Article Text

Abstract
OBJECTIVE To find disease parameters that can predict the functional capacity of patients with early rheumatoid arthritis (RA) at the first visit to the rheumatologist and one year after entry.
METHODS Patients referred to the outpatients clinic between 1995 and 1996, with a symptom duration of less than three years and fulfilling the American Rheumatism Association 1987 revised criteria for RA within one year after entry were included. Assessments of the duration of morning stiffness, the Disease Activity Score (DAS: a composite score based on erythrocyte sedimentation rate (ESR), number of painful and swollen joints and patient global assessment), pain (Visual Analogue Scale), the Arthritis Impact Measurement Scale (AIMS) and the Health Assessment Questionnaire (HAQ) were performed every three months. Possible predictors of the HAQ at entry and after one year were analysed by logistic regression.
RESULTS 133 patients were included in the study. The median duration of complaints was three months (range 0–35) and the median HAQ score at entry was 1.12 (range 0–3). There was no correlation between duration of complaints and the HAQ at entry (r = 0.01). An HAQ score under the 50th percentile at entry could be predicted correctly for 74% of the patients by entry DAS and C reactive protein concentration, and at one year could be predicted correctly for 73% of the patients by entry HAQ and pain score.
CONCLUSION Disease activity is strongly correlated with a lower functional capacity at entry, whereas disease duration is not. The functional status at entry is a good predictor for functional status at one year. Severity rather than duration of arthritis prompts referral in this cohort.
- rheumatoid arthritis
- outcome
- functional status
- HAQ
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory joint disease, which leads to functional decline and an increased mortality.1-4 Structural joint damage starts in the first years of disease and may be delayed by adequate treatment at an early stage.5-7 However, RA may be difficult to diagnose at an early stage because of an atypical presentation such as oligoarticular involvement. Furthermore, serological markers such as rheumatoid factor are frequently negative in early RA and radiographs only detect erosions after considerable damage has taken place. In most countries, patients with RA are initially seen by general practitioners who have less experience in diagnosing RA because of the low disease prevalence, subsequently appropriate referral and treatment may be delayed.8-10
It is important to recognise as early as possible the factors that predict a poor outcome in order to treat patients with such characteristics more aggressively than the mild cases. This approach may help to prevent joint damage and preserve functional capacity. This is confirmed by Houssien et al 9who concluded that those patients with delayed specialist referrals have worse physical function outcomes. Several clinical, radiological and laboratory variables have been reported as prognostic factors in patients with early RA: the number of swollen joints, the number of tender joints, functional indices, erosions on radiology, a positive rheumatoid factor test and the presence of the genetic marker HLA-DR4.11 The HAQ12 is a validated instrument for the measurement of functional status that has been widely used in observational studies of and clinical trials in rheumatoid arthritis. According to Eberhardt et al,5 the initial HAQ score is the best predictor of both impairment and disability after two years.
The objective of this study is twofold. Firstly, to test whether the duration of complaints and various disease parameters correlate with the functional status at first visit to the rheumatologist. Secondly, to investigate disease parameters at entry that are predictive for the functional capacity at one year. For this reason, a cohort of early RA patients was followed up during one year in a prospective study.
Methods
PATIENTS
From September 1995 until September 1996, patients with arthritis were followed up prospectively in the Jan van Breemen Institute in Amsterdam, a large outpatient clinic for rheumatology and rehabilitation. Patients newly referred, with symptom duration of less than three years were included in the study if they fulfilled the ACR criteria13 for RA within one year after presentation. All patients gave informed consent. The medical ethical committee approved the study design. Patients who were previously treated elsewhere with a disease modifying anti-rheumatic drug (DMARD) were excluded.
DISEASE PARAMETERS
Outcome was defined as functional capacity and measured by a validated Dutch version of the HAQ.14 The patients were assessed at entry and after 3, 6, 9 and 12 months with an interview, physical examination, HAQ and collection of blood. At entry, demographic characteristics, the time of onset of complaints (persistent pain and swelling), IgM-RF and radiographs of hands and feet were recorded. The presence or absence of radiographic erosions was scored by an experienced radiologist. To assess psychological wellbeing the scales anxiety and depression were used from a validated Dutch version15 of the Arthritis Impact Measurement Scale (AIMS).16 The following parameters were scored every three months: the duration of morning stiffness, C reactive protein (CRP), the 28 joint DAS17: (a composite score based on erythrocyte sedimentation rate (ESR), number of painful and number of swollen joints (both by 28 joint count) and patient global assessment by VAS), physician's global assessment of disease activity (VAS) and pain (VAS).
STATISTICS
Only variables expected to be clinically relevant in relation to functional capacity were used in this study. Variables with a skewed distribution (duration of complaints, serum IgM RF, ESR, morning stiffness, depressive mood and CRP) were log transformed. Pearson correlation was used for the assessment of the correlation between the different variables and the functional capacity (HAQ) at entry and at one year. The patients were dichotomised into two groups, “less disabled” or “more disabled”, using the median of the HAQ score at entry for the first analysis. Variables significantly (p < 0.1) correlated with the HAQ score at entry were dichotomised and subsequently entered into a forward stepwise logistic regression model. For the second analysis, the median of the HAQ score at one year was used to make two groups designating patients as “more disabled” or “less disabled”. Thereafter variables significantly (p < 0.1) correlated with the HAQ score at one year were dichotomised and entered into a forward stepwise logistic regression model. Odds ratios for variables significantly associated with the HAQ score were computed.
