Article Text

Abstract
Background: Severe neurological involvement in systemic lupus erythematosus (NPSLE) is one of the most dreadful complications of the disease.
Objective: To identify the best drug, dose, and treatment.
Patients and methods: The study was a controlled clinical trial at two tertiary care centres of patients with SLE according to the ACR criteria, with incident (no more than 15 days) onset of severe NP manifestations such as seizures, optic neuritis, peripheral or cranial neuropathy, coma, brainstem disease, or transverse myelitis. Induction treatment with 3 g of IV methylprednisolone (MP) followed by either IV monthly cyclophosphamide (Cy) versus IV MP bimonthly every 4 months for 1 year and then IV Cy or IV MP every 3 months for another year. The primary end point was response to treatment: at least 20% improvement from basal conditions on clinical, laboratory, or specific neurological testing variables.
Results: Overall, a response rate of 75% was observed. Of the 32 patients studied, 18/19 receiving Cy and 7/13 receiving MP responded to treatment (p<0.03).
Conclusions: Cy seems to be more effective than MP in the treatment of acute, severe NPSLE.
- CNS, central nervous system
- CSF, cerebrospinal fluid
- Cy, cyclophosphamide
- IV, intravenous
- MP, methyl prednisolone
- MRI, magnetic resonance imaging
- NPSLE, neuropsychiatric systemic lupus erythematosus
- SLE, systemic lupus erythematosus
- SLEDAI, SLE Disease Activity Index
- SLICC, Systemic Lupus International Collaborating Clinics
- neurological involvement
- systemic lupus erythematosus
- treatment
- controlled clinical trials
- methylprednisolone
- cyclophosphamide
Statistics from Altmetric.com
- CNS, central nervous system
- CSF, cerebrospinal fluid
- Cy, cyclophosphamide
- IV, intravenous
- MP, methyl prednisolone
- MRI, magnetic resonance imaging
- NPSLE, neuropsychiatric systemic lupus erythematosus
- SLE, systemic lupus erythematosus
- SLEDAI, SLE Disease Activity Index
- SLICC, Systemic Lupus International Collaborating Clinics
- neurological involvement
- systemic lupus erythematosus
- treatment
- controlled clinical trials
- methylprednisolone
- cyclophosphamide
The involvement of the central nervous system (CNS) is one of the major causes of morbidity and mortality in patients with systemic lupus erythematosus (SLE), and it is the least understood aspect of the disease.1 Its treatment continues to represent a major therapeutic challenge for the clinician in daily practice. The ideal drugs, doses, and length of treatment are not yet well defined.2
During the past two decades treatment has focused on the severity of CNS manifestations, and so far, has included symptomatic treatment such as antidepressants, anticonvulsants, antipsychotic drugs, and low dose corticosteroids. Immunosuppressive therapy has been employed in severe manifestations, and therapeutic regimens include high dose corticosteroids, intravenous (IV) pulse methylprednisolone, pulse cyclophosphamide, IV immunoglobulins, intrathecal methotrexate, azathioprine, mycophenolate mofetil, plasmapheresis, and biological agents (rituximab), with varying degrees of success in case series.3,4,5,6,7,8,9,10,11
To further complicate the situation antiphospholipid antibody syndrome may have an important role in CNS manifestations in patients with SLE.12–,14 In these cases treatment has included low dose aspirin, long term warfarin and, on some particular occasions (transverse myelitis) IV corticosteroids and immunosuppressant drugs have been employed.8,11 In none of these cases is a clinical trial available.
Clinical trials of therapeutic agents in SLE are difficult to carry out for several reasons. There are usually relatively small numbers of patients eligible for trials, the disease is highly heterogeneous, patients’ follow up is usually short, and there are no reliable biosurrogates of disease activity and organ damage.15
This study aimed at comparing two different monthly IV regimens: methylprednisolone (MP) versus cyclophosphamide (Cy) in the long term treatment of severe neurological involvement in SLE (NPSLE).
PATIENTS AND METHODS
Between July 1998 and July 1999 a total of 32 patients with SLE were enrolled in the trial at two tertiary care centres in Mexico City. All patients met the following study criteria: a diagnosis of SLE according to the American College of Rheumatology Criteria16; age ⩾18 years; and one of the following active NPSLE manifestations: peripheral/cranial neuropathy, optic neuritis, transverse myelitis, brainstem disease, or coma. All patients had no more than 15 days of onset (incident NPSLE). We also included patients with refractory seizures.
Exclusion criteria were CNS or systemic infections, known hypersensitivity to study drugs, or metabolic encephalopathy. Patients who had received pulse MP or Cy at any time during the 3 months before the start of the study were also excluded.
Any patients with neurological manifestations directly related to antiphospholipid syndrome17 were excluded as were patients with pure psychiatric involvement or mild CNS manifestations.
If any patient developed life threatening infections or haemorrhagic cystitis during the follow up period, the disease had to be eliminated and the patient included in an intention to treat analysis.
The ethics committees of both hospitals approved the study. Written informed consent was obtained from all study patients.
Assessment of NP manifestations
Peripheral neuropathy was defined as sensory or motor dysfunction compatible with mononeuritis multiplex or polyneuropathy, confirmed by electromyography. Follow up was by electromyography and visual analogue scales for strength and sensitivity as well as by muscular strength assessment using the British Empire Council scale.17a
Optic neuritis was defined as acute loss of vision, corroborated by neuro-ophthalmological examination and visual evoked potentials. Computed tomography and fluoroangiography were performed in order to exclude thrombotic events. Follow up included a full neuro-ophthalmological examination.
Transverse myelitis was defined as acute quadriplegia or paraplegia, with changes in osteotendinous reflexes, anaesthetic level, and loss of sphincter control.5 Follow up was by electromyography and included visual analogue scales for strength and sensitivity as well as muscular strength assessment using the British Empire Council scale.17a
Coma was defined as loss of consciousness with no response to verbal stimuli, excluding brain tumours or vascular malformations, active CNS infections, or metabolic encephalopathy. Follow up was assessed by noting changes in Glasgow scale ratings.
Refractory seizures were defined as persistence of seizure activity, with at least three episodes/month despite treatment with prednisone 30 mg/day and azathioprine 2 mg/kg/day for a minimum of 3 months. Follow up was by electroencephalogram evaluation.
Magnetic resonance imaging and lumbar puncture were performed in patients with CNS involvement. Evoked potentials were done in some specific cases.
Randomisation procedure
Patients were prestratified by centre and by NP manifestation and then randomised in blocks of 10 patients by a random number computer generated program. These lists, together with operative manuals, were distributed to both centres.
Treatment protocol
After randomisation each patient was allocated to receive MP 1 g daily for 3 days as induction treatment. This was followed by one of the following two treatments: MP 1 g daily for 3 days, monthly for 4 months, then bimonthly for 6 months and subsequently every 3 months for 1 year or Cy 0.75 g/m2 body surface monthly for 1 year and then every 3 months for another year. Oral prednisone was started on the fourth day of treatment, at 1 mg/kg/day, for no more than 3 months and tapered according to disease activity/remission.
Symptomatic treatment (anticonvulsants, analgesics) had to remain at the dose at entry to the study, and they were allowed to be tapered according to clinical activity, but no increases were allowed.
Primary end point
Response to treatment was rated according to Neuwelt et al18 as (a) improvement: 20% change from basal conditions in clinical, serological, and specific neurological measures (evoked potentials, cerebrospinal fluid analysis (CSF), electromyography, magnetic resonance imaging (MRI), etc) achieved by the fourth month of treatment; (b) worsening: disease progression of 20% or more despite continued treatment for at least 4 months.
Failure to improve after 4 months was considered grounds for stopping treatment early. In which case these patients were only considered in the intention to treat analysis and were subsequently treated according to the recommendations of their attending physician. In addition, a measurable response had to be sustained during the follow up period.
A preliminary cut off point was planned at the first 4 months after the first patients were recruited, and if any major adverse event or unfavourable outcome occurred in any of the groups, early stopping rules were applied.19
Patients were seen every month by the same rheumatologists (LB or JF) and the following laboratory data were recorded, once at baseline and once at each subsequent monthly consultation: complete blood cell count, urine analysis, and urine and throat cultures. C3 and C4 (nephelometry) were performed at baseline, at month 12, and at the final visit.
Additionally, CSF analysis (protein content, glucose, and differential cell count) and MRI were performed upon entry into the study, and for a particular NP manifestation one or more of the following tests were done: electroencephalography, visual evoked potentials, electromyography, Glasgow scale ratings, visual analogue scale for muscular strength and sensibility ratings, and a neuro-opthalmological examination.
