Article Text

Abstract
OBJECTIVES The balance between interferon γ(IFNγ) and interleukin 4 (IL4) producing T cells (T1 and T2 cells) seems to be of importance in many (auto)immune disorders. In general, T1 cell activity is important in cellular immunity whereas T2 cell activity plays a part in humoral responses. T1 cell activity predominates in joints of patients with rheumatoid arthritis (RA) whereas T2 cell activity is characteristic of atopic syndromes. This study investigated whether the prevalence of hay fever in RA is low and if severity of RA (T1 cell activity) can be influenced by the concomitant occurrence of a T2 cell mediated disease (hay fever).
METHODS The prevalence of hay fever was assessed in 643 consecutive (RA and non-RA) patients seen in our outpatient clinic and confirmed by skin test and specific IgE. Of this group the 12 RA patients with hay fever were compared with RA patients without hay fever (matched for age, sex, and disease duration).
RESULTS The prevalence of hay fever in RA patients is lower than in non-RA patients (4% versus 8%), and yields a relative risk for RA patients to develop hay fever of 0.48. RA patients with hay fever showed a lower disease activity (erythrocyte sedimentation rate, C reactive proten, Thompson joint score, and radiographic joint damage (Sharp) score) than RA patients without hay fever. The clinical data were related to peripheral blood T1/T2 cell balance: a lower IFNγ/IL4 ratio was observed for RA patients with hay fever, indicating a comparatively increased T2 cell activity in RA patients with hay fever.
CONCLUSION These results argue in favour of the exploration of treatments aimed at regulation of a possible imbalance in T1/T2 cell activity in RA.
- rheumatoid arthritis
- hay fever
- T1 T cell
- T2 T cell
- interferon γ
- interleukin 4
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a chronic inflammatory disease of unknown aetiology, characterised by destruction of joints. There is evidence that T lymphocytes play a part in chronic joint inflammation in RA.1 2 The balance between two functionally different types of T lymphocyte populations, characterised by their specific cytokine profiles, is reported to be of considerable significance in many human and animal diseases.3 4 Type 1 T cells (T1 cells) participate in delayed type hypersensitivity reactions and cytotoxicity responses and, in addition to other cytokines, specifically produce interferon γ (IFNγ).3 4 In RA intra-articular T1 cell activity has been shown to predominate.5 6 This T1 cell activity stimulates synovial macrophages to produce proinflammatory cytokines such as interleukin 1 (IL1) and tumour necrosis factor α (TNFα), which are important mediators in RA.7 8 Type 2 T cells (T2 cells), in addition to other cytokines, specifically produce interleukin 4 (IL4).3 4 They help B cells to differentiate into specific immunoglobulin producing cells and are involved in eosinophilia. T2 cell activity can inhibit IL1 and TNFα production by macrophages.3 4
In the proper environment specific antigens can direct the differentiation of T lymphocytes into T1 or T2 cells. Bacterial antigens primarily induce development of T1 cells whereas some of the parasitic antigens and allergens facilitate T2 cell development.3 4 Atopic allergy, which is characterised by an increased IgE response and eosinophilia, has been related to T2 cell activity.9-11 Analysis of cytokine production by allergen specific T lymphocytes from atopic donors has shown that the great majority of allergen specific T cells express a T2 cell phenotype, with a high production of IL4 and little or no production of IFNγ.12 13
As T1 and T2 cell activities counterbalance each other, balance of these T cell activities in RA might play an important part in the regulation of proinflammatory cytokines and hence the regulation of joint damage. Human and animal in vitro experiments have shown that T1 cell induced joint inflammation and hence damage of articular cartilage can be inhibited by addition of the T2 cell cytokine IL4.14-17 In this way RA and atopy, when occurring together, might be seen as counterbalancing conditions. Assuming that inflammation and joint damage in RA will increase under conditions of T1 cell predominance, a state of pronounced T2 cell activity (as in hay fever) might influence RA in terms of prevalence or RA disease activity, or both.
The purpose of this study was to investigate whether the prevalence of hay fever, as a major manifestation of the atopic syndrome, is low in a RA population. In addition disease activity and joint damage in RA patients suffering from hay fever were compared with those in RA patients without hay fever. Clinical data were related to peripheral blood T1/T2 cell activity.
Methods
PREVALENCE OF HAY FEVER
We presented a questionnaire to each consecutive patient who visited our rheumatology outpatient clinic during a three month period (from December until February). A total of 643 questionnaires were completed by RA patients (n=304) and non-RA patients (n=339). The diagnosis of the RA patients was based on the 1987 revised ACR criteria.18 The questionnaire included the standard questions on allergy routinely asked by physicians of the department of allergy. A personal history of asthma, allergic rhinitis, hay fever, eczema, and reactions to pets and food were noted and the patients were asked whether first degree relatives had any of these diseases. In all patients who reported via the questionnaire that they had a positive history of hay fever, the diagnosis of hay fever was confirmed by a positive reaction to intra-cutaneously injected inhalation allergens and/or the presence of specific IgE antibodies (confirmed hay fever). The prevalence of hay fever among RA patients was compared with that found for non-RA patients. Statistical analysis was performed by means of the χ2test.
RA HAY FEVER PATIENTS COMPARED WITH RA NON-HAY FEVER PATIENTS
It appeared that in total 12 patients had RA with confirmed hay fever. For these 12 RA patients medication, RA disease activity, joint damage, and T1/T2 cell ratios of peripheral blood mononuclear cells were evaluated. They were compared with the values found for 24 RA patients without hay fever. For every RA patient with hay fever the first two RA patients visiting our outpatient clinic who could be matched for sex, age (within ± 5 year), and disease duration (disease duration ⩽ 5 years: within ± 1 year, disease duration 5–10 years: within ± 2 years, disease duration ⩾ 10 years: within ± 5 years) were selected. These patients were found to have no symptoms of hay fever or asthma. Absence of hay fever was confirmed in this group by a negative test for pollen specific IgE in serum. Parameters of disease activity were assessed for both the RA hay fever and the matched RA non-hay fever group during the hay fever season and afterwards (March–July and September–February, respectively). The Mann-Whitney U test was used for comparison of RA hay fever and RA non-hay fever groups. The Wilcoxon signed rank test was used to compare in season data with out of season data.
Specific and total serum IgE measurement and intra-cutaneous skin test
Specific and total IgE in serum were determined fluorometrically (Pharmacia CAP System) according to instructions of the manufacturer.19 20 Responses toDermatophagoides pteronyssinus, grass pollen, birch, Artemisia vulgaris, A fumigatus, cat and dog dander were assessed. Intra-cutaneous skin tests (ICT) were performed as described previously21 22 using reagents purchased from ALK Benelux bv, Houten, the Netherlands (control, histamine 0.01 mg/ml, mixed grass pollen 30 BU/ml, mixed tree pollen 30 BU/ml,A vulgaris 30 BU/ml, D pteronyssinus 30 BU/ml, mixed fungi 0.05 mg/ml, dog and cat dander 30 BU/ml and latex 1:10).
RA disease activity and joint damage
RA disease activity was assessed by means of the erythrocyte sedimentation rate (ESR Westergren), C reactive protein level (CRP), Thompson joint score (max score 534), and joint damage on radiographs of hands and feet, assessed according to the modified Sharp score (maximum score 448).23 24
Mononuclear cell culture and cytokine determinations
Peripheral blood was diluted 1:1 with Dulbeco’s modified Eagle’s Medium (DMEM). Peripheral blood mononuclear cells (PBMNC) were isolated by density centrifugation using Ficoll-Paque (Pharmacia Biotech, Roosendaal, the Netherlands). Isolated cells were cultured in DMEM, supplemented with PSG (penicillin, streptomycin, and glutamine) and 10% human adult male AB+ serum. Because of undetectable low spontaneous production of IFNγ and IL4, T cells were stimulated aspecifically; 5 × 105 cells per ml were cultured for 48 hours in the presence of anti-CD3 and anti-CD28 antibodies (CLB, Amsterdam, the Netherlands), both diluted 1:1000.25 26 Subsequently culture media were harvested and rendered cell free by centrifugation, frozen in liquid nitrogen, and stored at −20°C. IFNγ and IL4 were determined by ELISA according to the manufacturer’s instructions (Medgenix, Flerus, Belgium). Detection limits of the assays were 5 pg/ml for IFNγ and 10 pg/ml for IL4.
