Article Text

Abstract
OBJECTIVE This study was performed to assess whether there is any change in the T cell cytokine pattern in early rheumatoid arthritis (RA) patients treated with methotrexate (MTX) and whether the lymphocytic cytokine pattern correlates with disease activity.
METHODS Eight patients with RA (disease duration < six months) were studied serially before, after three, and after six to nine months of treatment with MTX for the cytokines tumour necrosis factor α (TNFα), interferon γ (IFNγ), interleukin 4 (IL4) and interleukin 10 (IL10) by intracellular staining of T cells derived from peripheral blood. Response to treatment was assessed by the modified disease activitiy score.
RESULTS The clincial response was accompanied by a significant decrease of TNFα positive CD4+ T cells from a median of 8.53% (interquartile range 5.83–10.91%) before treatment to 6.17% (2.15–6.81%) after six to nine months of treatment (p=0.021). Inversely, IL10 positive T cells increased from a median of 0.65% (interquartile range 0.6–0.93%) to a median of 1.3% (1.22%-1.58%) after six to nine months of treatment (p=0.009). No significant change in the percentage of INFγ positive T cells and a small decrease of IL4 positive T cells during treatment were observed. The percentage of IL4 positive CD4+ T cells before treatment correlated with disease activity after six to nine months (r= −0.7066; p=0.05).
CONCLUSIONS During treatment of RA with MTX the percentage of TNFα producing T cells decreases whereas that of IL10 producing T cells increases. This may affect macrophage activation and, therefore, may represent a regulatory mechanism relevant to disease remission. Furthermore, the percentage of IL4 positive CD4+ T cells at disease onset may be a useful prognostic marker.
- tumour necrosis factor α
- interleukin 10
- rheumatoid arthritis
- methotrexate
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a systemic inflammatory condition the cause of which is unknown. Methotrexate (MTX) is currently the most widely prescribed disease modifying anti-rheumatic drug (DMARD) in RA because of its high efficiency and early onset of action. The molecular basis of the effects of low dose MTX in RA is not clear but it seems probable that anti-inflammatory effects are more important than sole inhibition of DNA synthesis (reviewed by Bondeson1).
In RA synovitis the proinflammatory cytokines tumour necrosis factor α (TNFα) and interleukin 1β (IL1β), which are locally produced by macrophages are undoubtledy important effector molecules. Several studies suggest that during MTX treatment a down regulation of monocyte activation takes place: the production of monokines such as TNFα and IL1β in synovial membrane, synovial fluid and peripheral blood is reduced.2-4 Furthermore, a decrease of interleukin 6 (IL6) concentrations has been reported in serum in responders to MTX treatment.5 ,6
The findings from all these studies demonstrate a decrease of the total inflammatory load during MTX treament. We and others showed that in RA synovitis a local T helper 1 (TH1) cytokine pattern predominates,7 ,8 which, although the number of lymphocytes in the inflamed synovium is rather small, could indeed cause macrophage activation via cytokines. Thus, anti-inflammatory effects of MTX in RA could well be the result of effects on lymphocytes, which then in turn may affect macrophage activity. Therefore, we studied prospectively the lymphocytic cytokine pattern in patients with early RA before and during treatment with MTX.
Methods
PATIENTS
Patients for this study were attenders of the rheumatology outpatient clinic of the Benjamin Franklin Hospital, Berlin. To be included in the study patients had to fulfill the following criteria: RA had to be diagnosed according to the revised 1987 ACR criteria for RA, onset of RA had to be less than six months before study entry, patients were not treated with DMARDs or glucocorticoids before, and patients had to have active disease requiring initiation of a DMARD treatment. Six of eight patients had a positive rheumatoid factor. All patients were started on treatment with MTX 15 mg intramuscularly per week, and the dose was reduced to 10 mg if side effects occurred. The intramuscular route was chosen to guarantee stable drug levels. Up to 7.5 mg of prednisolone per day was allowed.