Results
One hundred and forty five patients were eligible for the study. Twelve patients were excluded because they moved away at the start (n = 7), had a language problem (n = 3) or refused to participate (n = 2). One hundred and thirty three patients were included in the study of which 111 (83 %) completed the one year follow up (table 1).
Baseline characteristics of 133 patients with early arthritis
The reasons for loss to follow up were death (n= 3: malignancy (n= 2) and renal failure (n= 1)), non-compliance (n=13) and moving home (n= 6). Eight of 13 patients dropping out because of non-compliance were not willing to comply with the protocol although they kept coming to the rheumatologist. The baseline disease characteristics of the 22 patients lost to follow up were similar to those of the 111 completers (data not shown) except for the percentage of IgM-RF positive patients, which was significantly lower in the group of drop outs (45% versus 54%: p = 0.05). The mean ESR in the group of the non-completers at time of drop out (after a mean of three months) was 30 mm 1st h versus 26 in the group of the completers.
PREDICTORS OF FUNCTIONAL STATUS AT ENTRY
The median duration of complaints was three months (range 0–35) and the median HAQ at entry was 1.12 (range 0–3). The relation between the HAQ score and several clinical and laboratory variables at entry was measured by correlation coefficients (table 2, left column). There was no correlation between duration of complaints and HAQ. The HAQ correlated significantly (p < 0.001) with the DAS, pain, physician's global assessment, CRP, morning stiffness and depressive mood. In addition, anxiety (p < 0.01) and serum IgM-RF (p < 0.05) were significantly associated with the HAQ. The logistic regression analysis of possible predictors of functional status at entry is shown in table3. Only two variables, DAS and CRP at entry, independently correlated with HAQ at entry. The DAS score was the most significant one. Patients with a DAS score above the 50th percentile were 2.6 times more likely to be “more disabled” at entry than those with a lower DAS score. The functional status could be predicted with an accuracy of 74% according to the entry DAS score and level of CRP.
Correlation coefficients between HAQ score and clinical and laboratory variables at entry and after one year
Results of logistic regression analysis of entry variables predictive of HAQ score at entry and after one year
PREDICTORS OF FUNCTIONAL STATUS AT ONE YEAR
During the one year follow up 85% of the patients were treated with one or more DMARDS: hydroxychloroquine (13%), sulfasalazine (47%), methotrexate (22%) and auranofin (2%). Furthermore, 77% had received physical therapy and 21% occupational therapy.
The median HAQ score at one year was 0.53 (range 0–2.3). The course of the HAQ and DAS scores over the first year is shown in figure 1. The correlation between the HAQ score at one year and the various predictor variables as measured at entry was less strong than at entry (table 2, right column). The HAQ score at entry had the strongest relation to the HAQ score at one year. The results of the logistic regression analysis of functional status at one year are shown in table 3. Only the variables HAQ and pain at entry contributed significantly to the predictive model of parameters that correlated with HAQ at one year. Patients with a high HAQ score at entry were 2.9 times more likely to belong to the group “more disabled” after one year than those with a low HAQ score. The functional status could be predicted with an accuracy of 73% according to the entry HAQ and pain score.

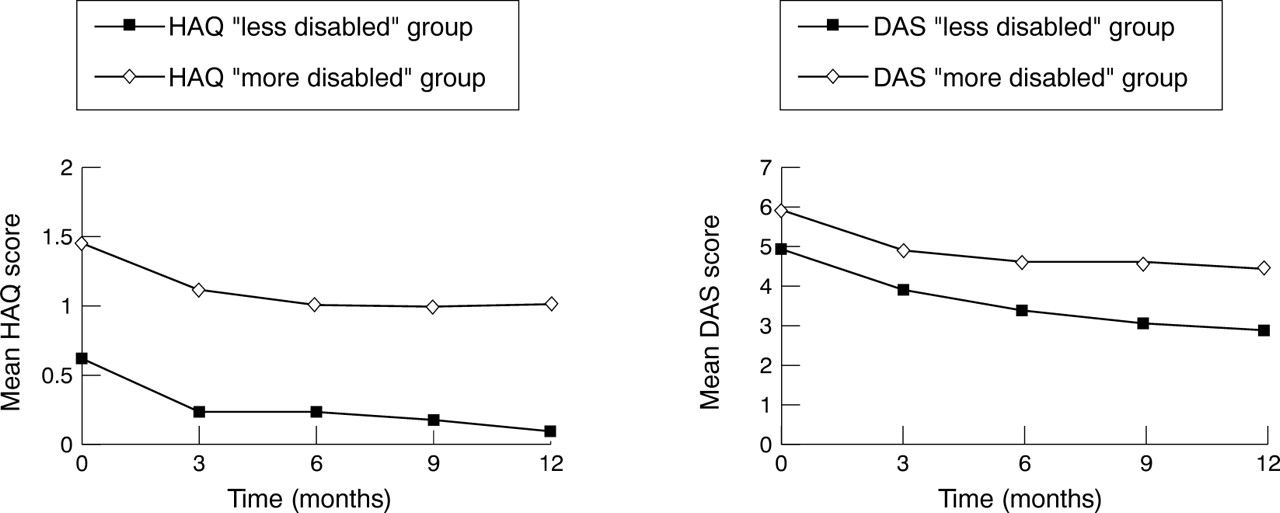{kind=link}
Change of mean HAQ and DAS scores between entry and one year: comparison of the less disabled versus more disabled group partitioned by HAQ 50th percentile at one year.