Results
PREVALENCE OF HAY FEVER
Of the 643 patients, 304 had RA according to the 1987 revised ACR criteria. The remaining non-RA group, comprising 339 patients, exhibited a wide range of diagnoses as regularly seen in a rheumatology outpatient clinic (table 1). Of the 339 non-RA patients and 304 RA patients, 102 (30%) and 60 (20%), respectively, reported to have symptoms possibly related to an atopic condition (table 2). From the questionnaires we could identify 38 (11%) non-RA patients with alleged hay fever. The diagnosis hay fever could be confirmed in 28 (8%) of the 339 non-RA patients. The numbers were significantly lower for the RA patient group. In the group of 60 RA patients with a positive history of atopic symptoms we found 13 (4%) RA patients who indicated via the questionnaire that they suffered from hay fever. The diagnosis hay fever could be confirmed in 12 (4%) of the 304 RA patients. The average age of the RA group did not differ from that of the non-RA group, nor was the average age of the hay fever patients in the RA group different from that of the non-RA group. The age distibution in the different groups was normal (skewness range 0.04–0.5). A relative risk for hay fever for the RA group compared with the non-RA group of 0.48 (95% confidence intervals: 0.25, 0.92, p<0.05) was calculated.
Diagnoses of non-RA patients
Prevalence of allergy
RA HAY FEVER PATIENTS COMPARED WITH RA NON-HAY FEVER PATIENTS
Table 3 gives the disease characteristics of the 12 RA patients with confirmed hay fever and the 24 RA non-hay fever patients (recruited as described above). In both groups 67% of patients were rheumatoid factor positive. Extra-articular manifestations were exhibited in none of the RA hay fever patients and in three of the RA non-hay fever patients (pericarditis, pulmonary fibrosis, Raynaud’s phenomenon, rheumatoid pulmonary nodus). Concomitant diseases were seen in two RA hay fever patients (hypertension, primary biliary cirrhosis) and in six RA non-hay fever patients (hypertension, coronary insufficiency, hyperthyroidism, hypothyroidism, prolactinoma). Separation according to ARA functional class (1–4)18 did not yield significant differences between the two groups. Total IgE and total eosinophilic count were significantly higher in the RA hay fever group (p<0.05 and p<0.005, respectively).
Patient characteristics
In the RA hay fever group 33% of the patients were taking methotrexate (maximum dose 12.5 mg weekly), 17% taking salazopyrine (maximum dose 2 g daily), 17% taking auromyosis, and 8% taking hydroxychloroquine. In the RA non-hay fever group single disease modifying anti-rheumatic drugs (DMARDs) were comparable; methotrexate 29% (maximum dose 15 mg weekly), sulphasalazine 21% (maximum dose 3 g daily), auromyosis 8%, hydroxychloroquine 8%, azathioprine 4%. However, combination therapy, not prescribed for the RA hay fever group, was administered to 21% of the RA non-hay fever group; methotrexate combined with hydroxychloroquine (17%) and sulphasalazine with hydroxychloroquine (4%). A significantly lower percentage of the RA non-hay fever patients received no DMARD medication (8% v 25%, p<0.05). None of the patients used prednisone. None of the 12 RA hay fever patients took anti-histaminic drugs outside the hay fever season. During the hay fever season seven patients took oral anti-histaminic drugs, one anti-histaminic nosespray, one occasionally used a beclomethasone nosespray (but not during the study), and three patients did not take any anti-allergic drug. Previous use of DMARDs was recorded for both groups but no differences were found. Previous use of corticosteroids (not shown) was 21% for the RA non-hay fever group compared with none of the RA hay fever patients (p<0.05).
