Article Text

Abstract
OBJECTIVE To demonstrate the diagnostic efficacy of ultrasonography in depicting erosions in patients with rheumatoid arthritis and to compare sonographic and radiographic findings.
METHODS Sonographic images were obtained with an AU-4 Idea Esaote Biomedica (Genoa, Italy) equipped with a 13 MHz linear transducer.
RESULTS The images reported in this essay are representative examples of the ability of ultrasonography to detect and characterise even minimal bone margin changes in rheumatoid arthritis.
CONCLUSION Ultrasonography with very high frequency transducers can depict bone erosions in early target areas of bone resorption. However, further studies are needed to validate this technique and to evaluate the relation between sonographic findings and those obtained with other imaging techniques (standard radiology, magnetic resonance).
- ultrasonography
- rheumatoid arthritis
- bone erosions
- small joints
Statistics from Altmetric.com
Ultrasonography is a highly sensitive tool for the identification of fine soft tissue changes. It is increasingly used in rheumatological practice, especially to assess tendon and joint involvement.1-6 Based on the high resolution performance of the last generation linear transducers, it can be suggested that ultrasonography might also be used as an adjunctive imaging tool in early detection of bone erosions in patients with recent onset rheumatoid arthritis (RA). Initial reports suggested that ultrasonography appears to be a promising technique for detecting bone erosions.7-11 The aims of this pictorial essay were to demonstrate the diagnostic efficacy of ultrasonography in depicting erosions in patients with RA and to compare sonographic and radiographic findings of the early target of the erosive process in RA.
Methods
Sonographic images were obtained with an AU-4 Idea Esaote Biomedica (Genoa, Italy) equipped with a 13 MHz linear transducer.
The sonograms of this study were taken in six representative patients with RA, fulfilling the American College of Rheumatology (formerly, the American Rheumatism Association) criteria, and three healthy subjects who had no history or signs of hand disease.12 Sonographic assessment was performed at the second metacarpophalangeal (MCP) joint and the fifth metatarsophalangeal (MTP) joint, which are among the anatomical areas affected earliest in the erosive process.13 ,14 All joints were studied by the following standard scans: longitudinal dorsal scan, longitudinal lateral scan, longitudinal volar scan, transverse dorsal scan, transverse lateral scan, and transverse volar scan. Moreover, both on longitudinal and transverse scans, the probe was moved over the joint to allow a careful assessment of the examined area (multiplanar dynamic assessment). Multiplanar sonographic scans were compared with standardx ray pictures of the selected areas.
Results
Figure 1 shows the standard sonographic appearance of the second MCP joint and of the fifth MTP joint, obtained with a 13 MHz linear transducer on the main scanning planes (dorsal longitudinal and transverse views).

Healthy subject. Metacarpophalangeal joint of the second finger: longitudinal (A) and transverse (B) dorsal scans. Metatarsophalangeal joint of the fifth toe: longitudinal (C) and transverse (D) dorsal scans. Articular cartilage appears as a clearly defined anechoic band delimited by sharp hyperechoic borders corresponding to the bone margin (arrowhead) and to the cartilage soft tissue interface (white triangle). mc = metacarpal head; mt = metatarsal head; ph = phalanx.
The second MCP joint was also explored on a longitudinal dorsal scan with the finger in maximal active flexion. The bone margin is clearly detectable in healthy subjects as a sharp, homogeneous, and hyperechoic band with a posterior acoustic shadow. Bone erosion appears as an interruption of the bone margin (fig 2).

Rheumatoid arthritis. Longitudinal dorsal scans. Sonographic features of bone erosions of the metacarpal head. (A and B) Early disease. (C and D) Late disease. * = erosion; mc = metacarpal head; ph = phalanx.
Multiplanar capabilities of ultrasonography allow a careful assessment of the bone surfaces on more views than those allowed by standardx ray. This improves the sensitivity of the ultrasonography in detecting small erosions in areas unexplored by standard views. Figure 3 shows the diagnostic efficacy of multiplanar sonographic assessment of the second MCP joint. The radial view (fig 4) is very useful in depicting bone changes of the metacarpal head, which is a typical early target of the erosive process in RA.

Rheumatoid arthritis. Longitudinal dorsal views at different scanning planes as indicated on the corresponding standard radiogram (A). (B) Longitudinal dorsal scan shows a still well defined bone margin of the metacarpal head. (C) Longitudinal dorsal scan on a contiguous plane shows a clearly evident erosion (*). (D) Radial scan of the joint showing a large area of bone resorption (*). mc = metacarpal head; ph = phalanx.

Rheumatoid arthritis. Metacarpophalangeal joint of the second finger (same patient as fig 3). (A) Coronal scan. (B) Healthy subject. The coronal view demonstrates the good correspondence between radiographic (C) and sonographic (D) changes of the bone margin. * = erosion; mc = metacarpal head; ph = phalanx.
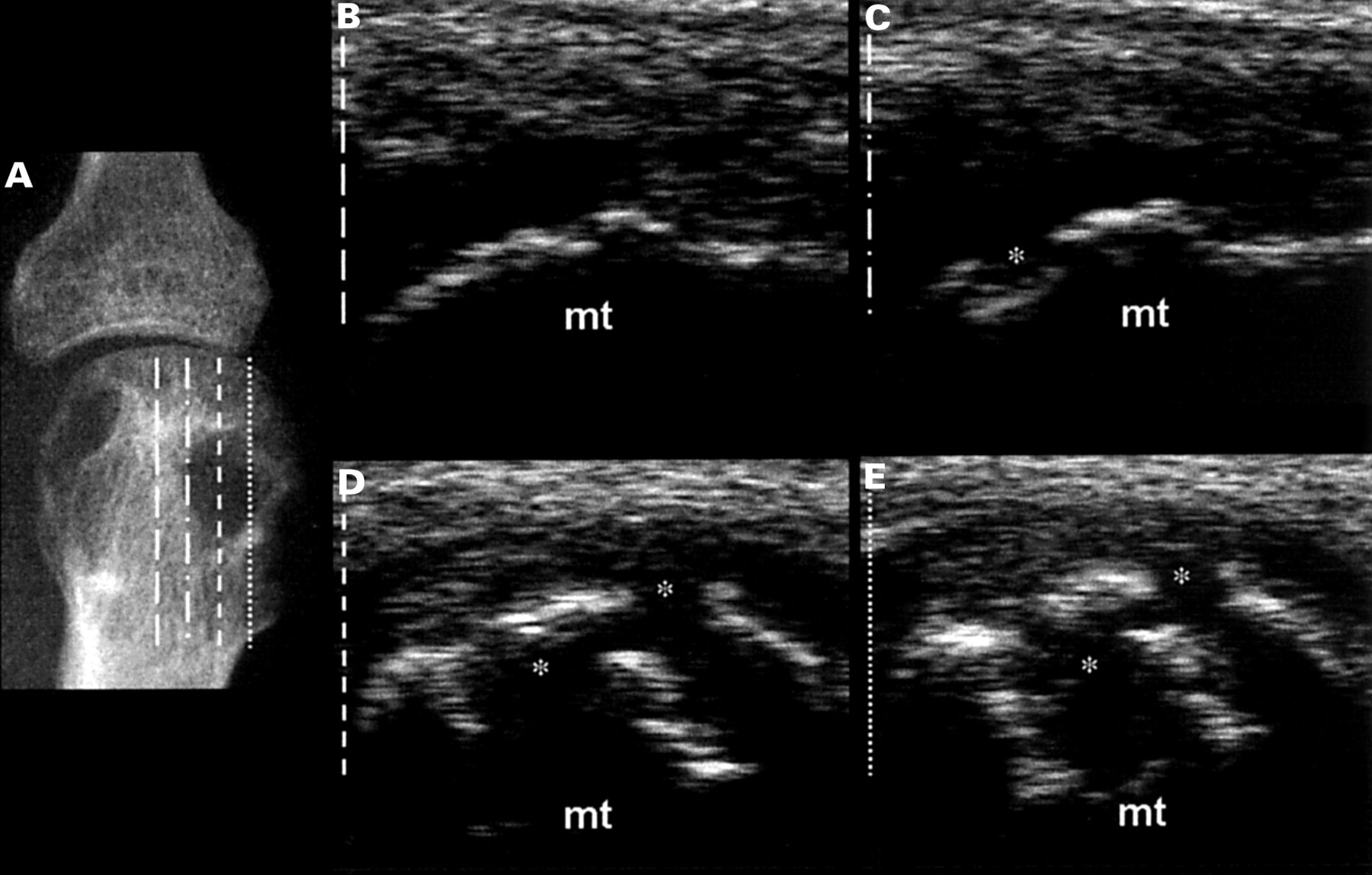
The fifth MTP joint is another key target of early RA. Initial erosions of the fifth MTP joints are among the earliest indicators of an erosive process but they can be frequently missed especially in patients with low quality radiographic documentation. Figure 5 shows a typical example of an x ray of the fifth MTP joint of uncertain interpretation (a Sharp's score of 1 is probably the most appropriate). Sonographic examination does not show any features indicating an erosive process on the standard longitudinal dorsal view. Conversely, lateral scan shows an interruption of the cortex of the metatarsal head with two clearly evident erosions. A reassessment of the x ray performed after an off line digitalisation of the standard radiogram and a subsequent image enhancement and analysis showed that two areas of low bone density could correspond to the erosions depicted by ultrasonography on a coronal plane (fig 5).

