetric.com
Musculoskeletal conditions (MSC) constitute major health and societal burdens as recognised recently by the UN and WHO by endorsing 2000–2010 as the “Bone and Joint Decade”.1 The health burden conferred by rheumatic diseases has been recently summarised by the WHO,2 and the societal burden can be appreciated from the fact that MSC are the main causes of sick leave and disability pension.3 Prevalence of MSC among adults approximates 30% and increases with age.4 With increasing life expectancy, their importance will also increase and good care will become more necessary than ever.
Good care depends on both access to specialists and awareness of particular conditions by patients and physicians. Access requires availability (numbers) and proximity (geographical and administrative) of specialists. Awareness depends on information provided to physicians and the public. Since MSC are primarily characterised by pain,5 which in turn is the major determinant of disability in these patients,6 one should assume that patients with MSC would readily seek physicians’ diagnostic and therapeutic advice. However, contrasting such seemingly obvious expectations, MSC are widely neglected by the public and by many affected individuals.7
In the context of Europe-wide awareness activities of the European League Against Rheumatism and its campaigning arm, the Alliance Against Arthritis, (http://www.eular.org/index.cfm?framePage=/international_AAA.cfm) and the middle of the Bone and Joint Decade,1,8 the Austrian Rheumatology Society launched an initiative providing easy, non-formal, free access to counselling by rheumatologists or pain specialists. A mobile unit (an adapted broadcast bus) was parked at easily accessible sites allowing passers-by to step in, talk to a specialist and receive information and further guidance.
In this report, we summarise the data obtained by the assessments, which are probably valid in other European countries and should have a major impact on European awareness activities and policy makers.
PATIENTS AND METHODS
Rheuma-Bus
A large bus was adapted to accommodate up to three clients (Rheuma-Bus) for informal medical counselling regarding any kind of MSC. The initiative was accompanied by country-wide information through broadcasts and newspapers. Between April and October 2005, this bus was positioned at a number of easily accessible public places throughout Austria.
Clients
Before physicians’ evaluation, all individuals were asked by study personnel to assess their severity of pain using a 100 mm visual analogue scale (VAS), ranging from “no” (0) to “extreme” (100) pain. Age, gender, diagnosis if known, duration and current or previous treatment were recorded. Personally identifying data (eg, name, birth-date and so on) were not acquired, because this campaign focused on awareness and information as well as data accrual, but tried to avoid counselling in a professional sense or interfering with patients’ and/or physicians’ practices.
Informal conversations about the presence of known or suspected disease were held and a brief history was taken. No medical examination or procedure(s) took place, although brief physical assessments (eg of the hands) were occasionally performed. Clients were told about the suspected diagnoses and referred to their general practitioner or to specialists for further care. Suspected diagnoses and the recommendation given were recorded.
Statistics
Categorical variables were analysed using Pearson’s χ2 tests (assuming equal distribution of cases among groups). For parametric comparisons, unpaired t tests or analyses of variance were performed (SPSS V.12.0). If analyses of variance indicated significant intergroup differences, pairwise comparisons by t tests were performed. p Values <0.05 were considered significant. Reported values are mean (SD) unless otherwise indicated.
RESULTS
Client demographics
The bus was open for 62 days at 42 sites: 62 rheumatologists/pain specialists recruited from local pain/rheumatology services performed the counselling. In all, 1–3 physicians were available for 6 h/day.
In all, 2862 clients visited the Rheuma-Bus. Thus, on average, 46 individuals were counselled per day (range: 5–128). Among them, 78.2% were women, with a mean (SD) age of 67.8 (14.7) years. Self-reported mean duration of musculoskeletal pain was 8.5 (9.5) years, mean current pain intensity (VAS) was 59.0 (20.6) mm. Values did not differ statistically between men and women.