Discussion
In this group of RA patients with disease duration shorter than three years, the most reliable predictors of functional status at entry are the disease activity parameters DAS score and CRP concentration, whereas the most reliable parameters that predict the functional status after one year are the HAQ and the pain score. The duration of complaints was not related to the functional status at entry or after one year.
The observation that the duration of complaints is not associated with the HAQ score might be because of selective referral. Mild cases may not be immediately referred by the general practitioners, whereas patients with an aggressive onset are presumably sent to the hospital quickly. This is in accordance with Wolfe18 who concluded that patients who are admitted to the hospital in an early stage of their illness usually have more severe disease than those who visit the outpatient clinic later. Furthermore, a selection was made by including only patients with less than three years of complaints in this study. Consequently, the variability in duration of complaints is limited, which may explain the negative result of the possible relation between the HAQ and the duration of complaints. In contrast, Harrisonet al 19 showed that a longer duration of symptoms was related to a decrease in functional capacity. However, their population consisted of patients with RA and undifferentiated inflammatory polyarthritis.
Most of the studies on predictive factors of functional capacity used either the HAQ or Steinbrocker's functional grades as outcome parameter.5 ,11 ,19-21 The HAQ is widely used and consequently this index is included in the ACR 1991 functional status criteria for RA.22 According to Thompsonet al 20 the HAQ performs well and, as a measure of the patients' perspective of disease reflects the true needs of patient care. Although the HAQ is the most frequently reported parameter of function, there are limitations for its use as well.23 According to van den Ende24 sex and disease duration confound the HAQ scores. In this study though, no significant baseline differences in these variables were found between the more or less disabled groups at one year.
In this study, functional outcome could be predicted at one year correctly in 73% of the patients using relatively simple entry measures as pain, HAQ and DAS score. No relation was found between sociodemographic factors and entry HAQ score. This is in contrast with the findings of Vliet Vlieland25 who concluded that a low level of education was correlated to a high number of erosions and a high HAQ score at entry.
Van der Heide et al 26 similarly concluded that disability at one year could be predicted correctly for 79% of the patients by entry HAQ and pain. The majority of studies of early arthritis confirm that initial functional status is the most important predictor of functional capacity at one year or more with an accuracy between 67% and 80%.4 ,5 ,11 ,19 ,26 As the HAQ at entry is the most powerful predictor of the HAQ after one year, other variables that are highly correlated with the HAQ will lose predictive power in the stepwise logistic regression analysis and therefore may not be included in the model. In this study, this is illustrated by the DAS at entry, which shows a strong correlation with the HAQ at one year in the univariate analysis. Therefore, the DAS remains an important predictor of future functional status next to the HAQ.
Several authors confirm the association between CRP, DAS score and HAQ score, but found other significant variables as well.5 ,11 ,19 ,27 ,28 Other factors associated with a high HAQ score are: female sex, a longer disease duration and large joint involvement (at one year)19; patient's global assessment of disease activity, morning stiffness and grip strength (at two years)5 and a positive IgM-RF (at six years).11 After a 12 year follow up age, female sex and radiological progression4 show a correlation with the HAQ.
There seems to be a difference in nature of predictors of functional status between short-term and long term studies. This could explain why in contrast with Sherrer4 and van Zeben,11this study and another26 with shorter term of follow up, the radiological progression and IgM-RF were not found to be predictors of the HAQ score. The disease severity of our patients according to the percentage of patients with a positive rheumatoid factor and erosive disease did not differ much from other studies. The early RA patients of this study are comparable with another study on early RA in the Netherlands according to the number of IgM-rheumatoid factor positive patients.10
In conclusion, the most reliable predictors of functional status at one year were the HAQ score and the level of pain in this group of patients with early RA. Many disease activity parameters correlated significantly with the functional status at entry, whereas disease duration and sociodemographic characteristics did not. Referral seems to be prompted by severity rather than by duration of arthritis. This study demonstrates that the HAQ is highly correlated with the DAS during the first year. Therefore, a goal of treatment is to decrease the DAS as soon as possible to maintain functional capacity.
Acknowledgments
We thank Linda Zandbelt for her large contribution to the organisation of the Early Arthritis Clinic in Amsterdam and the collection of data.