Article Text

Abstract
OBJECTIVE To investigate possible differences in Th1 and Th2 cytokine mRNA expression in the synovial tissue (ST) of patients with rheumatoid arthritis (RA) and seronegative spondyloarthropathies (SpA) with diagnostic and/or pathogenic interest.
METHODS Eleven RA patients and 14 SpA patients (10 with undifferentiated spondyloarthropathy (USpA), two with ankylosing spondylitis (AS) and two with psoriatic arthritis (PsA)) were included. Th1 (interferon γ, interleukin 2) and Th2 (interleukin 4, interleukin 5 and interleukin 10) cytokine mRNA levels from arthritic knee ST were quantified by using an optimised polymerase chain reaction method with a computerised analysis system. Protein levels of proinflammatory cytokines (interleukin 1, tumour necrosis factor α and interleukin 6) in synovial fluid were quantified with a specific ELISA test.
RESULTS Th1 cytokines were detected in all of RA ST samples in contrast with 58% (interferon γ) and 71% (interleukin 2) of SpA samples. Th2 cytokines were expressed in 90% of RA ST samples, but the findings in SpA were interleukin 10 in 90%, interleukin 4 in 60% and interleukin 5 in 40% of ST samples. However, when the mRNA levels of each cytokine were quantified and corrected for T cell mRNA levels, only interferon γ levels were significantly higher in RA than in SpA (p<0.003). Thus, the Th1/Th2 cytokine ratio in RA was fivefold that of SpA. Synovial fluid interleukin 1β concentrations were higher in RA than in SpA (p<0.05); there were also higher synovial fluid levels of tumour necrosis factor α in RA than in SpA, but without statistical significance.
CONCLUSION This study has detected both Th1 and Th2 cytokine gene expression in ST from RA and SpA patients. Synovium interferon γ mRNA levels and SF interleukin 1β protein levels were significantly higher in RA than in SpA, so reflecting the known proinflammatory activity of interferon γ through macrophage activation. Thus, the Th1 (interferon γ)/Th2 (interleukin 4) ratio is significantly higher in RA than in SpA ST. These data confirm previous studies on ST Th1/Th2 balance in RA and extend previous work in comparing ST RA with subgroups of SpA distinct of ReA.
- T cell cytokines
- rheumatoid arthritis
- seronegative spondyloarthropathies
- undifferentiated spondyloarthropathies
Statistics from Altmetric.com
- T cell cytokines
- rheumatoid arthritis
- seronegative spondyloarthropathies
- undifferentiated spondyloarthropathies
Rheumatoid arthritis (RA) and the so called seronegative spondyloarthropathies (SpA)1 (including the subgroups of ankylosing spondylitis (AS), reactive arthritis (ReA), undifferentiated spondyloarthropathies (USpA) and psoriatic arthritis (PsA)) are both characterised by chronic synovial inflammation. In these rheumatisms a similar synovial pathology is observed: the synovium is infiltrated by T cells, plasma cells and macrophages, although some distinguishing immunohistological features have been suggested.2
Multiple studies showed that macrophage derived cytokines (interleukin 1 (IL1), tumour necrosis factor α (TNFα), interleukin 6 (IL6) and interleukin 8 (IL8)) are powerful local protein mediators of major importance in inflammation and joint destruction in RA.3 ,4 This knowledge has recently led to successful clinical therapeutic trials with anti-cytokines.5 ,6However, it has proved difficult to find T cell derived cytokines, such as interferon γ (IFNγ), interleukin 2 (IL2) or interleukin 4 (IL4), in RA synovium,7-9 although the relevance of T cells in the pathogenesis of RA and SpA has been demonstrated in experimental animal models.10 ,11
T helper (Th) cells are divided into two subsets based on their cytokine production profiles: Th1 cells mainly secrete IFNγ and IL2, whereas Th2 cells generally produce IL4, IL5 and IL10. Studies using animal models indicate that Th1 cytokines promote the development of autoimmune disorders, whereas the Th2 pattern may attenuate these diseases.12 The Th1 and Th2 cytokine balance has attracted great interest as it is hypothesised that the degree of polarisation and heterogeneity of T cell lymphocytes may be important in the initiation and perpetuation of synovial inflammation.13 ,14 By using highly sensitive techniques, several investigators have found a preferential activation of Th1 cells in rheumatoid synovium, suggesting that Th1 rather than Th2 cytokines are involved in the pathogenesis of the disease.15-18However, the rheumatoid synovium is not a rich source of T cell cytokines, and the T cell primacy in RA has been questioned on the basis of their hyporesponsiveness in synovium of early and chronic RA.19
On the other hand, there are few studies on cytokines in patients with SpA, and most of these are devoted to ReA.17 ,18 ,20-22In a previous work we have shown that serum concentrations of IL6, TNFα and IFNγ were lower in AS than in RA patients; even so, IL6 levels correlated with the activity and severity of AS.23Recently, we have also found a similar pattern of macrophage-fibroblast derived cytokine (IL1β, IL6, IL8, TNFα and transforming growth factor β (TGFβ)) gene expression in synovium of patients with RA and SpA. However, it was difficult for us to find synovial expression of T cell derived cytokines in either disease.24
Studies on Th1/Th2 cytokine gene expression comparing SpA and RA synovial tissue are scarce. In previous reports, a predominant Th2 cytokine profile has been found in synovium of ReA,17 ,18although a recent work with quantitative PCR has not confirmed these findings.25 By immunohistological techniques it has been demonstrated an increased Th1/Th2 cytokine ratio in RA synovium when compared with that of ReA.21 ,22 However, there are no studies on the Th1/Th2 cytokine pattern in USpA synovium, one of the most prevalent forms of SpA.26 Neither are there any studies on IL5, a Th2 cytokine probably implicated in the stimulation of B cells to produce IgA.27
In this study we analysed the mRNA expression of Th1 (IFNγ, IL2) and Th2 (IL4, IL5 and IL10) cytokines in synovium of RA and SpA (predominantly USpA) patients using an optimised quantitative PCR method, with the aim of detecting differences of pathogenic or diagnostic interest, or both, between the two diseases. The possible correlation between these T cell derived cytokine patterns in synovium and clinical and biological parameters of disease activity, including the levels of the proinflammatory macrophage derived cytokines (IL1β, IL6, TNFα) in synovial fluid, was also investigated.
Methods
PATIENTS
A total of 29 patients were included in the study: 12 suffered from RA (1987 ARA criteria); eight of them with positive rheumatoid factor (>30 IU/l, nephelometry). Disease duration was (mean (SD)) 34 (34) months. The remaining 17 patients suffered from SpA, with 46 (68) months of disease duration. Twelve of them had USpA (ESSG criteria)28 (eight HLA-B27 positive, by microlymphocytotoxicity test); three had AS (New York criteria, all HLA-B27 positive), and two had psoriatic arthritis with peripheral and axial involvement (both B27 negative). Both RA and SpA patients were outpatients with active disease and knee synovitis. RA patients were not treated with slow acting anti-rheumatic drugs or prednisone in a dose higher than 5 mg/day during the three months that preceded their inclusion in this study. SpA patients were treated only with non-steroidal anti-inflammatory drugs (NSAIDs).
The ethical committee of the Hospital Clinic of Barcelona approved the study.
Blood and synovial tissue samples were obtained at clinical assessment. Clinical peripheral synovitis activity was measured according to Thompson's articular index.29 Eight synovial knee tissue samples were obtained from each patient using a needle biopsy (Parker and Pearson). The inflammatory synovitis was confirmed in each case by haematoxylin and eosin staining. The synovial tissue samples were dipped in guanidinium isothiocyanate buffer30 and immediately frozen in liquid nitrogen.
RNA ISOLATION FROM SYNOVIAL TISSUE AND QUANTITATIVE REVERSE TRANSCRIPTASE-PCR ANALYSIS
Total RNA was isolated from synovial tissue by the guanidinium isothiocyanate method.30 First strand cDNA synthesis was performed using random hexamers as primers and MMLV reverse transcriptase at 42°C for 60 minutes. cDNA (1 μl) was used in a PCR mixture containing 67 mM TRIS-HCl, pH 8.8, 16 mM (NH4)2SO4, 0.01% Tween 20, 1.5 mM MgCl2, 0.1 mM of each deoxynucleotide triphosphate, 0.4 mM of either β2 microglobulin (β2M), CD3, IFNγ, IL2, IL4 IL5 or IL10 specific primers (Clontech Laboratories, Palo Alto, CA) and 2.5 U Taq polymerase. Amplification of cDNA sequences was carried out in a PTC-100 Programmable Thermal Controller (MJ Research, Watertown, MA). The optimised conditions were 35 cycles of denaturation at 94°C for 45 seconds, annealing at 60°C for 45 seconds, and extension at 72°C for two minutes (except 30 seconds for IL2 and IL5), followed by a final extension step at 72°C for eight minutes. Negative controls (without target DNA) were included in each experiment to exclude cross contamination. β2M DNA was used as a positive control for the presence of total mRNA, and CD3 DNA for the presence of T cell mRNA. All samples were analysed in duplicate and yielded similar results; one of the duplicates was further used for quantification.
PCR products were separated by agarose gel electrophoresis and visualised by ethidium-bromide staining. The resulting fluorescent bands were video-digitalised by a GelDoc 1000 UV-Gel camera and quantified by a computerised analysis system using Molecular Analyst, version 1.4 software (Bio-Rad, Richmond, CA). Previously, the identity of each PCR product was confirmed by Southern hybridisation using sequence specific, digoxigenin labelled (Boehringer Mannheim, Germany) positive control cDNA (Clontech).
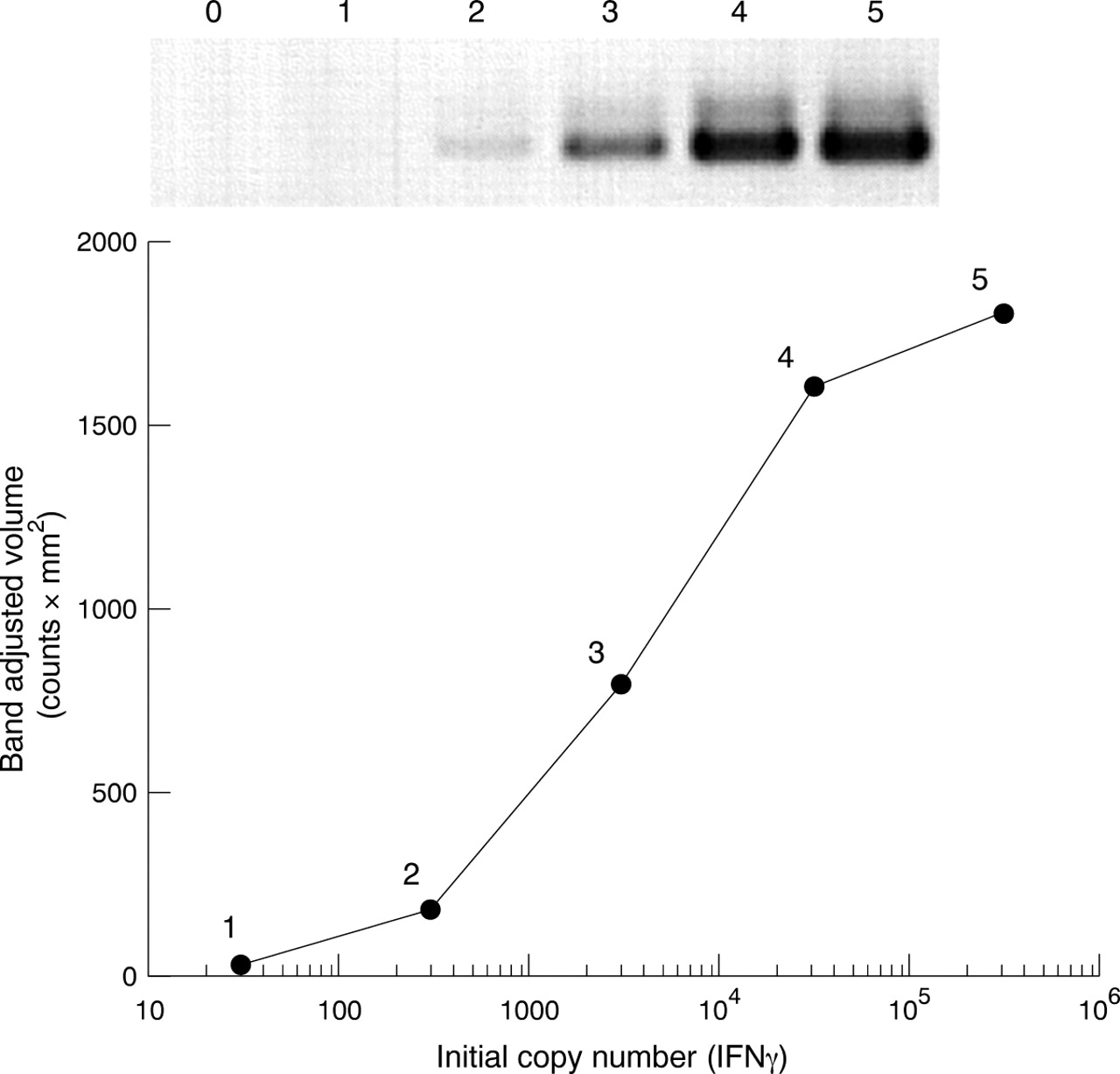
To permit quantitative PCR, analysis data must be collected in the exponential phase of the amplification reaction. To ensure this, standard curves for each cytokine, as well as β2M and CD3, were obtained by plotting the band adjusted volume (counts × mm2) against the log of initial cDNA copy number added to the PCR. Under the optimised PCR conditions, the lower limit of detection was found to be approximately 30 molecules cDNA/reaction. An example of the PCR products obtained from a serial dilution of IFNγ and the corresponding standard curve is shown in figure1.

Amplification of 1:10 serial dilutions of positive control IFNγ cDNA. Lane 0 is negative control. The band adjusted volume (counts × mm2) was plotted against the log number of target cDNA copies.
MEASUREMENT OF CYTOKINES IN SYNOVIAL FLUID
Synovial fluid was frozen at −70ºC until assayed. IL1β, IL6 and TNFα values were each measured with a specific ELISA test (Medgenix Diagnostics, Brussels, Belgium) in accordance with the manufacturer's instructions. In each assay, the appropriate recombinant human cytokine was used to generate the standard curve. Sensitivity of the various assays was: IL1β: 2 pg/ml, IL6: 3 pg/ml and TNFα: 3 pg/ml.
STATISTICAL ANALYSIS
The Mann-Whitney U test was used to determine whether there was a significant difference in the level of expression of each cytokine between patients with RA and SpA. Correlation analysis between different cytokines and other clinical and biological parameters was analysed by the non-parametric Spearman test. The level of statistical significance used was p<0.05.
Results
Four patients (one with RA, two with USpA and one with AS) were excluded from the initial groups because no CD3 mRNA was detected in their synovial samples, although they had β2M mRNA. Table1 details the clinical, biological and demographic data from the 25 patients who were finally analysed. There were no statistical differences between RA and SpA regarding age, disease duration, activity of peripheral arthritis (measured by Thompson's articular index), CRP or number of cells in the synovial fluid.
