Article Text

Abstract
OBJECTIVE To evaluate the clinical significance of antifilaggrin antibodies (AFA) measured by an enzyme linked immunosorbent assay (ELISA) in serial specimens from patients with recent onset rheumatoid arthritis (RA).
METHODS Filaggrin was purified from human skin and used as an antigen in ELISA. The AFA test was applied to five serial specimens from 78 patients with recent onset RA followed up for three years. Rheumatoid factor (RF) had been measured earlier from the same samples by quantitative immunoturbidimetry.
RESULTS The mean AFA level was highest at entry (54% positive), followed by a statistically significant decline at six months and a slight increase at three years. AFA were persistently positive in 23 patients and persistently negative in 28 patients. Eleven of the latter patients were persistently negative for RF. At study entry AFA levels correlated to some degree with RF levels. In general, raised AFA levels at entry were associated with an active and treatment resistant disease, but they did not predict radiological progression.
CONCLUSIONS The test for AFA has potential for an additional immunological test for RA.
- rheumatoid arthritis
- antifilaggrin antibodies
Statistics from Altmetric.com
Rheumatoid arthritis (RA) features several different autoantibodies,1 some of which are specific enough to serve as diagnostic and prognostic markers.2 Rheumatoid factor (RF) and two closely associated antibodies, antikeratin antibody (AKA) and antiperinuclear factor (APF), may even precede the onset of RA2 and at all events, most patients who produce these antibodies are positive already at the initial presentation of clinical symptoms.3-5 Thus these antibodies are not secondary manifestations of inflammation or tissue destruction.
The detection of AKA and APF is based on indirect immunofluorescence techniques, in which the substrates are not standardised. Technical difficulties have limited the use of these tests in clinical work. Both these antibodies are directed against proteins closely related to human epidermal filaggrin.6 ,7 We have described a method of purifying filaggrin from human skin and using it in an enzyme linked immunosorbent assay (ELISA) to measure antifilaggrin antibodies (AFA).8 Recently, AFA have been detected by immunoblotting on human semipurified or purified filaggrin.9 ,10 Also, synthetic peptides containing reactive antigenic sites of filaggrin have been used in ELISA.11 One of the immunoblotting studies showed a correlation between AFA and AKA,9 whereas the other showed a very low frequency of positive reactions for AFA.10 The test based on synthetic peptides showed a fairly good correlation with APF.11
We earlier measured RF by quantitative immunoturbidimetry in serial specimens from patients with recent onset RA.12 AFA have been shown to be specific serological markers in RA. In this study we investigated antifilaggrin ELISA on these patients.
Patients and methods
PATIENTS
Seventy eight consecutive patients (63 women, 15 men) with early RA satisfying the American Rheumatism Association (ARA) 1987 classification criteria were included in the study. At entry, the mean age of the patients was 43.5 years (range 19–65) and the mean duration of symptoms was 7.6 months (range 2–12). None of the patients had received any disease modifying antirheumatic drug (DMARD) treatment before entry into the study. Intramuscular gold was started in 63 patients, sulphasalazine in 12, and hydroxychloroquine in three. