Article Text

Abstract
Objective: To evaluate the gastrointestinal safety and efficacy of the COX inhibiting nitric oxide donator AZD3582 in patients with hip or knee osteoarthritis.
Methods: 970 patients were randomised (7:7:2) to AZD3582 750 mg twice daily, naproxen 500 mg twice daily, or placebo twice daily in a double blind study. The primary end point was the six week incidence of endoscopic gastroduodenal ulcers (diameter ⩾3 mm). Overall damage measured on the Lanza scale was a secondary end point. Safety and tolerability assessments included endoscopic upper gastrointestinal erosions and the gastrointestinal symptom rating scale (GSRS). Efficacy was primarily assessed by WOMAC.
Results: The incidence of ulcers with AZD3582 was 9.7% and with naproxen 13.7% (p = 0.07, NS), v 0% on placebo. The incidence of Lanza scores >2 was higher with naproxen (43.7%) than with AZD3582 (32.2%) (p<0.001). Compared with baseline, significantly fewer ulcers and erosions developed in stomach and stomach/duodenum combined, and fewer erosions developed in stomach, duodenum, and both combined on AZD3582 than on naproxen. GSRS reflux and abdominal pain subscale scores were lower for AZD3582 than for naproxen but there was no difference for indigestion, constipation, and diarrhoea. AZD3582 was as effective as naproxen at improving WOMAC scores. Both agents were well tolerated, with no significant effects on blood pressure.
Conclusions: At doses with similar efficacy in relieving osteoarthritis symptoms, the primary end point of six week endoscopic gastroduodenal ulcer incidence was not significantly different between AZD3582 and naproxen. Most secondary endoscopic gastrointestinal end points favoured AZD3582.
- ACR, American College of Rheumatology
- COX, cyclo-oxygenase
- CINOD, COX-inhibiting nitric oxide donator
- GSRS, gastrointestinal symptom rating scale
- ITT, intention to treat
- NSAID, non-steroidal anti-inflammatory drug
- SF-36, 36 item short form health survey
- VAS, visual analogue scale
- WOMAC, Western Ontario and McMasters University osteoarthritis index
- CINOD
- AZD3582
- naproxen
- gastrointestinal safety
- osteoarthritis
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- COX, cyclo-oxygenase
- CINOD, COX-inhibiting nitric oxide donator
- GSRS, gastrointestinal symptom rating scale
- ITT, intention to treat
- NSAID, non-steroidal anti-inflammatory drug
- SF-36, 36 item short form health survey
- VAS, visual analogue scale
- WOMAC, Western Ontario and McMasters University osteoarthritis index
Non-steroidal anti-inflammatory drugs (NSAIDs) are effective in the treatment of acute and chronic pain in patients with osteoarthritis.1,2 Their anti-inflammatory and analgesic effects arise from the blockade of prostaglandin synthesis through inhibition of cyclo-oxygenase (COX) enzymes. However, this action results in well documented gastrotoxicity.3–6 In clinical endoscopy studies lasting from one to six months, the incidence of ulcers that are at least 3 mm in diameter in patients receiving non-selective NSAIDs (for example, naproxen, diclofenac, ibuprofen, piroxicam) ranges from 10% to 50%.7,8,9,10,11,12,13 Complications, such as perforation and bleeding, attributable to NSAID use occur in up to 1% of long term NSAID users,3,14 with 15–35%15 of the 15 000 deaths a year in the USA and the 4000 deaths a year in England and Wales that involve peptic ulceration attributable to NSAID use.4,16,17
The COX inhibiting nitric oxide donator (CINOD) class was developed for the treatment of acute and chronic pain. CINODs are designed to provide a multipathway mechanism of action of COX inhibition and controlled nitric oxide donation. In the gastrointestinal tract, nitric oxide mediates many processes that contribute to gastric mucosal integrity and, in particular, it exerts many of the same physiologically protective actions as prostaglandins.18 Thus it is hypothesised that donation of nitric oxide within the gastrointestinal tract may protect the mucosa from many of the adverse consequences of COX inhibition.18,19 Representatives of this class are effective analgesic and anti-inflammatory agents with improved gastrointestinal safety profiles over non-selective NSAIDs in animal models.20
AZD3582 (4-(nitro-oxy)butyl-(2S)-2-(6-methoxy-2-naphthyl)propanoate) was the first CINOD to be studied in large clinical trials. It donates nitric oxide both in vitro21 and in vivo (Adding LC et al, personal communication) and inhibits both COX-1 and COX-2.22 AZD3582 effectively and dose dependently reduced pain and inflammation in rat models,23 and was associated with less gastrointestinal injury than equimolar doses of naproxen in rat models of gastrointestinal safety.24–26 In a 12 day study of 31 healthy volunteers,27 there were significantly fewer gastroduodenal erosions on AZD3582 than on naproxen. Moreover, naproxen increased intestinal permeability, a marker of small intestinal damage, whereas AZD3582 and placebo did not.27 On the basis of these data, we evaluated the gastrointestinal safety, tolerability, and efficacy of AZD3582 in patients with osteoarthritis over a six week period. This is the first reported, randomised, controlled trial of a CINOD in patients with musculoskeletal disease.
