Article Text

Abstract
OBJECTIVES To establish the risk of falling among those who consult their general practitioner with a new episode of hip pain and to discover if risk is altered by age and according to whether, at presentation, signs of osteoarthritis are present on radiography.
METHODS A case-control study was conducted. Cases were all patients who presented with a new episode of hip pain to participating general practices throughout the United Kingdom. All cases had a pelvic radiograph taken on recruitment to the study. Three controls were matched for sex, age, and general practice to each case. A questionnaire was sent by post to all cases and controls. The risk of having fallen in the past 12 months among cases and controls was compared.
RESULTS The study included 111 cases presenting with hip pain and 229 controls who had not consulted with hip pain in the previous 12 months. Women (odds ratio = 3.6, 95% CI 1.9, 6.7) but not men (odds ratio = 0.8, 95% CI 0.3, 2.3) reported an increased risk of falling in the previous 12 months. Similar results were obtained when the previous four months were considered. For all cases, hip pain predated any reported falls. The increased risk in women was found particularly for those aged less than 70. Risk of falling was not altered by the presence of radiological changes of osteoarthritis.
CONCLUSIONS Hip pain, which may be a symptom of osteoarthritis of the hip, increases the risk of falling. This finding has implications for the advice offered by general practitioners to patients who consult with early hip pain.
- falls
- hip osteoarthritis
- general practice
Statistics from Altmetric.com
Falls are a significant cause of morbidity and mortality among the elderly. Campbell1 discovered a high rate of falling among over 70 year olds: 40% of women experienced at least one fall during the study year, compared with 28% of men. Women who fell were more likely to have a limited range of hip movement (an objective indication of osteoarthritis of the hip), while those with a history of hip pain (a subjective indication of hip osteoarthritis) were no more likely to fall compared with those with no such history.
Osteoarthritis of the hip is comparatively common among the elderly. It is estimated that 5% of 65 year olds have symptomatic osteoarthritis of the hip.2 Jones et al 3 found that although subjects with osteoarthritis had higher bone density, those who fell were not protected against osteoporotic fracture.
Falling may be an important risk factor in determining the outcome of early hip osteoarthritis. This study aims to establish whether there is a higher occurrence of falls among those who consult their general practitioner with a new episode of hip pain, the risk of falling by age, and whether risk is altered by signs of osteoarthritis on radiography.
Methods
PATIENTS
A network of 60 general practitioner members of the Primary Care Rheumatology Society throughout the United Kingdom agreed to recruit cases and controls for the study. Patients were eligible for inclusion as cases if all of the following criteria were satisfied: the patient consulted with an episode of hip pain believed to be musculoskeletal in origin between November 1994 and November 1995 (although not all practices recruited for the full study year), no consultation for hip pain had taken place within the previous 12 months, the pain arose from within the area shown in figure 1, and the painful hip had not previously been replaced. On recruitment to the study, a pelvic radiography was taken.