At three time points blood was taken for cytokine analysis: at study entry before treatment with MTX, at three months, and at six to nine months after the start of MTX treatment. The modified disease activity score (mDAS), which includes the number of tender and swollen joints (using the 28 joint count), erythrocyte sedimentation rate (ESR), and the general health status,9 was used to assess disease activity at each of these visits.
INTRACELLULAR CYTOKINE STAINING OF PERIPHERAL BLOOD T CELLS AND ANALYSIS BY FLOW CYTOMETRY
Peripheral blood (PB) mononuclear cells (MNC) were separated by Ficoll-paque (Pharmacia, Uppsala, Sweden) and stored in liquid nitrogen until use. After thawing and short stimulation the cells were stained for intracellular cytokines and cytokine positive T cells quantified by flow cytometry (Becton Dickinson, CA) as described before.10 Briefly, 1 × 106 PB MNC were cultured for six hours in the presence 5 ng/ml PMA (phorbol 12-myristate 13- acetate; Sigma, St Louis, MO) and 1 ng/ml ionomycin (Sigma, St Louis, MO), 2.5 μM monensin (Sigma, St Louis, MO) was added during the last two hours, the cells were fixed, stained with antibodies directed against cytokines and against the T cell surface markers CD3 and CD8, and subsequently analysed by flow cytometry.
