Article Text

Abstract
Background: Research on autoantibody formation in patients treated with TNFα inhibitors has produced contradictory results.
Objective: To study the prevalence of autoantibodies in patients with rheumatoid arthritis treated with the TNFα inhibitor infliximab.
Methods: 53 patients (48 female, 11 male) treated with infliximab for rheumatoid arthritis were followed for autoantibody production before treatment and after 14, 30, and 54 weeks. Six patients treated with etanercept were studied for comparison. The analyses included antibodies against nuclear antigens (ANA), extractable nuclear antigens, double stranded (ds)DNA (by ELISA, IIF on Crithidia luciliae for IgM and IgG, and Farr assay), nucleosomes, cardiolipin, smooth muscle, mitochondria, proteinase 3, and myeloperoxidase antigens.
Results: The number of patients treated with infliximab who developed antibodies against dsDNA of both IgG and IgM class (tested by IIF) increased significantly. The prevalence of patients positive for IgG class increased to 66% at 30 weeks and 45% at 54 weeks, and of IgM class to 85% and 70%, respectively. The titre and number of patients expressing antibodies against nucleosomes and ANA also increased significantly. The number of rheumatoid factor or anticardiolipin positive patients was stable and there was no increase in antibodies against the other antigens. A lupus-like syndrome was seen in one patient. No patient treated with etanercept developed any of these autoantibodies.
Conclusions: Patients treated with infliximab may develop anti-dsDNA antibodies of both IgM and IgG class, anti-nucleosome antibodies, and ANA, with a gradual increase until 30 weeks.
- aCL, anticardiolipin
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- anti-dsDNA, anti-double stranded DNA antibodies
- ENA, extractable nuclear antigens
- IIF, indirect immunofluorescence
- TNFα, tumour necrosis factor α
- TNFα inhibitor
- anti-dsDNA
- antinucleosome antibodies
- rheumatoid arthritis
Statistics from Altmetric.com
- aCL, anticardiolipin
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- anti-dsDNA, anti-double stranded DNA antibodies
- ENA, extractable nuclear antigens
- IIF, indirect immunofluorescence
- TNFα, tumour necrosis factor α
Patients with rheumatoid arthritis, spondylarthropathy, and Crohn’s disease treated with selective tumour necrosis factor (TNFα) inhibitors have been reported to develop autoantibodies such as antinuclear antibodies (ANA) and anti-double stranded DNA antibodies (anti-dsDNA).1–4 These are mostly of the IgM class.1,2 There have also been case reports of patients developing drug induced lupus syndrome, although the incidence has been fairly low.5 The development of autoantibodies and drug induced lupus syndrome has been described during treatment with infliximab and etanercept.1,2,5,6 Etanercept inhibits binding of both TNFα and TNFβ (lymphotoxin α) to cell surface TNF receptors, rendering TNF biologically inactive.7 Infliximab binds to both soluble and transmembrane forms of TNFα in vitro but not to lymphotoxin. Binding to soluble TNFα results in loss of bioactivity, whereas binding to membrane bound TNFα leads to cytotoxicity by complement or antibody dependent cell mediated mechanisms or both.8
TNFα is a proinflammatory cytokine produced by multiple cell types, including blood monocytes, macrophages, mast cells, and endothelial cells. It interacts with receptors on a wide variety of cells.9 It has multiple complex functional roles within the immune system including proinflammatory properties, cytotoxic effects, regulation of cell adhesion, and induction of cachexia.10–12 Consequently there are several potential mechanisms whereby anti-TNFα treatment could exert its beneficial effect in rheumatoid arthritis and other diseases. These mechanisms include decreased expression of activation markers on circulating lymphocytes and downregulation of T helper-1 cell production, resulting in a net overall decrease in TNFα expression.13,14 Reports have suggested that TNFα can induce not only apoptotic but also anti-apoptotic signals.15,16 Interestingly, TNFα neutralisation ameliorates the severity of a murine model of ileitis by interrupting intestinal epithelial cell apoptosis while inducing apoptosis in lamina propria mononuclear cells.17 Thus interference with apoptosis is a possible mechanism whereby anti-TNFα treatment exerts its effect systemically, even though infliximab does not appear to alter the anti-apoptotic state of the synovium.18
The inconsistencies between reports on the prevalence of various autoantibodies, including analyses of anti-nucleosome antibodies and of the different isotypes expressed, in patients treated with TNFα inhibitors encouraged us to undertake a prospective long term follow up study on rheumatoid patients treated with the selective TNFα inhibitor infliximab. The development of autoantibodies was followed for 54 weeks. As a comparison we also followed six patients treated with etanercept.