History of care
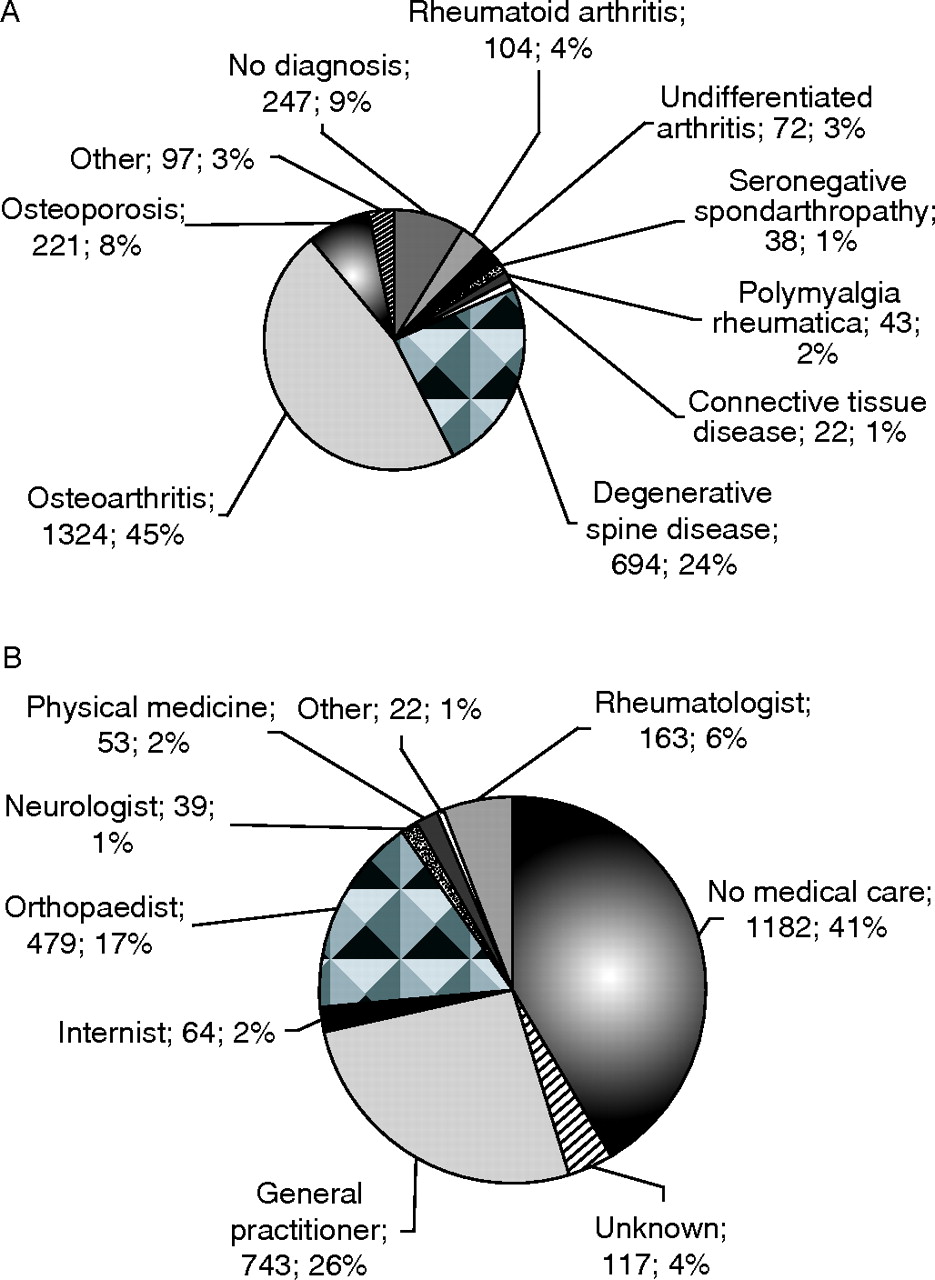
The largest subgroup (n = 1166, 41%) had never before consulted a physician for their painful condition. The second largest group (n = 744, 26%) comprised patients who were treated by general practitioners, followed by orthopaedic care (n = 477, 17%). Only 157 (6%) patients had been seen by rheumatologists (fig 1B⇓).

{kind=link}
(A) Suspected diagnoses. The majority of clients were suspected to have degenerative joint or spine disease. A sizeable proportion (close to 10%) was suspected to have a chronic inflammatory disease. (B) History of medical care among the 2862 clients. The largest subgroup had not been seen by any physician for their painful condition before being counselled in the Rheuma-Bus.
Diagnoses
Figure 1A⇑ shows the distribution of presumed diagnoses. Degenerative joint/spine disease was suspected in 69%. In 8% of all clients, osteoporosis was present by history, and in 11% an inflammatory MSC was suspected. Thus, at least 2518 (88%) of the counselled individuals had pain caused by MSC. In 8.6%, the counselling physicians indicated no diagnosis, the remaining causes of pain (<4%) were considered to be of non-rheumatological origin.
Rheumatoid arthritis (RA) was presumed in 104 individuals (3.6% of all clients). Interestingly, among the 72 who had been given this diagnosis previously, only 36 were cared for by a rheumatologist; 11 patients with RA had not been treated by any physician over the past years. In 32 clients (1.1% of all individuals), RA was considered for the first time by the physician in the bus. These patients were referred to a rheumatology unit.