Rheumatoid arthritis. Metatarsal head of the fifth toe. Standard x ray (A) does not reveal clearly evident erosive changes (Sharp's score =1). (B and C) Off line digitalised radiograms show two areas of lower bone density (*) and loss of the normal sharp bone margin of the metatarsal head. (D) Longitudinal dorsal scan of metatarsal head does not reveal bone margin changes. (E) Coronal scan discloses clearly evident erosions of the metatarsal head, probably corresponding to the areas of low bone density on x ray. mt = metatarsal head.
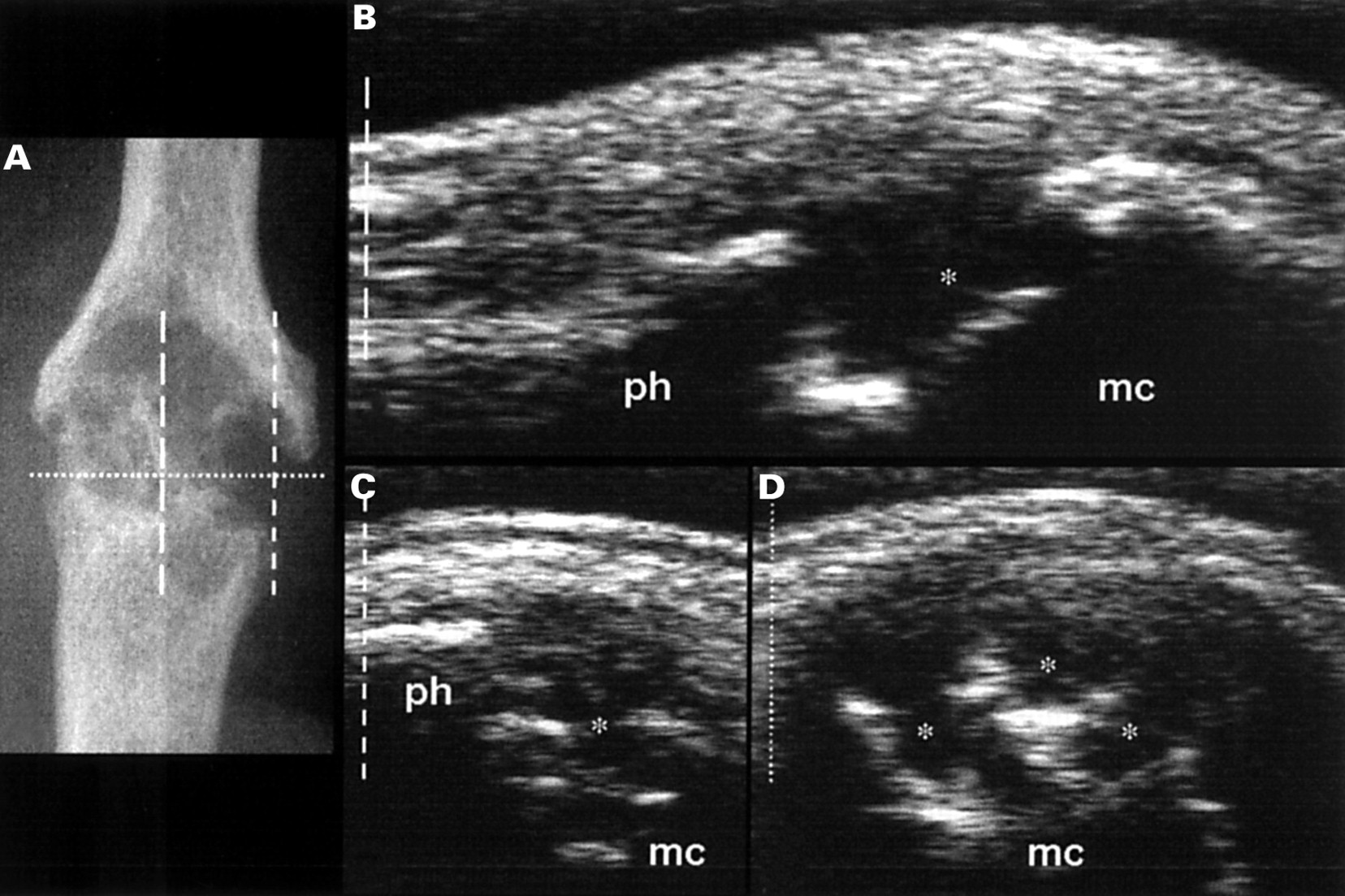
Figure 6 shows the different sonographic views that can be obtained by examining the fifth MTP joint on different planes. Figure 7 is a representative example of the sonographic appearance of severe erosive changes. In patients with advanced joint damage, ultrasonography clearly depicts areas of extensive bone resorption (fig 8). The extension of the erosive changes can be documented both on longitudinal and transverse scans.
Rheumatoid arthritis. Metatarsophalangeal joint of the fifth toe. Sonographic features of the metatarsal head at different scanning planes. These pictures demonstrate the potential role of multiplanar sonographic examination in detecting bone erosion (*). mt = metatarsal head.
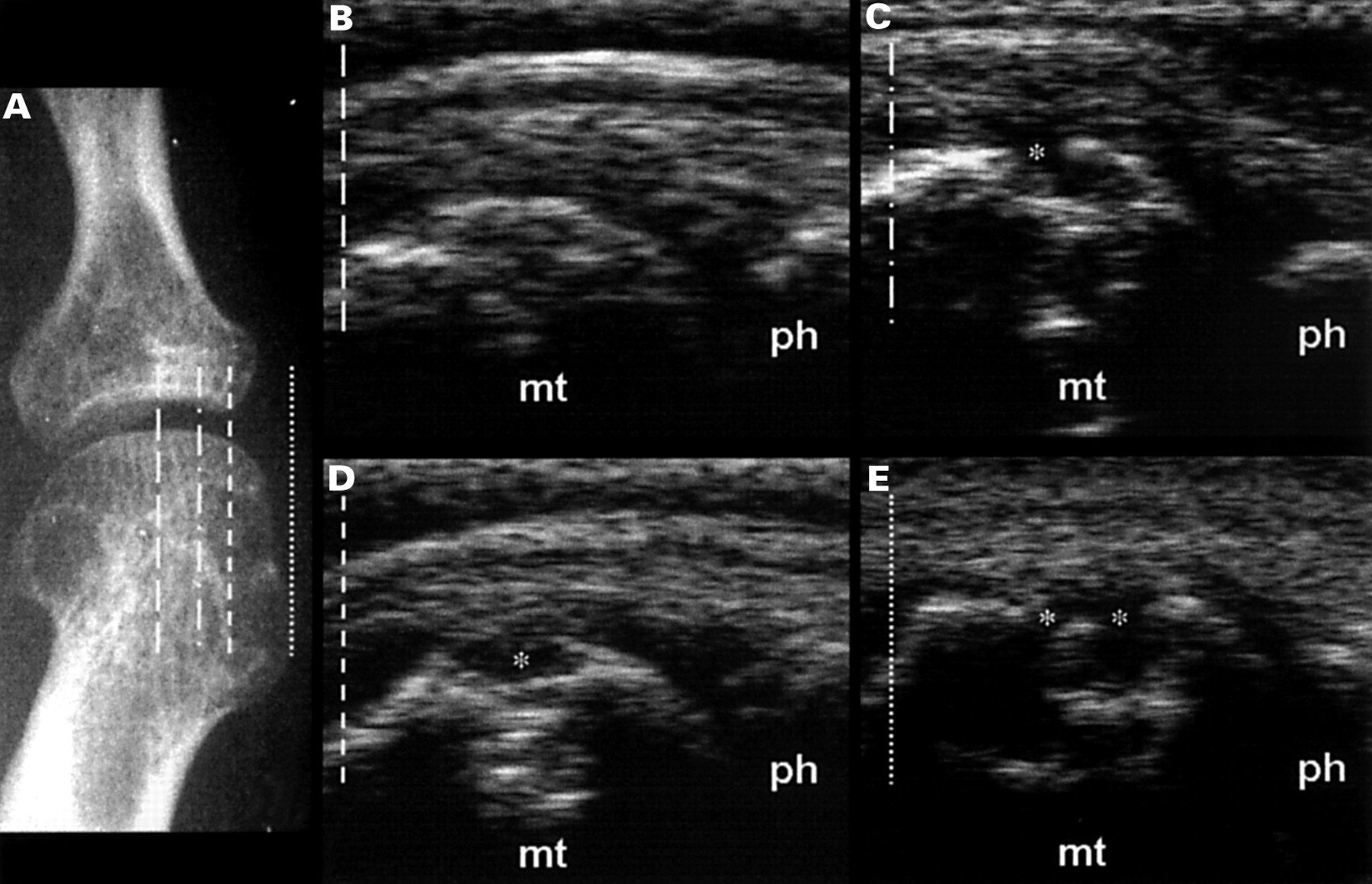