METHODS
Patients
Fifty nine patients (48 female and 11 male) with rheumatoid arthritis according to the ACR criteria19 were consecutively recruited into the study. Fifty three were treated with infliximab (3 mg/kg body weight at inclusion, after two weeks and eight weeks, and thereafter at eight week intervals); and six were treated with etanercept (25 mg twice weekly). Demographic data on these patients are presented in table 1.
Demographic data of the patients in the study
Procedures
Blood samples were collected from patients before treatment and after 14, 30, and 54 weeks. The sera were stored at −80° until analysis. The autoantibodies analysed included: rheumatoid factor (RF) by Rose–Waaler, antinuclear antibodies (ANA) by indirect immunofluorescence (IIF) on rat kidney, anti-smooth muscle antibodies and antimitochondrial antibodies by IIF on rat tissue (using an in-house protocol), antihistone antibodies, anti-extractable nuclear antigens (ENA: anti-Sm, RNP, SSA, SSB, Scl-70, and Jo-1), anti-proteinase 3, antimyeloperoxidase (anti-MPO), and anticardiolipin (aCL, IgG) antibodies (Autozyme, Cambridge Life Science, Cambridge, UK) by enzyme linked immunosorbent assay (ELISA). Antibodies against double stranded DNA (ds-DNA) were analysed by IIF on Crithidia luciliae coated slides for both IgM and IgG (Immunoconcept, Sacramento, California, USA), by ELISA (Varelisa: Pharmacia Diagnostics, Freiberg, Germany), and by the Farr assay (Ortho, Amersham, UK). Antinucleosome antibodies (IgG class) were analysed by ELISA (Euroimmun, Luebeck, Germany).
Strategy
All 53 patients treated with infliximab were assessed for RF, ANA, ds-DNA (IgG class) and antinucleosome antibodies. The first 27 patients included were also assessed for ds-DNA (IgM class) and aCL antibodies. Anti-DNA ELISA tests and Farr assays were done only on the first 20 patients recruited. At 54 weeks there were serum samples from only 45 patients because seven were prematurely withdrawn from treatment, for one individual there was no serum available for any analyses at 54 weeks, and in another two there was no serum for antinucleosome antibodies at 54 weeks. In three individuals antinucleosome antibodies were not analysed at any point because of lack of sera. Furthermore, for some of the other analyses there was no serum available; this loss of sera was random. The six patients receiving etanercept were assessed for all autoantibodies except antinucleosome antibodies.
Statistics
The statistic analyses were carried out using non-parametric tests: Kruskall–Wallis one way analysis of variance for independent samples and Friedman two way analysis of variance by ranks for related samples. A χ2 test for trends was used for testing categorical data.