Demographic, clinical and biological data of the 25 patients finally included in the study
DETECTION AND QUANTIFICATION OF TH1 AND TH2 CYTOKINES MRNA IN SYNOVIUM FROM RA AND SPA PATIENTS
To investigate the T helper profile of lymphocytes present in RA and SpA synovium, the expression of cytokine mRNAs that are useful in defining Th1 (IL2 and IFNγ) and Th2 (IL4, IL5 and IL10) lymphokine patterns were evaluated. By using a sensitive PCR method with a computer assisted analysis, we were able to detect Th1 and Th2 cytokine mRNAs in the synovium of RA and SpA patients. In general, RA synovium showed greater expression of both Th1 and Th2 cytokine genes than that of SpA: Th1 cytokine mRNAs could be detected in all RA synovium samples, but only in 58% (IFNγ, fig 2) and 71% (IL2) of SpA samples. The mRNAs from IL4 and IL5 were also detected in 90% of RA samples against 60% and 40% of SpA samples, respectively. However, IL10 was expressed similarly in RA and SpA synovium (90% of samples).

PCR amplification of the IFNγ mRNA (427-bp fragment) from the synovium of rheumatoid arthritis (RA) and seronegative spondyloarthropathy (SpA) patients included in this study. Lanes: a, RA; b, SpA; +, positive control; −, negative control, without added template DNA.
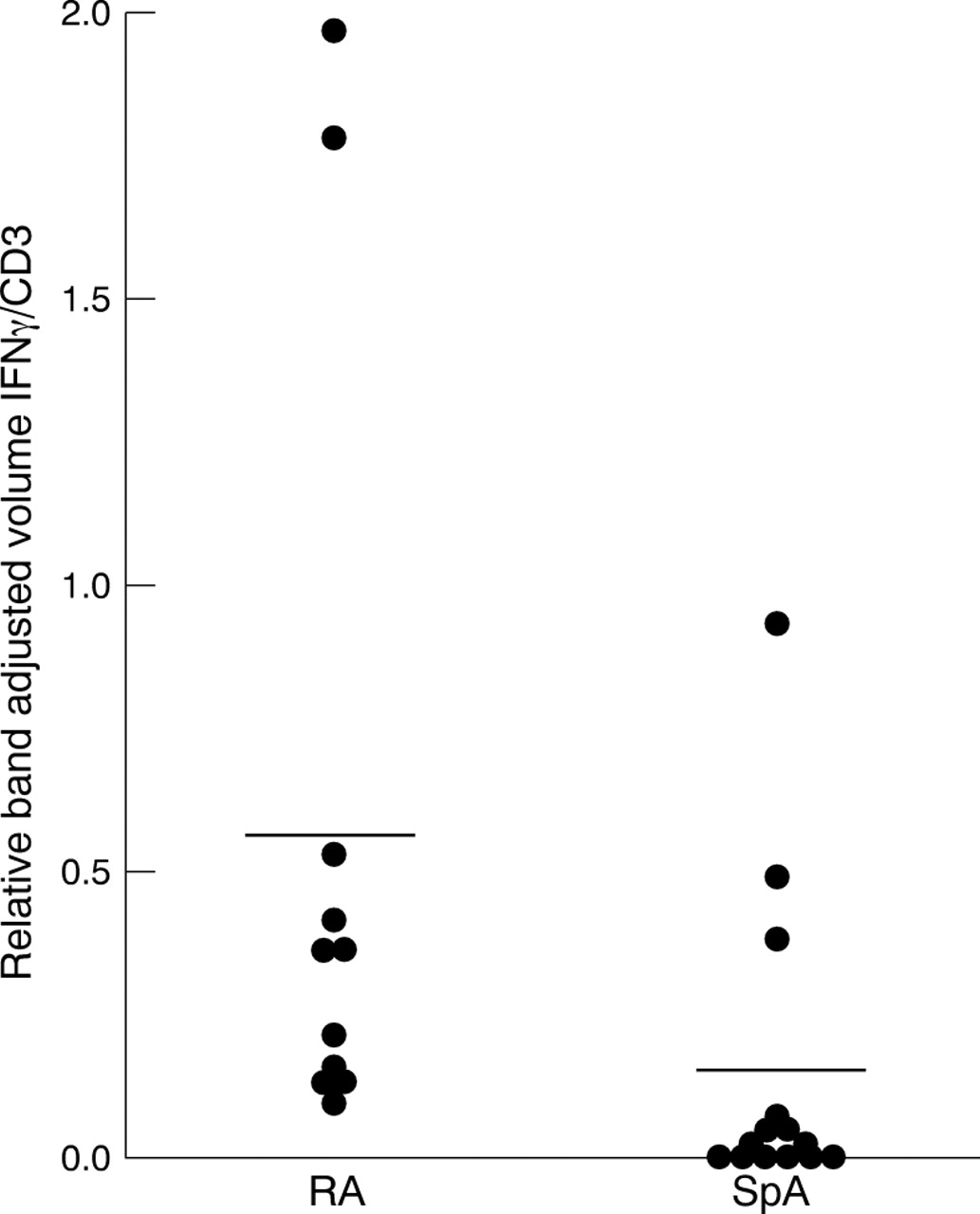
Quantification of Th1/Th2 cytokine mRNA showed that RA synovium expressed statistically significant higher levels of IFNγ, IL2 and IL4 than SpA synovium (table 2). The statistical difference remained when the results were expressed relative to the amount for β2M mRNA. However, when the results were expressed relative to the amount for CD3 mRNA, which is expressed specifically by T cells, only IFNγ levels were higher in RA compared with SpA (p<0.003) (fig 3). This result suggests that the differential expression of IFNγ between RA and SpA synovium could not be attributed to a lower density of T cells in SpA synovium biopsy samples compared with that of