Global activity was evaluated by the SLE Disease Activity Index (SLEDAI)27 at entry and every 3 months.
Statistical analysis
We used non-parametric tests. Median, minimum, and maximum values were employed for descriptive analyses; Wilcoxon’s ranked test and Mann Whitney’s U test for correlation analyses; and Friedman’s analysis for multiple qualitative measurements. Response to treatment was evaluated with χ2 and Fisher’s exact tests.
If any NP manifestation appeared to be overrepresented, we used a Maentel-Haezel test for different strata.
All data were entered on an SPSS 10.0 program PC compatible (SPSS Inc, Chicago, IL). A p value <0.05 was considered significant. Data were analysed at months 3, 6, 12, and 24.
RESULTS
We included 32 patients (30 women, two men) out of 38 eligible patients with incident NP symptoms. Six were excluded because of thrombotic NP events. Of the 32 mainly young patients with a short disease duration, 19 received Cy and 13 MP. The demographic characteristics were similar in both groups (table 1⇓). In two of the patients the NP syndromes were the first disease manifestation. Table 2⇓ shows the extraneurological features of SLE.
Demographic characteristics and basal immunological tests at baseline
Other disease features
Disease activity
The median SLEDAI was 10 and 14 for Cy and MP, respectively, and the mean prednisone dose was at least 40 mg/day. Table 3⇓ shows the distribution of the different NP syndromes according to treatment. The most common NP manifestation in the overall group was seizures, with a total of 11 patients, followed by peripheral neuropathy and optic neuritis; the remaining NP syndromes were seen in four patients or fewer each.
Patients distribution by neurological syndromes
Overall, a response rate of 75% was observed, with 24/32 patients responding to treatment, and with treatment failure in only eight (25%) patients. Figure 1⇓ shows the response according to each treatment group. Most of the treatment failures were seen in the MP group, with only one failure recorded in the Cy group (p<0.001, Fisher’s exact test). Average recovery or full response was seen at the fifth month of treatment in both groups.
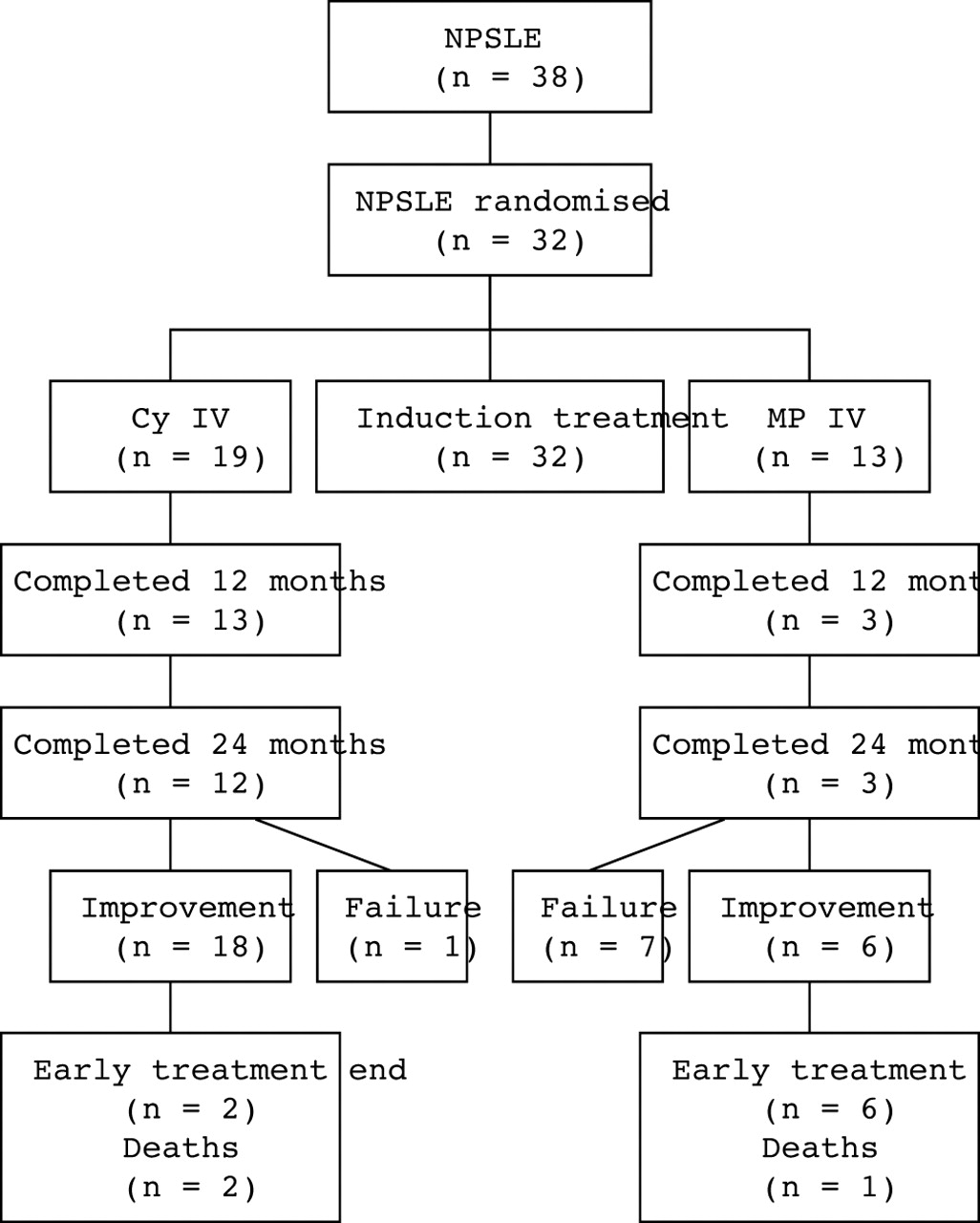
Patient’s outcome throughout follow up.