RESULTS
Analyses of autoantibodies in patients treated with infliximab
The frequency of presence of anti-dsDNA, antinucleosome, and ANA antibodies increased significantly (χ2 for trends) during treatment with infliximab (table 2). Two patients had either IgG and IgM antibodies against dsDNA, at a low titre, before treatment. The proportion of patients positive for IgG class anti-dsDNA antibodies assessed by the Crithidia luciliae test increased to 66% at 30 weeks and 45% at 54 weeks, and for IgM class to 85% and 70%, respectively (tables 2 and 3). In the 27 patients tested for both IgG and IgM class anti-dsDNA antibodies, the concordance between the antibodies was high. Patients having IgM antibodies were also positive for IgG antibodies in 94% (at 14 weeks), 86% (at 30 weeks), and 81% (at 54 weeks), respectively. At inclusion five individuals were positive for antinucleosome antibodies and this number increased significantly to 13 at 30 weeks and remained at that level. The concordance between positive antinucleosome antibodies and IgG class anti-ds DNA antibodies at 30 weeks was 85% and at 54 weeks 78% (table 2), and of IgM class it was 88% and 86% (table 3), respectively. The concordance between positive ANA and anti-dsDNA antibodies of IgM and IgG isotype or antinucleosome antibodies was high, at 82–90% at 30 weeks and 88–100% at 54 weeks. The anti-DNA ELISA was only positive in one of the 20 patients tested after 30 weeks of treatment, while the Farr assay was positive in five patients, all of whom were IgG positive in the Crithidia luciliae test. The numbers of RF positive and aCL positive patients were stable throughout the study (tables 2 and 3).
Frequency of antinuclear antibodies, anti-ds-DNA of IgG subclass, antinucleosome antibodies and rheumatoid factor (RF) in 53 patients with rheumatoid arthritis treated with infliximab
Frequency of anti-ds-DNA of IgM subclass analysed by immunofluorescence, anti-DNA analysed by ELISA and Farr assay and anticardiolipid antibodies (aCL) of IgG class in patients with rheumatoid arthritis treated with infliximab
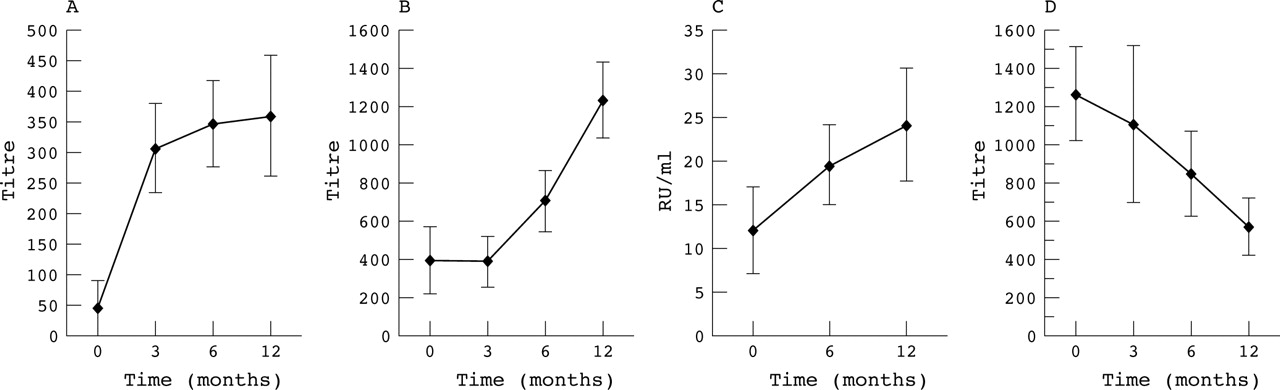
In most patients who developed anti-dsDNA antibodies of both IgG (fig 1A) and IgM types, the titres were high and increased significantly both as a group (Kruskal–Wallis one way analysis of variance, p<0.0001 and p<0.05, respectively) and on an individual level (Friedman two way analysis of variance, p<0.0001 and p<0.0001) at 30 weeks; thereafter the titres declined, although not significantly. This pattern was the same for the ANA titres in that they increased until 30 weeks (Kruskal–Wallis one way analysis of variance, p<0.001; Friedman two way analysis of variance, p<0.001; fig 1B) and were thereafter stable (table 2). The titres of antinucleosome antibodies also increased (Kruskal–Wallis one way analysis of variance, p<0.01; Friedman two way analysis of variance, p<0.0001) (fig 1C), while the titres of RF decreased over time (Kruskal–Wallis one way analysis of variance, p<0.001; Friedman two way analysis of variance, p<0.05) (fig 1D). The anti-dsDNA titre measured by ELISA increased, although all values were below the cut off value (data not shown). There was no increase in the number of individuals positive for antibodies against histones, ENA, proteinase3, MPO, smooth muscle, or mitochondria.