Because stimulation with PMA/ionomycin induces a reduction of CD4 expression on the cell surface CD4+ T cells were indirectly identified by gating on CD3 positive but CD8 negative lymphocytes. For triple staining, cells were incubated with PerCP-labelled anti-CD3 (Becton Dickinson, San Diego, CA), cy5-labelled anti-CD8 (for this cy-5 (Amersham, Braunschweig, Germany) was labelled to purified anti-CD8), and either with FITC-labelled antihuman IFNγ mAb, FITC-labelled antihuman TNFα mAb, PE-labelled antihuman IL10 mAb, or PE-labelled antihuman IL4 mAb (all Pharmingen, San Diego, CA). After gating either on CD3+/CD8 positive or CD3+/CD8 negative (CD4+) lymphocytes, data were analysed using CELLQuest software and displayed as dot plots of FITC (x axis) and PE (y axis) fluorescence (four decade log scales). Quadrant markers were positioned to include > 99% of control Ig staining cells in the lower left quadrant.
STATISTICS
As the numbers studied were small medians and interquartile ranges (25th–75th percentile) of cytokine positive cells are given. For comparison of medians the Mann-Whitney U test was applied. All statistics including Spearman's rank correlation were calculated using the SPSS computer program.
Results
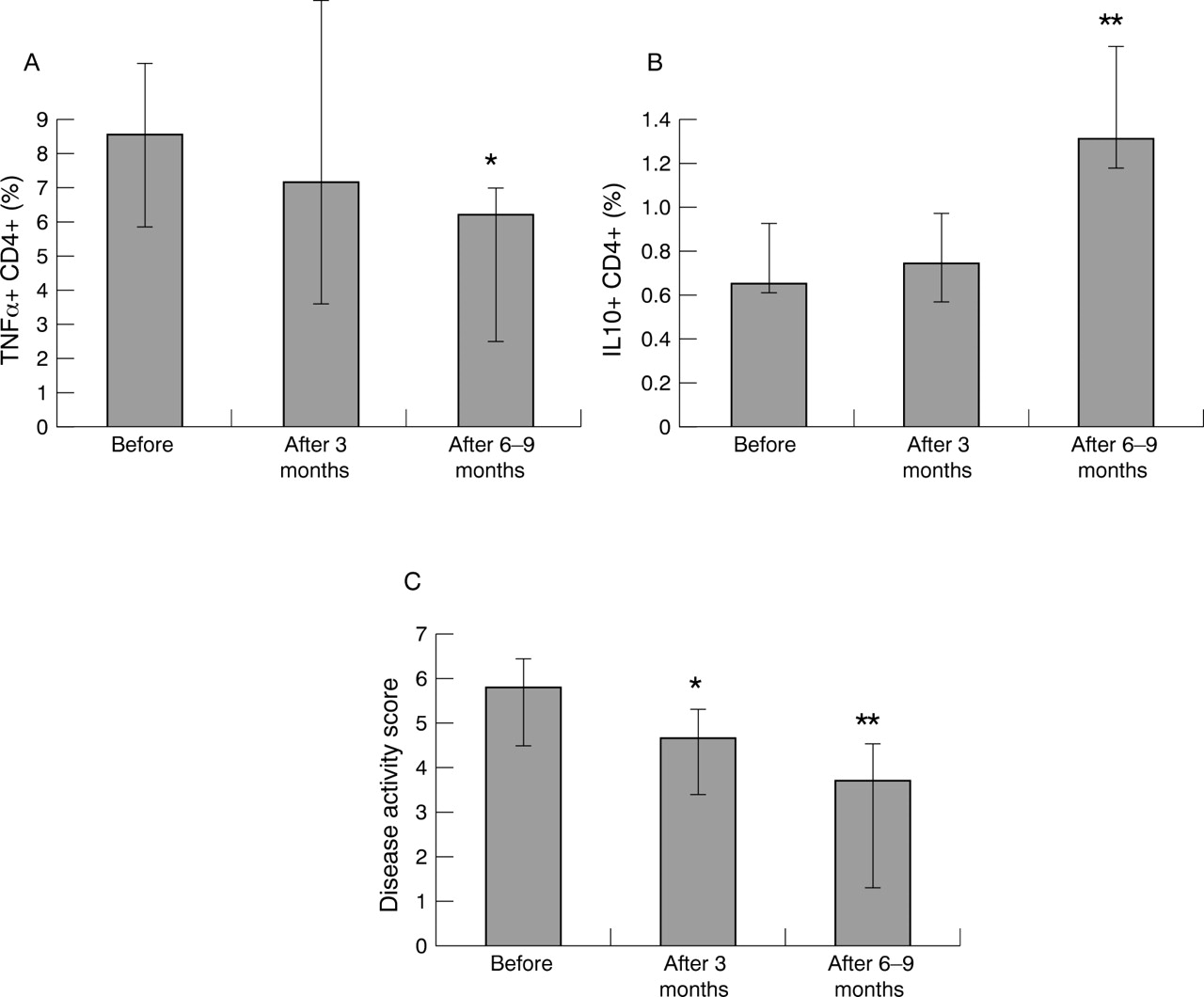
There was a significant clinical improvement of RA during treatment with MTX as judged by a decrease in the mDAS from before treatment (median mDAS 5.75, interquartile range 4.9–6.9) to 4.6 (4.1–5.4) after three months (p=0.035) to 3.6 (1.8–4.8) after six to nine months of treatment (p=0.005) (fig 1C).
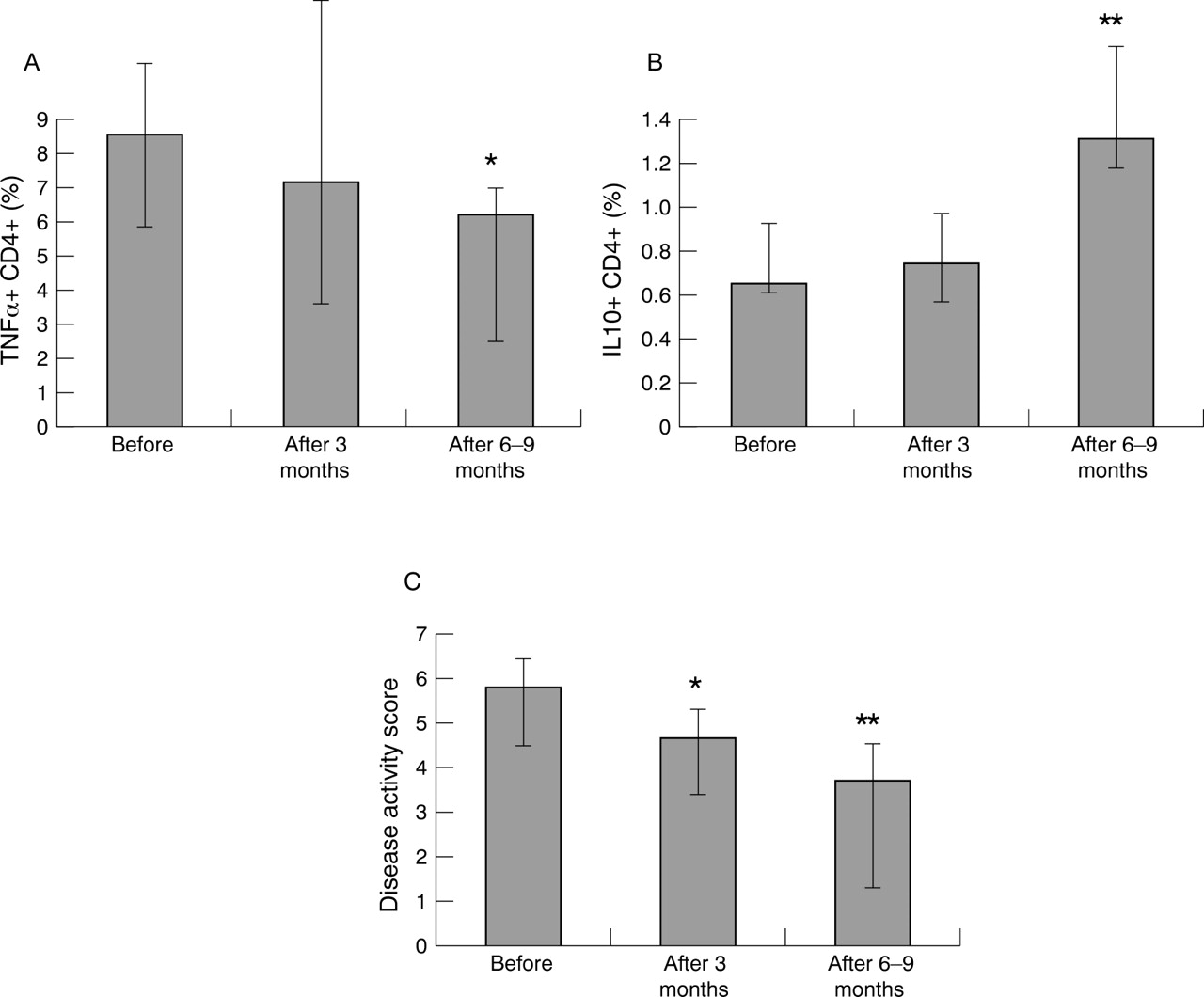