Seizures were the most common NP manifestation in our final dataset. To determine whether statistical significance was related only to seizures or to all the NP manifestations included we considered four strata: (a) only seizures; (b) peripheral neuropathy; (c) transverse myelitis and optic neuritis added; and (d) the remaining cases, seen in two patients or fewer, included. The overall significance persisted, with a p value of 0.002. We found no differences in any particular strata.
Response variables in the different clinical subgroups
Seizures
Figures 2A and B⇓ show the median number of seizures by group. All the patients had generalised seizures, 10 with tonic-clonic manifestations (grand mal) and one with absence-type involvement (petit mal). We observed a significant decrease in the number of seizures per month in the Cy group. All the patients in the Cy group had electroencephalographic improvement, shown either by a disappearance of epileptogen foci, or by a better overall wave rhythm pattern. In contrast, only two of five in the MP group improved (figs 2A and B⇓).

Mean number of seizures/month in (A) MP group; (B) Cy group.
Optic neuritis
Of the five patients with optic neuritis, visual function improved by at least 25% and up to 75% in the four patients included in the Cy group. All the patients had an initial visual acuity of finger counting of <1 m, and two of them achieved 20/40 vision after 1 year of treatment, while the other two continued to have a visual acuity of 20/70 and 20/80, respectively. No improvements were seen in the MP group.
Transverse myelitis
Two patients with transverse myelitis were in the MP group. The first became pregnant by the fourth month of treatment, despite the use of birth control, and therefore she was suspended early from treatment; by the time of her withdrawal she was beginning to improve. The second patient had finished 2 years of treatment when she was switched to receive MP every 3 months. Her neurological symptoms relapsed, and therefore she had to receive monthly pulses for 2 months and then bimonthly pulses for another 4 months. Anal sphincter control was recovered at the 6th month of treatment, bladder sphincter control was only partially recovered, and she continued to have a neurogenic bladder.
The other three patients were receiving Cy. Two of them died, one of them due to severe disease activity (Evans’s syndrome) and the other initially improved. However, she abandoned treatment after five pulses, after which she developed abdominal vasculitis and died. The third patient completed 24 months of treatment and she can currently walk, with only partial bladder sphincter control.