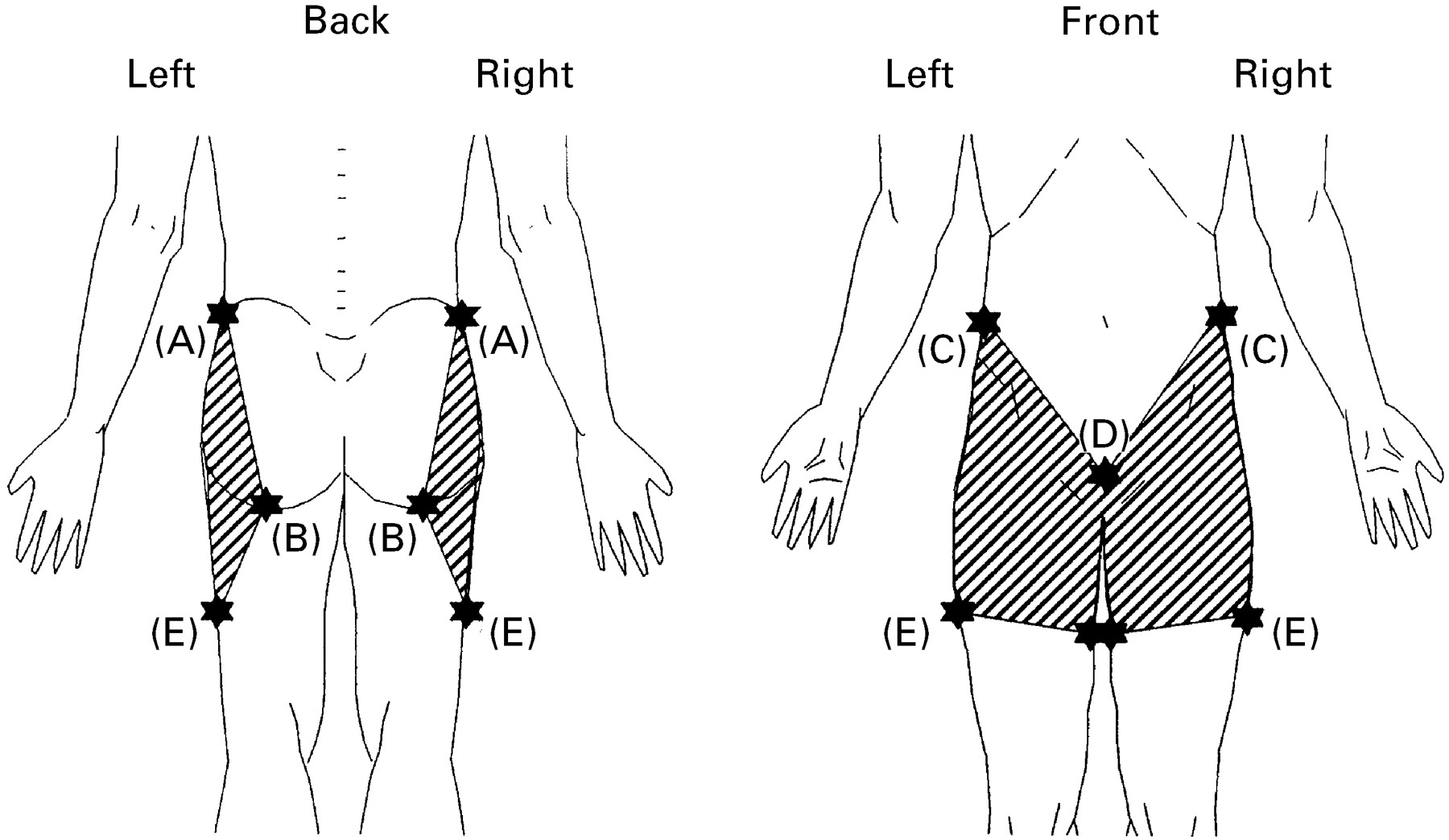{kind=link}
Musculoskeletal pain in the shaded area. A: Iliac crest, B: ischial tuberosity, C: anterior superior iliac spine, D: pubic tubercle, E: point one third down thigh.
The general practitioner selected the next three patients on the age-sex register of the practice who were of the same sex and had the same year of birth as the case. These patients formed the control group.
DATA COLLECTION
A questionnaire was sent by post to all cases and controls. For those failing to respond, up to two written reminder letters were sent after two and four weeks. The questionnaire, previously used in a study by O’Neill et al 4 made specific inquiry about falls in the previous 12 months and the previous four months. If subjects had fallen within the previous four months, details (location, time, and circumstances) of their most recent fall were requested. An additional screening question was included in the questionnaire for controls to identify those who had consulted their general practitioner with hip pain during the previous 12 months.
STATISTICAL ANALYSIS
Analysis, as a case-control study, has been conducted using the statistical package STATA.5 The results of the analysis are presented as odds ratios with 95% confidence intervals. Given that similar results were obtained from a matched and unmatched analyses, the results reported are from an unmatched analysis.
Results
A response rate of 97% was obtained among cases (111 completed questionnaires from 115 eligible subjects) and 73% among controls (251 completed questionnaires from 345 eligible subjects). Twenty two controls (4 men, 18 women) had consulted their general practitioner with hip pain during the previous 12 months and were excluded from further analysis. All cases had suffered hip pain before their reported fall.
Thirty six of 111 cases (32%) were male with a median age of 69 (interquartile range (IQR) 59–74); female cases were slightly younger (median age = 66, IQR 56–72). As controls were matched for age and sex, the sex distribution among controls is very similar to that of cases, although a particularly high response rate in the controls aged 70+ years has led to a slightly higher percentage of controls (40%) compared with cases (37%) in this age group.
Among women the odds of having fallen in the last 12 months were increased threefold in those who had consulted their GP with hip pain (odds ratio (OR) =3.6, 95% confidence intervals (CI) (1.9, 6.7)). Of women consulting with hip pain 41% reported having fallen in comparison with 16% of controls. In contrast among men the risk of falling did not differ between those with and without hip pain (OR=0.8, 95%CI (0.3, 2.3)); 19% of male cases fell compared with 22% of controls. All persons with hip pain who reported having fallen, indicated that the hip pain predated the reported fall.