METHODS
Patients
Men and women aged 40 to 75 years with symptomatic osteoarthritis of the knee or hip of at least three months’ duration were recruited. All patients had radiographic evidence of hip or knee osteoarthritis (qualified as American College of Rheumatology (ACR) global functional class I, II, or III) and were current NSAID or paracetamol (acetaminophen) users. Helicobacter pylori status was assessed by serology at screening.
Patients were excluded from the study if they had any of the following: osteoarthritis secondary to inflammatory joint disease; a diagnosis of arthritis other than osteoarthritis; a history of gastric or duodenal bleeding within six months, or gastric or duodenal ulcer within three months; NSAID hypersensitivity; history of orthostatic hypotension; endoscopic ulcers at baseline screening. Patients on aspirin, H2 antagonists, antacids, misoprostol, proton pump inhibitors, or sucralfate were not eligible, and the use of these agents was prohibited throughout the study period.
Study design
The protocol was a six week, double blind, randomised, parallel group, placebo controlled study conducted at 80 sites: 15 in the United Kingdom, 12 in South Africa, eight in Poland, 13 in Hungary, 14 in Norway, six in Brazil, six in Argentina, and six in Mexico. The study was conducted from November 2001 to November 2002. It was carried out in accordance with the ethical principles in the Declaration of Helsinki, good clinical practice, and applicable regulatory requirements. The institutional review board or independent ethics committee of each participating centre provided ethical approval of the study protocol. All patients gave their written informed consent.
Subjects were randomised in a 7:7:2 ratio to AZD3582 750 mg twice daily, naproxen 500 mg twice daily (which is an equimolar naproxen dose), or placebo twice daily. Study blinding was maintained by using capsules of AZD3582, naproxen, and placebo of identical appearance. Patients were instructed to take the treatment with food at 12 hour intervals. They were considered compliant to the treatment regimen if they took at least 70% of the study drug over the course of the study. Compliance was assessed by pill count.
Patients were assessed at an initial screening visit, and those who fulfilled the entry criteria discontinued NSAID treatment for two to 10 days before the baseline visit. Patients were allowed to take paracetamol up to 4000 mg a day, provided by the investigator, for control of pain during the washout period. If the patient used paracetamol, it was requested that it be discontinued 12 hours before the baseline visit.
Safety, tolerability, and efficacy assessments were made at the screening and baseline visits, at weeks 1, 2, 3, 4, 5, and 6, and at the follow up visit (that is, within one week plus or minus three days of the end of the treatment).
Gastrointestinal safety and tolerability assessments
Upper gastrointestinal endoscopy of the oesophagus, stomach, and duodenum was carried out according to local routines. Baseline endoscopy was conducted before the administration of the first dose of study drug. The second endoscopy was to be carried out within two days of the final dose. The primary end point of the study was the incidence of gastric or duodenal ulcers after six weeks of treatment. An ulcer was defined as a break in the mucosa of at least 3 mm in diameter with unequivocal depth, and was measured by close apposition of an endoscopic forceps with defined dimensions. In addition to number of ulcers, the size of the largest ulcer was recorded at each endoscopy.
To explore the properties of the ulcer size cut off employed, we undertook an ad hoc analysis using a minimum diameter of 5 mm as the criterion for an ulcer, instead of the 3 mm diameter that was specified as the primary variable.
Gastric damage was also scored using the Lanza scale.28 The proportion of patients with more than two erosions or an ulcer (Lanza score >2) was a secondary end point. Other secondary end points for gastrointestinal safety were the within-subject change between baseline and end of treatment in the number of oesophageal, gastric, and duodenal ulcers, erosions, and petechiae.
Gastrointestinal tolerability was assessed using the gastrointestinal symptom rating scale (GSRS).29 The GSRS contains 15 questions covering five major gastrointestinal symptoms: abdominal pain, reflux, indigestion, diarrhoea, and constipation. Patients were asked to rate discomfort from each gastrointestinal symptom on a seven point Likert scale, where 1 represents “no discomfort” and 7 represents “very severe discomfort.” The GSRS was applied at the screening and baseline visits as well as on visits at weeks 1, 2, 4, and 6.
Efficacy assessments
The Western Ontario and McMaster Universities (WOMAC) osteoarthritis index, version 3.1 visual analogue scale (VAS),30 and the 36 item short form health survey (SF-36)31 were used to assess response to treatment at baseline, at weeks 1, 2, 4, and 6, and at the follow up visit. Patients answered the WOMAC subscales of pain, stiffness, and physical function using a 48 hour recall period. The acute version of SF-36, with a recall period of one week, was used to evaluate the physical and mental wellbeing of the patients.
Efficacy was also assessed at the six week visit by the subjects’ and physicians’ overall rating of treatment, which were five point Likert scales (where 1 represents “very poor” and 5 represents “very good”) by answering the following questions:
-
Patient: “How do you rate your treatment overall, taking both pain relief and everything else into consideration?”
-
Investigator: “How do you rate the subject’s treatment overall, taking both pain relief and everything else into consideration”
General safety
Patients were questioned by the investigator at each visit about the occurrence of any adverse event. For all adverse events, the investigator recorded the intensity, the seriousness, the action taken, and the outcome. Other assessments included haematology, clinical chemistry, urine analysis, pulse, blood pressure, and electrocardiogram. The blood pressure was measured with a calibrated manometer supine after 15 minutes of rest, and after two and five minutes of standing. At the request of an Independent Safety Monitoring Board (ISMB), the initial 401 patients enrolled in the study had additional assessments of pulse and blood pressure at one, two, and three hours after the first dose, and two to three hours after dosing following three days and one week of treatment.
Statistical analysis
The primary objective was to compare the proportion of patients with gastroduodenal ulcers after six weeks’ treatment with AZD3582 or naproxen, using a two sided 95% confidence interval (CI) for the AZD3582/naproxen ratios of proportions. The confidence interval was based on a generalised linear model with log as link function and a binomial distribution taking country into account. Studying 350 patients in each of the two groups made it possible to show a 50% reduction with a power of at least 80% with AZD3582, assuming 4–6% of patients would get ulcers on AZD3582 and 20–25% on naproxen.
The within-subject differences between baseline and the mean of treatment weeks 4 and 6 were used to analyse changes in WOMAC subscale scores and GSRS subscales. For the SF-36, the within-subject differences between baseline and the end of treatment for each subscale were analysed. An analysis of covariance (ANCOVA) approach with adjustment for country, baseline, and treatment was used for the pairwise comparisons between the different treatment groups when analysing WOMAC, GSRS, and SF-36. No correction for multiple comparisons was to be made.
Efficacy and safety analyses were carried out on all randomised patients who received at least one dose of the study preparation. The analysis of the primary end point involved an initial pairwise comparison of the ratio of the incidence of gastroduodenal ulcers with naproxen and placebo. The statistical analysis only allowed a comparison of AZD3582 and naproxen if a significant difference had been detected between naproxen and placebo.
A supplementary per-protocol analysis was carried out. This included all patients taking at least 70% of the investigational product, having the second endoscopy within two days before or after the last intake of the study drug, and without any other major protocol deviations judged to have an impact on the endoscopy result.
RESULTS
Patients
In all, 1297 patients were enrolled in the study, of whom 970 were randomised and received at least one dose of investigational product; 838 completed the six week long trial (fig 1). There were 898 patients (100 in the placebo group, 404 in the AZD3582 group, and 394 in the naproxen group) who had two endoscopies within or outside the protocol-specified two days before or after the last intake of study drug, and were included in the analysis of the endoscopy based variables (ITT). In the supplementary per-protocol analysis, 686 subjects were included (77 in the placebo group, 314 in the AZD3582 group, and 295 in the naproxen group). Of the 212 subjects excluded, 184 exclusions were because the second endoscopy was outside the specified two days. These exclusions were well balanced across the three groups. The remaining subjects were excluded because they received a prohibited drug (1.6% of the AZD3582 group, 0.7% of the naproxen group, 3.4% of the placebo group), took less than 70% of investigational product (3.4% AZD3582, 3.4% naproxen, 5.2% placebo), or had other important deviations from the protocol (2.1% AZD3582, 2.4% naproxen, 1.7% placebo).

Patient disposition in a six week placebo controlled trial of the gastrointestinal safety and efficacy of AZD3582 and naproxen in patients with osteoarthritis.
The treatment groups were well balanced at baseline for demographic characteristics, joints affected by osteoarthritis, Hpylori status, and ACR functional class (table 1). There were no differences in baseline endoscopy scores between treatment groups. Further, there were no differences in baseline WOMAC scores between treatment groups or between those with hip or knee osteoarthritis. The baseline scores for all SF-36 domains were similar between treatment groups, as were the proportions of subjects taking rescue medication for osteoarthritis related pain (data not shown). Three subjects with ulcer at baseline were erroneously included in the trial (table 1).
Demographic and baseline characteristics
Gastroduodenal ulcer
None of the patients on placebo had gastroduodenal ulcers by six weeks of treatment, compared with 13.7% in the naproxen group and 9.7% in the AZD3582 group. Compared with placebo, the incidence of gastroduodenal ulcers was higher with both AZD3582 (p<0.002) and naproxen (p<0.0001). The ratio in ulcer incidence between AZD3582 and naproxen was 0.70 (95% CI, 0.48 to 1.03) and did not achieve statistical significance (p = 0.07). The results of the per-protocol analysis were similar (10.2% ulcers with AZD3582 v 12.5% with naproxen, p = 0.32). The relative effects of the two treatments were similar in patients who were Hpylori negative or positive at baseline (data not shown) and for ulcers ⩾5 mm in size (7.2% on AZD3582, 9.9% on naproxen, p = 0.18, fig 2).

Incidence and location of ulcers ⩾3 mm or ⩾5 mm (with depth) in osteoarthritic patients treated with AZD3582 or naproxen.
Secondary end points
Table 2 shows the nine prespecified secondary endoscopic end points. AZD3582 was associated with significantly less mucosal injury than naproxen when scored on the Lanza scale, or in terms of the number of erosions and ulcers in the stomach and duodenum combined or stomach alone, and the number of erosions in stomach and duodenum combined, stomach alone, or duodenum alone. There were few duodenal ulcers and little oesophageal injury, so that differences in the number of erosions and ulcers in the duodenum alone and injury scores for the oesophagus were not significantly different between the two active treatments.
Secondary endoscopic end point results (Lanza and erosion scores) at week 6
Symptoms and quality of life
On the GSRS scale, treatment with AZD3582 was associated with an improved within-subject difference between baseline and treatment in weeks 4–6 of 0.14 (95% CI, 0.03 to 0.25) (p = 0.011) for reflux and 0.11 (0.02 to 0.2) (p = 0.016) for abdominal pain, compared with naproxen. There were no significant differences between AZD3582 and naproxen in the GSRS indigestion, constipation, and diarrhoea subscales, neither were there significant differences in changes from baseline in any of the GSRS subscales for the pairwise comparison of placebo with AZD3582 or naproxen. AZD3582 and naproxen provided significant improvements over placebo in six of eight SF-36 domains: bodily pain, physical functioning, role–physical, vitality, mental health, and social functioning.
Efficacy
As shown in tables 3 and 4, AZD3582 and naproxen were of similar efficacy and significantly better than placebo. The WOMAC subscales showed this to be true for both knee and hip combined, and for knee and hip separately, although the efficacy at the knee was somewhat better than for the hip (table 3). The two active treatments offered greater improvements than placebo in the subjects’ and physicians’ overall rating of treatment (p<0.0001 for both comparisons), and there were no significant differences between AZD3582 and naproxen for either overall rating (table 4). Use of rescue medication (paracetamol) was similarly decreased by AZD3582 or naproxen compared with placebo (data not shown).