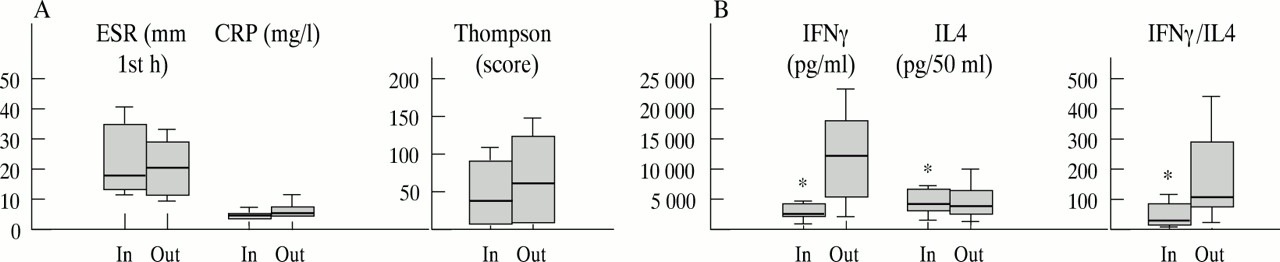
Figure 1A shows the severity of the RA (ESR, CRP, Thompson joint score, and modified Sharp score) during the hay fever season (March–July) for both RA hay fever and RA non-hay fever patients. In the RA hay fever group ESR and CRP were significantly lower compared with the RA non-hay fever group (p<0.05 and p<0.001 respectively). Thompson joint score and Sharp score were lower in the RA hay fever group but did not reach statistical significance (p<0.06). Figure 1B shows the PBMNC cytokine profiles for the RA hay fever patients and RA non-hay fever patients during the hay fever season. IFNγ levels were significantly lower for RA hay fever patients compared with RA non-hay fever patients (p<0.01). IL4 was slightly higher, although not statistically significant, in the RA hay fever group. The average IFNγ/IL4 ratio determined for every person was significantly lower in the RA hay fever group compared with the RA non-hay fever group (p<0.04).

(A) ESR, CRP, Thompson joint score, and modified Sharp score of RA non-hay fever patients (C; n=24) and RA hay fever patients (HF; n=12,), studied during the hay fever season. Boxplots represent: median (thick line), 25–75% (box), 10–90% (thin line). Asterisks indicate a statistical significant difference between the two groups (p< 0.05). (B) Characteristic T1 and T2 cell cytokines IFNγ and IL4, respectively (left axis) and their ratio (right axis) produced by mitogenic stimulated PB-MNC of 24 RA non-hay fever patients (C) and 12 RA hay fever patients (HF) during the hay fever season. Boxplots represent: median (thick line), 25–75% (box), 10–90% (thin line). Asterisks indicate a statistical significant difference between the two groups (p< 0.05).
To evaluate whether the cytokine profile and disease activity are influenced by a change in season, the 12 RA hay fever patients and 24 RA non-hay fever patients were studied both during the pollen season and during the rest of the year. Radiographic joint damage is not expected to change within a year and was therefore not included in this part of the study. In season cytokine profiles for the RA non-hay fever group and parameters of RA disease activity did not differ from those obtained during the rest of the year (data not shown). Cytokine profiles of RA hay fever patients on the other hand were influenced significantly by seasonal changes (fig 2B). For the RA hay fever group the IFNγ level was significantly lower during the hay fever season than the rest of the year (p<0.003). The average IL4 level was significantly higher during the hay fever season than the rest of the year (p<0.03). As may be expected, the IFNγ/IL4 ratio during the hay fever season differed significantly from the ratio found for the rest of the year (p<0.002). Surprisingly, RA patients suffering from hay fever exhibited no significant differences in RA disease parameters with respect to the hay fever season (fig 2A).
{kind=link}
{kind=link}
(A) ESR, CRP, Thompson joint score, and modified Sharp score of RA hay fever patients (n=12), studied during (in) and after the hay fever season (out). Boxplots represent: median (thick line), 25–75% (box), 10–90% (thin line). (B) Characteristic T1 and T2 cell cytokines IFNγ and IL4, respectively (left axis) and their ratio (right axis) produced by mitogenic stimulated PBMNC of 12 RA hay fever patients, studied during (in) and after the hay fever season (out). Boxplots represent: median (thick line), 25–75% (box), 10–90% (thin line). Asterisks indicate a statistical significant difference between the two groups (p< 0.05).
Discussion
The balance between T1 and T2 cell activity seems crucial in controlling immune responses.3 4 In several immune disorders a skewing towards either T1 or T2 cell predominance in the chronic phase of the disease has been shown. Chronic RA has been suggested to be T1 cell predominated,5 6 whereas atopic diseases, such as hay fever, are T2 cell directed.9-13 Because in many disorders T1 and T2 cell activities counterbalance one another, we hypothesised that a T1 cell related disorder might in part exclude a T2 cell related disorder. This might be reflected in a low prevalence of a T2 cell mediated disease in a population of patients suffering from a T1 cell dominated disease or vice versa. Moreover, suppression of activity of the T1 or T2 cell mediated disease might occur in the presence of the counterbalancing disease.