RA. Production of detectable Th2 cytokine mRNA in RA synovium was not associated with a reduction of Th1 cytokine mRNA. Although both diseases express a complex pattern of mRNA cytokines in their synovium, the Th1/Th2 (IFNγ/IL4) ratio is fivefold greater in RA than in SpA, thus supporting a predominantly Th1 cytokine pattern in RA in comparison with SpA. No significant differences in the cytokine profile were observed between the different SpA subgroups (data not shown).
T cell cytokine mRNA levels in synovial tissue from rheumatoid arthritis (RA) and seronegative spondyloarthropathy (SpA) patients
{kind=link}
{kind=link}
{kind=link}
IFNγ mRNA expression in the synovium of RA and SpA patients. For each patient the IFNγ/CD3 ratio is plotted. Arithmetic mean values are indicated by horizontal bars.
In synovium from SpA patients, but not in RA patients, the expression of IFNγ correlated with that of IL2 (r=0.85; p< 0.0001), but no other evidence of interdependence between the expression of Th1 or Th2 mRNA was found. No correlation between the synovium cytokine mRNA and clinical and biological data of active disease was observed, except for a positive correlation between IL4 mRNA levels and Thompson's articular index in SpA (r= 0.59; p=0.04).
QUANTIFICATION OF PROINFLAMMATORY CYTOKINES IN SYNOVIAL FLUID
Synovial fluid levels of macrophage derived cytokines, IL1β, TNFα and IL6, were each measured by specific ELISA tests to find differences between RA and SpA, as these cytokines are major mediators of inflammation and joint destruction. IL1β levels were higher in RA than in SpA (p<0.05) (table 3). Moreover, there were also higher levels of TNFα in RA than in SpA, but without statistical significance. Furthermore, in SpA patients, but not in RA patients, a positive correlation was detected between levels of IL6 and TNFα from synovial fluid (r=0.72; p=0.02), and also between IL6 and the number of cells from knee synovial fluid (r=0.72; p=0.02).