Mean change in WOMAC subscales from baseline for knee and hip combined, and for knee and hip separately
Rating of response to treatment
Adverse events
Adverse events occurred in 310 patients (71%) in the AZD3582 group, 295 (71%) in the naproxen group, and 77 (66%) in the placebo group. There were similar incidences and types of clinical adverse events in the three treatment groups (table 5). In particular, the incidence of any gastrointestinal NSAID related adverse events—such as nausea, abdominal pain, or dyspepsia—was similar between groups, with incidences of 28% for AZD3582, 32% for naproxen, and 28% for placebo. Most adverse events were mild to moderate in severity. There were seven serious adverse events reported in six subjects. Similar proportions of patients in each treatment group withdrew because of adverse effects (table 5).
Adverse events and NSAID related gastrointestinal adverse events.
Blood pressure
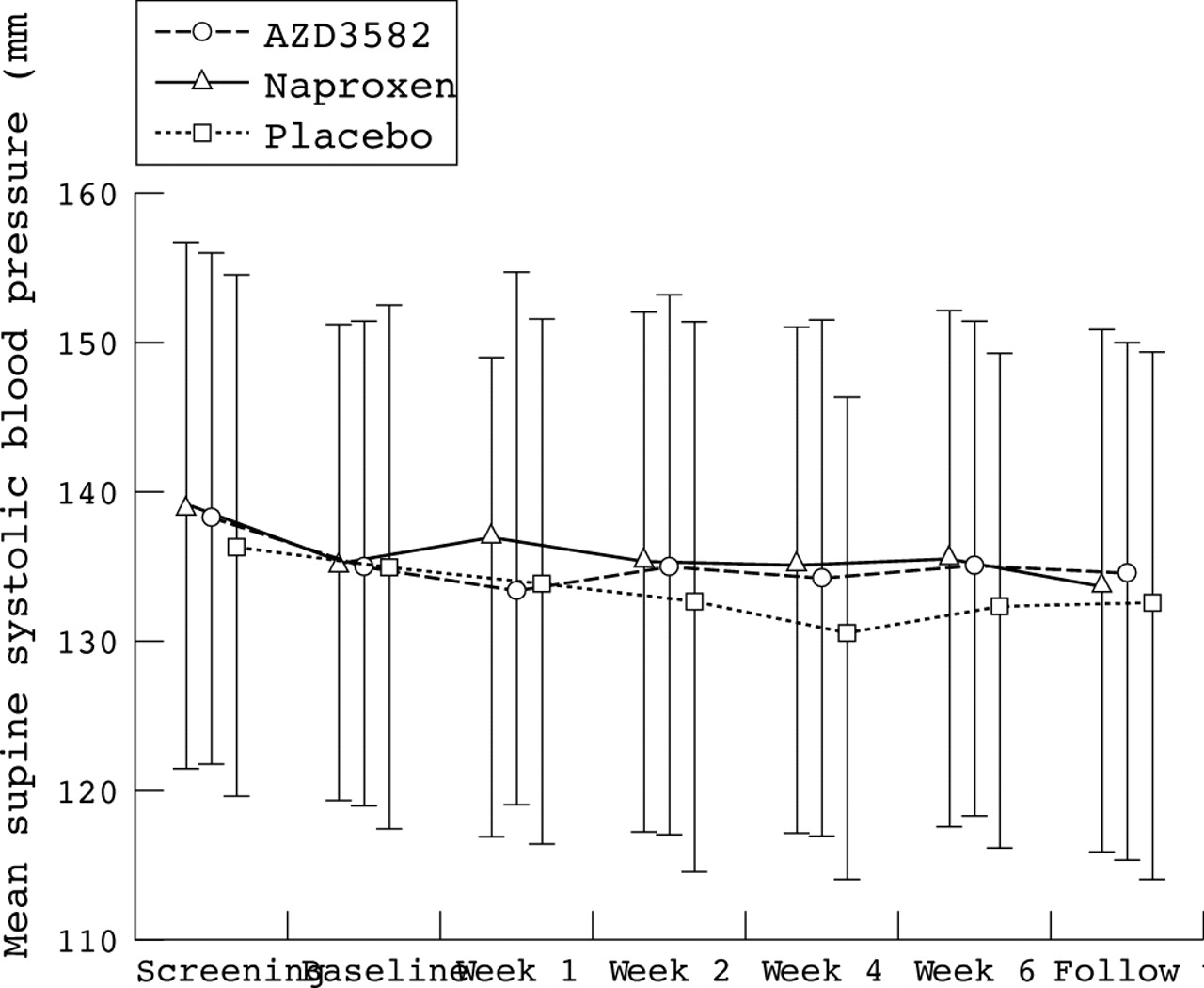
Overall, there were no significant differences between the treatment groups in terms of mean supine systolic (fig 3), diastolic, or mean orthostatic blood pressure (data not shown). The percentage of patients with a systolic blood pressure decrease from baseline of more than 30 mm Hg did not differ between the treatment groups. More subjects on AZD3582 (19%) and naproxen (16%) had a decrease in diastolic blood pressure of greater than 15 mm Hg than in the placebo group (10%), but the proportions with a decrease of 30 mm Hg or more did not differ. These changes were generally well tolerated and did not usually give rise to any symptoms. However, four subjects on AZD3582 had hypotension or decreased blood pressure recorded as an adverse event (versus none on naproxen or placebo), although this did not lead to withdrawal from the study. There were three protocol discontinuations because of a supine systolic blood pressure of 100 mm Hg or less (two in the AZD3582 and one in the naproxen group). In the subset of 401 subjects in whom extra assessments were done at one, two, and three hours after first intake of drugs or placebo, there was a decrease in mean systolic and diastolic blood pressure of 6–8 mm Hg with AZD3582. The effect was less after three to five days, and had diminished further after five to nine days.

{kind=link}
{kind=link}
{kind=link}
Mean supine systolic blood pressure in patients with osteoarthritis receiving AZD3582, naproxen, or placebo. Error bars = SD.
DISCUSSION