Rheumatoid arthritis. Metatarsophalangeal joint of the fifth toe. Sonographic findings in late rheumatoid arthritis with cystic like areas of bone resorption on posteroanterior view. (A) Standard x ray. (B) Longitudinal dorsal scan between the two areas of bone erosions does not show any interruption of bone margin. (C) Sonographic scan on the border of the erosion. (D) Longitudinal scan in the centre of the area of bone resorption. (E) Coronal scan. * = erosion; mt = metatarsal head; ph = phalanx.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rheumatoid arthritis. Metacarpophalangeal joint of the second finger. (A) Standard x ray. Multiplanar examination in patient with late disease. Ultrasonography is able to depict the extent of bone resorption both on longitudinal (B and C) and transverse scans (D). mc = metacarpal head; ph = phalanx; * = erosion.
Discussion
Multiple imaging modalities are currently available to explore bone and soft tissue involvement in RA.7 ,15 Standard radiology is still the best method for detecting and monitoring erosive changes.16-18 Early depiction of erosions by ultrasonography may have a useful role in assessing the course of the anatomical damage in patients with RA.19
This pictorial essay aimed at demonstrating that ultrasonography with very high frequency transducers can depict bone erosions, especially in the early target areas of bone resorption (second MCP and fifth MTP joints).20-24 These joints can be carefully explored because of the multiplanar capability of ultrasonography.
Our preliminary investigation of a representative group of patients with RA shows that last generation ultrasonography equipment allows a safe, quick, inexpensive, and accurate identification of small bone erosions.
Despite the lack of standardised criteria for sonographic assessment of bone erosions in RA, our pictorial essay provides a convincing evidence of the capabilities of ultrasonography in clearly depicting small erosions, even when they appear as a vanishing aspect of the cortical plate on standard x ray. Because the appearance of bone erosions on radiographs of a patient with a recent onset arthritis indicates a poor prognosis, the possibility of demonstrating small hidden erosions at the level of the early targets of the disease opens up interesting perspectives of research. Further studies are needed to validate this technique and to evaluate the relation between sonographic findings and those obtained with other imaging techniques (standard radiology, magnetic resonance).
References
Footnotes
Supported by Università degli Studi di Ancona grant Ref. n.601 17–03–1999.