{kind=link}
Antibody formation in infliximab treated patients with rheumatoid arthritis. (A) The titres of anti-double stranded DNA antibodies (anti-dsDNA) of IgG class (53 patients; Kruskal–Wallis one way analysis of variance, p<0.0001; Friedman two way analysis of variance, p<0.0001). (B) The titres of antinuclear antibodies (ANA) (53 patients; Kruskal–Wallis one way analysis of variance, p<0.001; Friedman two way analysis of variance, p<0.001). (C) Antinucleosome antibodies of IgG class (50 patients; Kruskal–Wallis one way analysis of variance, p<0.01; Friedman two way analysis of variance, p<0.0001). (D) Rheumatoid factor titres (53 patients; Kruskal–Wallis one way analysis of variance, p<0.001; Friedman two way analysis of variance, p<0.05).
Of the seven individuals who withdrew from the treatment prematurely (that is, before 54 weeks) six did so because of side effects: three with allergy, one with anaphylaxis, and one with infection. The other withdrawal was because of the development of an SLE syndrome (with leucopenia, C3 and C4 consumption, myalgia, and arthritis) with antihistone antibodies. This patient recovered within a few weeks after stopping the treatment, but anti-dsDNA antibodies of IgG isotype remained positive at a high titre 20 months later. Another of the patients had IgG class anti-dsDNA antibodies eight months after withdrawal. Five of the six individuals with side effects had anti-dsDNA antibodies of IgG class (χ2 = 4.02, p<0.05). In two of these cases withdrawal from the drug because of side effects was combined with a lack of efficacy, and another patient withdrew purely because of lack of efficacy. A further patient with anti-dsDNA antibodies and antinucleosome antibodies was withdrawn just after 54 weeks because of the development of a lupus-like syndrome (leucopenia, rash, arthralgia, and vasculitis on the finger tips).
There were no effects of methotrexate treatment, drug dosage, or corticosteroid use on the development of autoantibodies. Patients with ANA antibodies at 30 weeks had a significantly higher 28 joint disease activity score (DAS28) at 54 weeks (p<0.05).
Analyses of autoantibodies in patients treated with etanercept
No patients treated with etanercept developed any of the autoantibodies tested for in this study.
DISCUSSION
The frequency of autoantibodies against ANA, ds-DNA (of both IgG and IgM isotype), and antinucleosome increased significantly during treatment with infliximab in patients with rheumatoid arthritis. It has been suggested that antinucleosome antibodies are a useful marker for diagnosis and disease activity assessment, particularly in anti-dsDNA negative patients with systemic lupus erythematosus.20,21 This antibody has not previously been described in patients with rheumatoid arthritis.21 In the present study five of the 50 patients (10%) were positive for antinucleosome antibodies before treatment. Antinucleosome antibodies have been found to develop in patients with both rheumatoid arthritis and ankylosing spondylitis treated with infliximab.2 These results are further supported by the recent findings of increased levels of nucleosomes in patients treated with infliximab.22
The number of ANA positive patients on entry to our study was as described for rheumatoid arthritis (about 25%); however, the numbers increased, as did the titres, during infliximab treatment, while the number of RF positive patients remained the same with decreasing titres. The increase in antibodies against ANA was in agreement with previous findings2,23 but the increase in anti-dsDNA and antinucleosome antibodies was greater in this study than in those reports. In previous studies on rheumatoid arthritis24 or Crohn’s disease,3 anti-dsDNA antibodies were only analysed in ANA positive patients, and this might have been responsible for the reduced frequencies. The development of autoantibodies during infliximab treatment in the present study and in other reports2,6 does not seem to have the same underlying mechanism as the development of lupus-like syndromes induced by other drugs, because antihistone antibodies were found in only one patient.