AZD3582 donates nitric oxide both in vitro32 and in vivo (Adding LC et al, personal communication). This has been hypothesised to protect the gastrointestinal mucosa from many of the adverse consequences of COX inhibition by preserving adequate blood flow and by increasing protective mucus and bicarbonate secretion.18,19 The protective effect that was shown earlier against erosions in healthy volunteers27 could not be found against ulcers in patients with osteoarthritis in the present study. The incidence of gastroduodenal ulcers for AZD3582 was not significantly less than for naproxen, and both were higher than for placebo.
It is difficult to compare the ulcer incidence of 13.7% for naproxen in the present study with other studies, as the design, duration, and patient population differ across studies. Many studies are 12 weeks long, involve more than two endoscopies, and also involve patients with rheumatoid arthritis. The ulcer incidence from naproxen in studies involving osteoarthritic patients has varied between 10% and 19%,9,33,34 but has been reported to be up to 26% for patients with rheumatoid arthritis.8 The gastroduodenal ulceration rates for COX-2 selective NSAIDs in patients with osteoarthritis were reported to be about 3% after six weeks12,13 and between 3% and 5% after 12 weeks.9
The sample size of 350 patients in each active group was chosen assuming true underlying proportions of 4–6% ulcers for AZD3582 and 20–25% for naproxen. At the end of the trial, 404 patients in the AZD3582 group and 394 in the naproxen group were analysed. With an ulcer incidence of 14% for naproxen it would then still be possible to achieve a significant difference with at least 80% power if the ulcer incidence for AZD3582 were half that of naproxen—that is, around 7%.
Most six week studies have shown ulcer incidences of 3–4% for placebo,8,9,13 so the placebo gastroduodenal ulcer rate of 0% in the present study is low but not unique. Hawkey et al,12 in a 24 week long study where the six week data were presented separately,35 showed no ulcers in 182 patients on placebo. One reason for the low figure in the present study could be that patients with a history of recent upper gastrointestinal events were excluded. This was done for ethical reasons, as these patients are at high risk of developing new and potentially life threatening ulcer complications, but it should also add to the validity and clinical relevance of the study. Further, patients with one or more ulcers at the start of the study were excluded to allow a more easy evaluation of the influence of the study preparation on endoscopic findings. It was also considered more ethical, as those with significant lesions at inclusion would have had a higher risk of developing complications.