Pelvic radiography for 105 of the 111 cases were available. These have been blindly assessed and graded using a modified version of the classification originally proposed by Kellgren and Lawrence.6 When the above analysis was stratified according to whether changes consistent with osteoarthritis were present on radiography the excess risk of falling among women is evident in both groups. Among those with radiological changes the odds of falling were more than double that of controls (OR = 2.8, 95%CI (1.3, 6.0)) but an even higher risk was observed in those without radiological changes (OR = 5.5, 95%CI (2.4, 13). In men the risk of falling, among those with radiographic osteoarthritis was increased but not significant (OR = 1.7, 95%CI (0.6, 5.0)).
The risk of falling has been further analysed, separately for men and women, by age group (table 1). For women, the excess risk of falling among those with hip pain is confined to the age groups less than 60 years and 60–69 years. In the oldest age group (70 years and over) the risk of falling was similar irrespective of whether hip pain was present. Among men, there was no significantly increased risk of falling among those with hip pain, although the risk at ages less than 60 was increased (non-significant).
Odds of falling in past 12 months by age group according to hip pain status
The frequency of falling increased with age among control patients: in men from 10% at age less than 60 to 32% at ages 70 or over, and in women from 15% to 25%. In contrast among cases the frequency of falling did not increase with age, the highest fall rates being in the under 60 years age group for both men (27%) and women (50%).
Further information, on the circumstances and type of fall, was available on falls that had taken place within the previous four months. Men with hip pain were more likely to report a fall with their hand hitting the ground first (OR=5.6, 95%CI (1.2, 26)) compared with men without hip pain, while women with hip pain more commonly reported hitting the ground with their hip (OR=8.8, 95%CI (1.4, 56)). There was no increased risk for men with hip pain having a fall resulting in some injury but women with hip pain were twice as likely to have such a fall (OR=2.4, 95%CI (1.0, 5.9)).
Among male controls all falls occurred outdoors, while one third of those with hip pain fell indoors. Falls occurred outdoors and indoors to the same extent in female cases and controls, but those with hip pain were more likely to fall between noon and 6 pm (10 of 21 falls) in comparison with those without hip pain (1 of 18 falls) (OR=24, 95%CI (5.5, 104)).
None of the female and only one of the male controls blamed hip pain as the reason for falling while 40% of the male cases (2 of 5) and 25% of the female cases (5 of 20) gave this as the reason. Cases often attributed their fall to their leg “giving way” or “locking” (67% men, 38% women).
Discussion
We aimed to discover whether patients who consult with early symptomatic hip osteoarthritis are more likely to fall compared with the general population. Women under 70 years old who consulted with hip pain were more likely to fall, with the increased risk of falling observed both in the presence and absence of radiological changes indicating hip osteoarthritis.
The participation rate among cases was excellent and among controls satisfactory, and the control participants did not differ from all potential controls in terms of age and sex. Furthermore, the rates of falling reported in the control population were similar to those found in other studies: 32% of male controls aged 70 or over had fallen in the past 12 months compared with 25% of female controls. Campbellet al 1 found this same rate of falling among men but a higher rate among women, while Gryfe7 found similar rates of falling among men and women. We can therefore conclude that response bias did not lead to an underestimation of falls. The data were collected retrospectively and therefore are prone to recall bias. For example, those having consulted the GP with hip pain may be more likely to recall falls than those without hip pain. This seems unlikely, however, because firstly falls are likely to be a memorable event for subjects and secondly associations between hip pain and falls were only evident in specific age-sex groups. Nevertheless, it would be important to confirm such a result in a prospective study of subjects with hip pain, and not confined solely to those who have consulted.
We believe therefore that the main finding of women aged under 70 with hip pain being more prone to falling can be extrapolated to the general population. Considering that women are more likely to fall on the hip and are more likely to have a fall that results in an injury, this may aggravate any potential hip osteoarthritis and reduce range of movement. General practitioners would be advised to inform women under 70 who consult with hip pain that they may be more prone to falling and therefore should take premature action such as removing potential obstacles.
Acknowledgments
The authors thank Arthritis Care for funding this study, the general practitioner members of the Primary Care Rheumatology Society who recruited patients to participate in this study and supplied details of the controls, the subjects who completed the questionnaires, Elaine Thomas who advised and assisted with the statistical analysis, Daniel Pope for graphics work, and Lesley Jordan for preparation of the manuscript.