Synovial fluid levels of monocyte/macrophage derived cytokines3-150
Discussion
In this study the mRNA profile of T cell derived cytokines expressed in synovium from RA and SpA patients was evaluated by quantitative RT-PCR. In addition, their possible correlation with the protein levels of macrophage derived cytokines in synovial fluid and with clinical and biological data from patients was analysed. Our results show that: (1) in both RA and SpA synovium a complex pattern of T cell derived cytokines is observed, with the two diseases expressing Th1 (IFNγ and IL2) and Th2 (IL4, IL5 and IL10) cytokines; (2) the expression of Th1 and Th2 (except for IL10) cytokine mRNA was more prevalent in RA than in SpA patients; (3) IFNγ mRNA levels were significantly higher in RA than in SpA synovium; (4) the Th1/Th2 (IFNγ/IL4) cytokine mRNA ratio was higher (5:1) in RA than in SpA synovium, supporting a predominantly Th1 pattern of cytokine mRNA expression in RA, but a mixed or Th0-like pattern in SpA; (5) IL4 mRNA levels correlated positively with Thompson's articular index in SpA patients; (6) synovial fluid levels of IL1β were significantly higher in RA than in SpA patients.
The data of this study confirm other studies on Th1/Th2 cytokine expression on RA synovium and extend previous works by investigating USpA patients and by determining IL5 expression. We studied mRNA cytokine expression in synovium because in these diseases the synovial joints display the most marked pathology. The PCR method used in this study has been shown to be sensitive and reproducible.31Moreover, it has previously been demonstrated that, in general, the pattern of cytokine gene expression in synovial tissue paralleled the profile of cytokine release in synovial explant supernatant.32 ,33
The major finding in this study was a marked difference in IFNγ mRNA levels between the two disease groups, with significantly higher levels in RA synovium samples. This was not because of different T cell density between the biopsy specimens analysed as it remained after correcting for the levels of CD3 mRNA, which is specific for T cells. Our results are consistent with previous evidence for a predominance of Th1 cytokine pattern in RA synovium,15-18 ,22 ,34 and with several studies that have also detected the expression of Th2 along with Th1 cytokines in this disease.35 ,36 Moreover, a higher ratio of IFNγ/IL4 positive cells in RA than in ReA has previously been shown using immunohistological techniques.18 ,22 In another study, IFNγ and its receptor were found to be more abundant in RA synovium than in osteoarthritic synovium, and this has been proposed as an evidence for the role of this cytokine in the pathogenesis of rheumatoid inflammation.37 However, a recent study clearly shows the reduced expression of IFNγ by T cells from RA synovium when compared with T cells from tonsils, a chronic T cell mediated immunological reaction. The hyporesponsiveness state of T cells in RA has been widely reported, although it is not observed in all RA patients. Thus, it has been argued that T cell activity waxes and wanes during the course of RA, or that T cell activity plays a dominant part in some subsets of the patient population.19
A similar expression of Th1 and Th2 cytokines was detected in all SpA patients. However, the low levels of IFNγ mRNA in SpA synovium could make the levels of Th2 cytokines more relevant in controlling disease activity, because of the known mutually inhibitory effect between IFNγ and IL4.38 Previous studies on cytokines in SpA synovium have not included USpA patients (the most prevalent group in our SpA patients) and they were basically performed with ReA patients.21 Conflicting results have been reported regarding a predominance of Th1 or Th2 cytokines in ReA.17 ,25 ,39 Two recent works using immunohistological methods showed a lower amount of IFNγ than IL4 expression in ReA synovium.22 ,40 Another study using PCR and immunohistochemistry in PsA synovium detected high levels of IFNγ, IL2 and IL10, but it did not detect IL4. Interestingly, the IFNγ levels were greater in PsA than in RA synovium.33 However, the full clinical classification of PsA patients was not given. Our study included only two PsA patients with axial and peripheral disease and their cytokine profile was similar to that of USpA and AS patients. The low number of patients with PsA excludes a comparison between the two studies. With respect to IL5, which may be implicated in IgA production by B cells in SpA, a preliminary study detected IL5 producing cells in RA synovium35 but a different work only detected gene expression in one out of five samples of PsA synovium.33 Our results do not indicate a differentiated role for IL5 in SpA synovium compared with RA synovium.