Pain scores and physician care
Pain scores differed significantly between diagnostic groups: Inflammatory conditions (RA, undifferentiated arthritis, seronegative spondarthropathies etc) were associated with significantly greater pain than degenerative MSC or osteoporosis (table 1⇓).
Pain scores according to disease groups
Individuals not under physicians’ care reported significantly lower pain scores than patients treated by physician(s) (55.3 (20.1) vs 61.7 (20.8); p<0.001), indicating that the degree of pain might be a driving force to seek physicians’ help. Approximately half the clients whose pain scores were in the lowest tertile (<49 mm) were not under physicians’ care. This proportion significantly decreased to ∼30% in the highest tertile (>70 mm; supplementary Figure 1⇑ available online at http://ard.bmj.com/supplemental).
History of pain-treatment
Non-steroidal anti-inflammatory drugs were the most common treatment (40.0%), followed by physical therapy (17.0%), non-opioid analgesics (eg, paracetamol; 9.8%) and opioids (5.0%). Antidepressants were used rarely (<2.5%; supplementary fig 2). Opioids were used more frequently in patients with pain scores above the mean (supplementary table).
Clients with a history of medication had significantly higher pain scores (VAS 60.0 (20.6)) than clients receiving no pharmacotherapy (56.4 (21.1), p = 0.006). In addition, disease duration was positively correlated with VAS pain scores (correlation coefficient: 0.157, p<0.001).
DISCUSSION
Our observations show that many individuals having musculoskeletal pain who accepted this offer of counselling had never visited a physician before for their problem. Importantly, patients under physicians’ care reported significantly higher pain scores compared with those not seeking such care. The threshold above which clients sought medical help seemed to be unacceptably high: the mean pain score in the group of individuals who stated not to have seen a physician for their MSC was ∼55 mm, a level at which guidelines tend to recommend opioid treatment (http://www.nccn.org/professionals/physician_gls/PDF/11 pain.pdf. 2006).9
The proportion of individuals who were not under medical care was significantly lower in the group of clients with high MSC-induced pain scores (>70 mm VAS). Nevertheless, even in the “high-intensity-pain group”, ∼30% of clients were not cared for by any physician. Remarkably, patients treated with drugs reported higher pain scores. Since it is unlikely that treatment contributed to more pain, it seems that individuals have to reach an even higher threshold of pain before being willing to take specific drugs. Alternatively, drug dose might have been insufficient. This indicates that even treated musculoskeletal pain is still a “neglected problem” not accepted as an important condition worth dealing with.
This study aimed at improving awareness of “passers-by”, enhanced by accompanying media announcements. Its conclusions are in line with the data from other studies with different design. Such previous European studies concerning public awareness of rheumatic diseases showed that the consequences of rheumatic diseases and the associated pain are largely undervalued, despite recognition of pain as one of the major manifestations of rheumatic diseases.10,11 One survey revealed that the knowledge of pain management may improve over time through mass-media education12 despite residual misconceptions regarding therapy. Our study shows that patients seek treatment for their MSC, only at a very high threshold of pain. The reason underlying this attitude may be local factors (cultural, regional or societal); however, we observed no significant differences in pain scores between regions (rural vs metropolitan; data not shown).
Another important finding is that almost 3% of the clients seemed to have hitherto unrecognised inflammatory rheumatic diseases, with 1% each presumed to have RA and polymyalgia rheumatica. Again, this observation indicates negligence in assigning sufficiently important rank to musculoskeletal diseases, even inflammatory ones, for accessing specialised care. This is in line with the general notion of the relative neglect of information and funding for this disease group compared with other areas of medicine.8 It is also in line with previous observations on a broadly non-informed state of the public and physicians regarding rheumatic diseases.13
Our study has clear limitations. First, this analysis was cross-sectional and it was impossible to check reliability and accuracy of the data and tentative diagnoses. Second, the nature of this study allows no inference to the distribution or prevalence of rheumatic disease. On the other hand, this campaign offered access to counselling for almost 3000 individuals and led to previously unrecognised insights, which are likely to be valid in other countries also.
In summary, this analysis shows that many individuals with MSC seemingly neglect their disease, not looking for help at all or seeking treatment only above a very high pain-threshold. In addition, patients’ mean pain scores while under treatment suggest that MSC are still undertreated and not considered to importantly contribute to disability and decreased quality of life. Primary healthcare takers seem to underdiagnose inflammatory rheumatic conditions or to refer patients rarely to specialist care. These results, if confirmed in other similar studies, call for major measures by health authorities to alleviate suffering and improve the care of MSC, consequently reducing the societal burden.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
* Members of the Rheuma-Bus group are listed in the accompanying online material.
Competing interests: None declared.
Published Online First 4 January 2007