Peripheral neuropathy
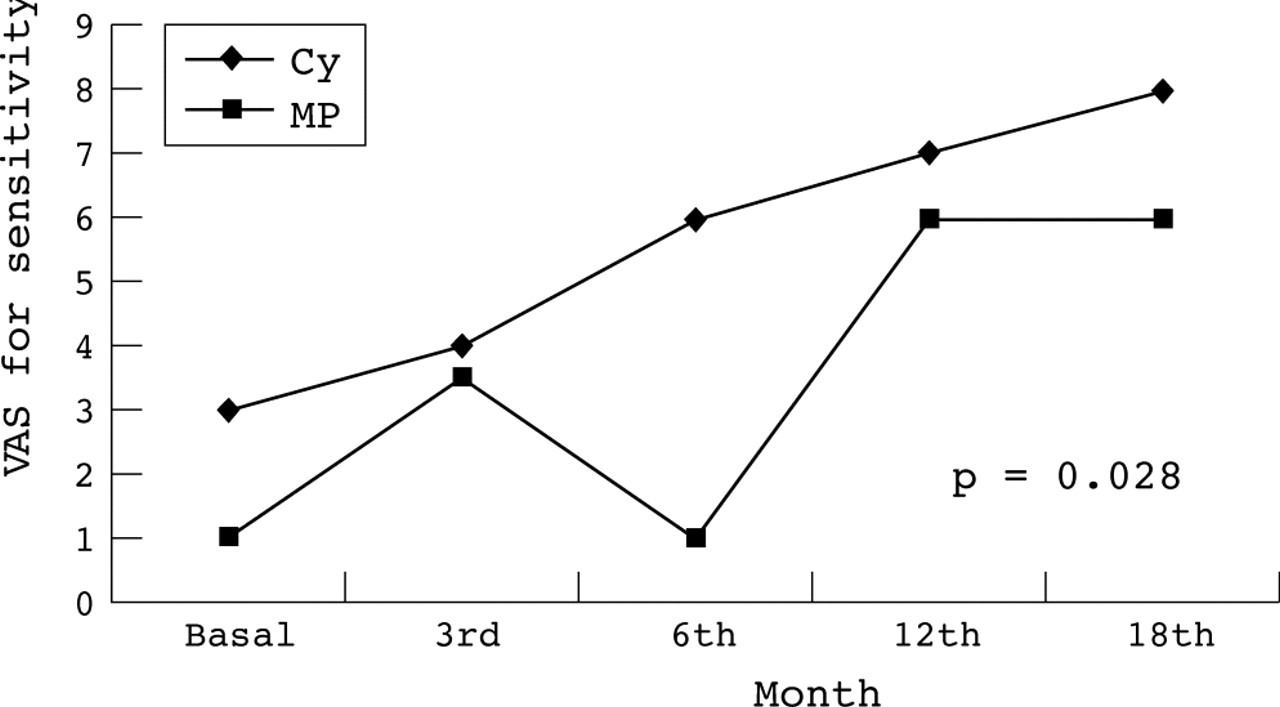
Four patients with peripheral neuropathy were assigned to Cy; for three of them electromyographic findings, and sensitivity and muscular strength scales (figs 3⇓ and 4⇓) improved and for one of them treatment failed.

Changes in visual analogue scale for sensitivity in transverse myelitis and peripheral neuropathy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in visual analogue scale for muscular strength in transverse myelitis and peripheral neuropathy.
Three patients received MP. In one of them signs of treatment failure were seen at the 6th month of follow up, in another treatment was suspended early because she withdrew consent, and the last patient experienced an adverse event (pancreatitis) that caused treatment withdrawal at the 5th month of follow up.
Brainstem disease
One patient in each group had brainstem disease. Treatment failed for the patient receiving MP, with structural abnormalities in evoked potentials, and the patient receiving Cy improved. Evoked potentials were consistent with structural brainstem damage and were described as normal after treatment, at the 12 month evaluation.
Coma
One patient in each group had a coma. Both improved within the first 15 days of treatment.
Nuclear ophthalmoplegia
One patient in the Cy group had nuclear ophthalmoplegia. She improved, but treatment was temporarily withdrawn because of concurrent infection, after which she presented with meningeal signs, seizures, and died.
Seven (22%) patients had an abnormal magnetic resonance finding. The most common findings were hyperintense plaques with signal enhancement in T2 weighted images in three patients (one with coma, one with brainstem disease, and the other with seizures) and cortical atrophy in four patients. Three out of seven showed a normal MRI scan after the 1st year of treatment. The three were receiving Cy—one with brainstem disease, one with coma, one with seizures.