In this study, two patients treated with infliximab developed a lupus-like syndrome, and on the whole patients with side effects were more likely to develop these autoantibodies. Antinucleosome antibodies of the IgG class are considered to be a more sensitive marker of SLE than anti-dsDNA antibodies, as they occur at an earlier stage in the evolution of the disease.25 Although there was a significant relation between anti-dsDNA antibodies of IgG and IgM classes and antinucleosome antibodies, anti-dsDNA antibodies of IgG class were most common and were not preceded by antinucleosome antibodies in all cases.
We were unable to identify the suppressive effect on autoantibody production by methotrexate treatment that was suggested by Boehm et al.26 However, the number of cases was small when stratified for methotrexate treatment. Patients with ANA antibodies had significantly higher disease activity scores (DAS28) at 54 weeks. This could suggest that they also produced autoantibodies that blocked the therapeutic effects of infliximab.
An increased frequency of aCL antibodies has been reported in patients treated with infliximab or etanercept.5,27 In the present study we did not find any increase in the prevalence of these antibodies. However, there is great variability in the methods of analysis of aCL, which could contribute to the contradictory findings.28,29
Only six individuals were treated with etanercept and none developed autoantibodies or any side effects. There have, however, been reports of a lupus-like syndrome as a side effect in patients receiving etanercept.5,6 An increased production of autoantibodies during treatment with etanercept has not been reported at high frequency.30 In one study, only 5% of cases were found to develop anti-dsDNA antibodies measured by radioimmunoassay.30 However, 67% of the patients developing these antibodies were ANA negative.
In vivo neutralisation of TNFα in rheumatoid arthritis, as demonstrated here, has a profound stimulatory effect on humoral immunity to DNA and other nuclear antigens. This effect may be accounted for by several possible mechanisms, including interruption of apoptosis and downregulation of T-helper cell activity. The induction of autoimmunity to nuclear antigens may also reflect inhibition of cytotoxic cells with the potential to suppress autoreactive B cells, which has been proposed as an explanation for SLE-like autoimmunity in chronic graft versus host disease.31 Another possibility is that induction of autoimmunity to nuclear antigens reflects interference by anti-TNFα with the capacity of TNFα to terminate lymphocyte responses by promoting activation induced cell death in CD8+ T cells.32 It is also possible that TNFα may directly modulate the immunogenicity of DNA through effects on serum amyloid P and complement factors C1q and C4b which bind chromatin DNA in apoptotic bodies and account for the clearance of DNA. Absence of these mediators in mice leads to the development of antinuclear autoimmunity and lupus-like disease.33,34 It is interesting in this context that combined inactivation of TNFα and interleukin 6 prevents induction of acute phase proteins such as serum amyloid P, pointing to a pathway whereby reduced TNFα may aid in the development of lupus.35 Although there are several possible mechanisms underlying anti-dsDNA, antinucleosome antibodies, and ANA formation in rheumatoid patients treated with TNFα inhibitors, it is apparent that these autoantibodies reflect a selective development of antibodies to one particular type of intracellular antigen (that is, originating from the nucleus). Thus it also remains to be explained why the altered immune reactivity provoked by anti-TNFα treatment does not induce autoantibodies to cytoplasmic antigens.
In summary, we have shown that patients treated with infliximab developed autoantibodies such as ANA and anti-dsDNA of both IgG and IgM class measured by Crithidia luciliae, and also antinucleosome antibodies. The increase was most evident in patients with side effects. Methotrexate treatment did not suppress the autoantibody production.
Acknowledgments
We gratefully acknowledge the staff at the Division of Rheumatology and Hans Stenlund BSc, PhD, Department of Public health and Clinical Medicine, Umeå University, for statistical advice.