In previous studies, it has been common practice to include study patients having their gastroscopy up to seven days after last intake of investigational product in gastroduodenal endoscopic studies.12,13 In the present study, the second gastroscopy was to be done no later than two days after the last intake of investigational product, and this was achieved in 84% of patients, with 97% no later than seven days. That the results of the per-protocol analysis were similar to the intent to treat population gives further support to the robustness of the study results.
The clinical significance of erosions is under debate. In a recent study it was found that patients with a baseline gastric ulcer had twice as many gastric erosions as those without ulcer (Yeomans ND, personal communication), and gastroduodenal erosions at baseline have been shown to increase the risk for endoscopically detected ulcers and clinical bleeds.36 The Lanza scale is a practical tool that combines erosions and ulcers and has been used in many studies.28,37,38 Although there was a significant difference between AZD3582 and naproxen for the Lanza scale for erosions alone both in the stomach and duodenum and for erosions and ulcers combined in the stomach only, these results did not translate into a statistically significant difference for the primary end point.
AZD3582 and naproxen were generally well tolerated, with similar adverse event rates. It is unclear whether the small but statistically significant differences between AZD3582 and naproxen in the two GSRS dimensions of reflux and abdominal pain are clinically relevant. Changes of 0.5 in the GSRS scale have been considered to be clinically significant in trials of proton pump inhibitors, but these changes represent decreases in the score from a different baseline value.39 For example, in a study of omeprazole, patients had mild discomfort at baseline (that is, 3 on the Likert scale) which decreased towards minor discomfort (2 on the Likert scale),40 whereas patients in the present study started with no discomfort (1 on the scale), but discomfort increased.
The decrease in blood pressure, possibly related to nitric oxide donation, which was initially apparent in the patients having extra blood pressure assessments, had diminished after one week. No further differences between treatment groups at subsequent visits were noted. This may have been related to the subsequent lack of specified timing of blood pressure measurements with respect to intake of investigational product; alternatively, nitrate tolerance may have occurred. The blood pressure lowering effects were generally well tolerated and subjects were typically asymptomatic.
In conclusion, AZD3582 had similar analgesic efficacy to naproxen. The 30% difference in the incidence of gastroduodenal ulcers after six weeks of treatment between AZD3582 and naproxen was not statistically significant.
APPENDIX
The STAR Multinational Study Group
Argentina: L Catoggio, E Gutfraind, J Duhau, E Mysler, J Marcos, O Messina. Brazil: M L Cardoso Pucielli, J Batista de Miranda, M Barros Bértolo, C Goldenstein Schainberg, J F Marques Neto, N R Severino. Hungary: F Gyulai, E Koó, F Szanyó, A Insperger, L Náfrádi, T Balázs, A Búvár, A Molnár, E Gömöri, J Náfrádi, Z Szekanecz, K Tarján, A Major. Mexico: R Borbon, R A Figueroa Gama, F Irazoque, L J Jara, L Lino Perez. Norway: T Forthun, S A Lonning, O Vassel, H Hövik, K Mariadasan, A Vedvik, H Fonnelöp, A Tandberg, Å N Hansen, T Tomala, B Jordet, B O Bache, A Kubak, O E Bo, R Stene, T M Pedersen, M Andersen, J F Nilsen. Poland: A Wall, J Lacki, S Mackiewicz, M Glowacka, E Kucharz, K Suchon, J Blacha, K Kwiatkowski. South Africa: S Lipschitz, M Tikly, E M van Duuren, N David, J Terblanche, C Lyddell, I Louw, G Mody, I Anderson, H Nell, M V Middle. United Kingdom: C McKinnon, H P McGoldrick, M Salman, C Harding, S Taylor, J Robinson, J Maroni, J Fraser, S Sharma, J James, C Horne, M Anderson, B Norton, B Glekin.
Acknowledgments
We thank Professor C J Hawkey, Wolfson Digestive Diseases Centre, University Hospital Nottingham, for valuable discussions on the results and for review of the manuscript. The study was supported by a grant from AstraZeneca R&D Södertälje.
REFERENCES
Footnotes
-
The members of the STAR Multinational Study Group are listed in the appendix