Percentage of (A) TNFα and (B) IL10 positive CD4+ T cells in eight patients with early RA expressed as median (boxes) and interquartile range (bars) before, after three months, and after six to nine months of treatment with MTX. The modified disease activity score (mDAS) also expressed as median (boxes) and interquartile range (bars) is shown in (C). * p<0.05 versus before treatment. **p<0.01 versus before treatment.
During treatment with MTX the percentage of TNFα positive CD4+ lymphocytes decreased from a median of 8.53% (interquartile range 5.83–10.91%) TNFα positive CD4+ T cells before, to 7.11% (interquartile range 3.90–12.04%) after three months, and 6.17% (interquartile range 2.15–6.81%) after six to nine months of treatment (p=0.021 for the percentage beforev after six to nine months) (fig1A). Inversely, IL10 positive T cells increased from a median of 0.65% (interquartile range 0.6–0.93%) to a median of 0.74% (interquartile range 0.52–0.97) after three months to 1.3% (1.22%-1.58%) after six to nine months of treatment (p=0.009 for the median beforev after six to nine months of treatment) (fig 1B). In the CD8 subset a decrease in the number of TNFα positive cells was also observed, however, this was not significant (data not shown). The findings cannot be explained by technical problems. In three patients the same blood sample was processed and analysed on three different occasions to assess variation of results attributable to laboratory handling (including intra-assay variation). The estimated coefficient of variation for TNFα of 8.3% was small.