An increase in IFNγ over IL4 production may be of pathogenic significance and may account for several of the histomorphological changes in RA, such as activation of monocytes/macrophages and upregulation of HLA class II antigens.15 Therefore, the Th1 pattern, specifically the higher levels of IFNγ in RA synovium, could be responsible for the known progressive and destructive course of this disease, whereas the balanced expression of Th1 and Th2 cytokines in SpA synovium could be related to the frequently observed non-aggressive inflammation in these diseases. Recently, it has been observed that in RA patients, both a decrease in IFNγ and an increase in IL4 production by peripheral T cells correlated with disease activity and severity.41 The same work suggests that these phenomena probably reflect selective Th1 cell migration into the joint, and points to a role for the Th1/Th2 balance in RA pathogenesis.
We have found increased levels of IL10 gene expression in both RA and SpA synovium. Although the synthesis of IL10 is not restricted to Th2 cells, this cytokine has an important immunoregulatory role in arthritis through inhibition of machrophage derived cytokines. Previous studies have detected high levels of IL10 in joints of RA patients, although these levels are insufficient to control the immunoinflammatory response.42 The arthritic joints of ReA patients have characteristically high IL10 and IL4, and low IFNγ levels, and this balance has been related with the persistence of bacteria in the joint.43
Also of interest in our study are the higher levels of proinflammatory cytokines in synovial fluid from patients with RA in comparison with SpA, as IL1β and TNFα are the most important macrophage derived cytokines that contribute to the pathogenesis of RA. The known effect of IFNγ is to activate macrophages, which produces high levels of proinflammatory cytokines.44 In this respect, the higher levels of IFNγ in RA synovium may account for the significantly higher levels of IL1β in synovial fluid from RA patients. The correlation between TNFα, IL6 levels and the number of synovial fluid cells is consistent with our knowledge of the inflammatory cascade, where TNFα induces production of IL6, and both cytokines produce chemoattracting factors, which cause cellular infiltration of the joint space.
Probably because of the sample size, there are no other statistical significant correlations in the RA group. However, in SpA patients the positive correlation between IL4 mRNA levels in synovium and the activity of peripheral synovitis, measured by Thompson's articular index, is remarkable. In this respect it has been demonstrated that IL4 may contribute to the pathogenesis of synovitis by different mechanisms.43 ,45
In conclusion, our study detects significant differences in IFNγ mRNA levels between RA and SpA (mostly USpA patients) synovium, as well as higher IL1β protein levels in RA synovial fluid. Moreover, the IFNγ/IL4 mRNA ratio is significantly higher in the synovial tissue of RA than that of SpA patients. These data confirm previous work on Th1/Th2 cytokine balance in RA and extend the results by comparing RA to SpA subgroups distinct of ReA, predominantly USpA, and probably reflect differences in the pathogenesis of synovitis between RA and SpA, as well as between different subgroups of SpA.
Acknowledgments
The authors are grateful to Dr Salvador Bartolomé, from the Laboratory of Electrophoretic, Fluorescent and Chemiluminescence Data, Department of Biochemistry and Molecular Biology, Universitat Autònoma de Barcelona, for his technical assistance.
References
Footnotes
Funding: this study was supported in part by a grant from DGICYT (Ministerio de Sanidad) Project PM91–0042, and from the Hospital Clínic de Barcelona. Spain.