When we analysed individual variables, no major differences in lymphocytes, haemoglobin, leucocyte, or neutrophil counts were found. We did find a statistically significant difference in oral prednisone requirements by the third month of treatment, as well as median SLEDAI rating, both favouring the Cy group (Table 4⇓).
Changes in study variables during follow up
Interestingly, glucose and protein levels in the CSF were basically normal in all the patients with CNS involvement (glucose 3.6 (1.6) mmol/l, proteins 0.28 (0.15) g/l).
No significant differences in adverse effects between the groups were found (table 5⇓). The most common side effects were infections of the gastrointestinal tract and upper respiratory system. Two major adverse events occurred in the MP group (pancreatitis and uncontrolled hypertension), which led to protocol withdrawal. None of the patients in the Cy group had to finish treatment early owing to a major adverse event.
Adverse events in both treatments during follow up
Cy exerts a beneficial effect on specific disease activity measurements such as the SLEDAI, and also a steroid sparing effect, both were statistically significant when compared with MP (table 4⇑). For disease related damage, Systemic Lupus International Collaborating Clinics (SLICC) measurements were 0.88 for Cy and 0.82 for MP at the study inclusion and they improved to 0.72 and 0.80, respectively, at the end of follow up; although there is a trend towards Cy, this was not significant.
Fifteen patients were able to complete the protocol up to 2 years of treatment: 12 receiving Cy and only three in the MP group. Every patient receiving MP had to be given monthly pulses at least once during the 2nd year owing to a disease flare—one of them because of transverse myelitis symptoms and the other two because of extraneurological activity.
DISCUSSION
In this study we conducted a long term controlled clinical trial, with incident cases and a balanced sample in two referral centres. Our findings showed that Cy was significantly more effective than MP. Cy was clearly better in patients with seizures, peripheral neuropathy, optic neuritis, and brainstem disease, while differences were not clear in coma and transverse myelitis.
Treatment failed for 1/19 in the Cy group compared with 7/13 in the MP group, and this difference was significant. In addition, for the MP group when treatment was changed to every 3 months, relapses were frequent both as neurological and extraneurological manifestations. Side effects were similar in both groups.
Until recently, NP lupus treatment has been widely heterogeneous owing to the wide range of NP manifestations,1,19,28 their relapsing course, and the difficulty in gathering a representative sample for a controlled study. Therefore, our study represents one of the scarce controlled clinical trials in SLE.
Most studies that have examined the clinical response to immunosuppressive treatment in NPSLE have been short term reports of one or several patients (in general no more than 10) and most have failed to evaluate long term outcome and the need for sustained treatment (table 6⇓).
Previous published series
Recently, the Cochrane study group performed a meta-analysis of the efficacy of MP versus Cy in NPSLE and they did not find one comparative study that could be included.29
Our study suggests that in order to achieve optimal response with no flares, treatment with Cy should be sustained for 2 years.
Our group has previously reported the long term outcome of a cohort of more than 50 NP patients followed up for 10 years30; there was a tendency for relapse whenever immunosuppressive therapy was withdrawn before at least 12 months of treatment. This seems biologically plausible because other major organs such as the kidney require at least 2 years of treatment in order to improve long term survival or to prevent progression to renal failure.31 It seems logical that the brain should also require such treatment.
The differences in clinical responses in the different NP subsets might be explained by differences in the pathogenic mechanisms. It has been suggested that several pathogenic mechanisms have a role in a variety of clinical symptoms. A true vasculitic process affecting the cerebral circulation is less common than alterations of the cerebral microcirculation, even though in both situations, brain endothelium does represent the target of pathogenic mechanism.32
The study has some limitations. Although we originally planned to study a larger sample, we only studied 32 patients, because during follow up of the first enrolled patients it became clear that rate of treatment failures after the pre-established evaluation point (4 months) in the MP treatment group was unacceptable. Therefore it seemed unethical to enrol further patients into this treatment, and we stopped the recruitment early according to the protocol rules.33
In conclusion, in this initial study Cy seems to be more effective than MP in the treatment of severe NPSLE. Larger studies are necessary to document the beneficial effect of CY in NPSLE.
Acknowledgments
The study was reported in its abstract version at the American College of Rheumatology Meeting, San Franciso, 2000, and at the 6th International Lupus Conference, Barcelona, 2001.
This project was partially supported by grant No 297M1 from Consejo Nacional de Ciencia y Técnología (México).