During treatment with MTX there was a small but non-significant decrease in the percentage of IL4 positive T cells (data not shown). Of more importance, however, there was a clear negative correlation between IL4 positive CD4+ T cells before treatment and disease activity after six to nine months (r= −0.707; puncorr.=0.05) (fig 2). The percentage of IFNγ positive T cells did not change significantly during treatment with MTX (data not shown).

{kind=link}
{kind=link}
Correlation of disease activity score (mDAS) after six to nine months of treatment with methotrexate in eight patients with early RA (each filled box indicates one patient) with the percentage of IL4 positive CD4+ T cells before treatment.
Discussion
The most salient result of our study is a significant decrease in the percentage of TNFα positive CD4+ T cells and a significant increase of IL10 positive T cells in patients with early RA who showed a clinical response to treatment with MTX. The change in these cytokines was already seen after three months but was more pronounced after six to nine months of treatment. In contrast, no significant change in the percentage of IFNγ or IL4 positive T cells was observed.
Whether the TNFα shift we observed is a primary event in disease remission during treatment with MTX or secondary to disease remission cannot be answered by our study. The dramatic therapeutic effect of anti-TNFα treatments seen in RA patients suggests a relevant role of TNFα in inducing disease remission. It is intriguing to speculate that T cell cytokine secretion is central to disease activity in RA and changes of T cell cytokines precede both disease remission and disease flare. The function of TNFα positive CD4+ T lymphocytes is yet to be defined, although this subset has been recognised for some time. Strong support for this hypothesis comes from MTX treated mice with experimental arthritis. In these mice, there is a strong reduction of TNFα production by splenic T cells but not by macrophages during MTX treatment.11
From animal models it is also known that IL10 secreted by lymph node cells is very low at onset of arthritis but at later stages IL10 levels increase steadily over time before remission occurs.12This is in parallel to the IL10 increase seen in our patients who respond clinically. Recently it has been suggested that T cell derived IL10 might be of important relevance for the immunoregulatory functions of T cells.13 Thus, the increase of IL10 producing T cells may have led to a reduction of TNFα producing T cells. However, from our data we cannot judge whether the decrease of TNFα and the increase of IL10 are dependent or independent of events.
Clinical response to treatment in RA patients and changes of the T cell cytokines IFNγ and IL4 have been the subject of recent studies.14 ,15 In the first study peripheral blood mononuclear cells were investigated ex vivo by PCR for IFNγ, IL2, IL4 and IL10 gene expression. No clear differences were found between RA patients treated with MTX and RA patients without treatment. Only after in vitro stimulation with phytohaemagglutinin in the presence of MTX an increase of IL10 gene expression was observed. However, the source of IL10, whether T cells or non-T cells, could not be identified by PCR.14 In the second study, peripheral blood T cells from RA patients treated with sulfasalazine were investigated longitudinally by intracellular cytokine staining. Similar to our results, the percentage of IFNγ or IL4 positive T cells did not correlate with disease activity scores.15 In contrast with these studies we included TNFα and IL10 produced by T cells in our analysis, which seems to be more relevant to RA disease remission than a mere change of IFNγ or IL4 producing T cells.
The second important finding of our study is that the percentage of IL4 positive CD4+ T cells at disease onset seems to predict disease remission during treatment with MTX. There was a clear negative correlation between the percentage of IL4 positive CD4+ T cells before treatment with MTX and mDAS after six to nine months. This means that the likelihood of responding to treatment increases if the initial percentage of IL4 positive T cells is high. Our data are in line with a recent report showing a correlation of an initially low IFNγ/IL4 ratio with an improvement of the disease activity score after nine months of treatment with sulfasalazine or hydroxychloroquine in patients with RA.15 Thus, IL4 may serve as a prognostic marker in RA and, moreover, could be used in its ability to predict disease remission independently of the DMARDs used.
Although the number of patients studied was small and our findings need to be confirmed in a larger study before definite conclusions are drawn our data support the concept of lymphocytes and their cytokines as important players in RA orchestrating monocytes and the inflammatory process.