In this study we assessed the prevalence of hay fever in a RA population and studied the severity of RA when hay fever was evident. Hay fever, in contrast with eczema or asthma, was chosen because it can be diagnosed reliably by means of a questionnaire because of its typical signs and symptoms that affect the conjunctiva, nasal mucosa, and respiratory tract and its occurrence during typical seasons. A significantly lower prevalence of hay fever (4%) among RA patients compared with a group of non-RA patients (8%) was observed. These findings could not be attributed to an age difference between the two groups. The prevalence of hay fever in the non-RA patient group corresponds to the prevalence of hay fever in the general population, reported to be 8% to 14%.27 28 The decreased prevalence of hay fever in RA is corroborated by data from the O’Driscoll group in 1985.29 They showed that the prevalence of allergic rhinitis in 40 RA patients and 40 age and sex matched controls was 8% and 15%, respectively. The difference was not statistically significant because of the comparatively small groups so that no definitive conclusion could be drawn from their study. On the other hand, in another T1 cell mediated chronic immune disorder, multiple sclerosis, the prevalence of IgE mediated allergy has been reported to be low (4%) as well.30 A recent study on Japanese children with positive delayed type hypersensitivity reaction to mycobacterium tuberculosis showed serum cytokine profiles suggestive of a predominant T1 cell response which correlated with a lower incidence of asthma.31 These results suggest that not only RA and multiple sclerosis but the presence of a T1 cell dominated disease in general (more or less) excludes a T2 cell mediated disease such as an atopic disorder. Although no definitive data are available as yet, it could be speculated that T1 and T2 cell related diseases mutually exclude one another, including protection against development of a T1 cell mediated disease when a T2 cell dominated disease is present.
It seemed that not only the prevalence of hay fever is low in RA patients but also that RA is less severe when hay fever is evident. Parameters of disease activity (ESR, CRP, Thompson joint score) were all significantly lower in the RA hay fever group compared with the RA non-hay fever group. This was also reflected by the use of DMARDs in the two groups (although not statistically significant); for example, combination DMARD medication was used more often by the RA non-hay fever group. Radiographic joint damage (modified Sharp score) was also lower in the RA hay fever group compared with the RA non-hay fever group. The latter may be the result of longstanding lower disease activity in RA hay fever patients. This suggests suppression of a T1 cell dominated immune disease by a T2 cell mediated immune disorder, which is supported by the observed differences in ratio of T1/T2 cell activity. RA hay fever patients produce significantly lower IFNγ levels compared with RA patients without hay fever. No difference in IL4 levels was seen, but it is significant that the IFNγ/IL4 ratio was lower in the RA hay fever group. That RA hay fever patients do not exhibit a significantly increased IL4 production compared with RA non-hay fever patients may be attributed to the pronounced T1 cell dominance in RA. Seasonal changes, however, clearly showed a relation between hay fever and T2 cell activity (increased IL4 production in the hay fever season). Surprisingly, seasonal changes, reflected by changes in the T1/T2 balance, did not coincide with further suppression of disease activity in these RA hay fever patients. ESR, CRP, and Thompson joint scores did not differ significantly during and after the hay fever season. Although many RA hay fever patients used anti-histaminic drugs during the hay fever season, it is unlikely that the observed change in T1/T2 balance was caused by these drugs. Apart from corticosteroids it is not known to our knowledge that other DMARDs suppress symptoms of hay fever. As the questionnaire reflects lifetime history of hay fever rather than current hay fever symptoms it is not likely that a bias has been introduced. Moreover, the within RA group patients comparison seems to refute such a bias. It is more probable that a longstanding atopic constitution with seasonal T2 cell dominance is needed to suppress RA disease parameters. Allergen specific seasonal T2 cell activity may suppress (the generation of) T1 cell activity in the peripheral blood, which may lead to longlasting suppression of local intra-articular (induced) T1 cell activity, which in turn leads to suppression of RA clinical outcome parameters.
This study shows that in the clinical setting of a T1 cell mediated disease such as RA, T2 cell activity may be regulatory. Thus it would be worthwhile to evaluate means by which T cells can be directed towards a T2 cell phenotype to control the inflammatory process in a T1 cell mediated disease such as chronic invalidating RA.
Acknowledgments
We thank the physicians involved in the care of participating patients: Dr JWG Jacobs, Dr AA Kruize, Dr AAM Blaauw, CA Goldhoorn, Dr MJ van der Veen, DM Hofman, RM van Vugt. This work was supported by “Het Nationaal Reumafonds” (Dutch League against Rheumatism), the Netherlands.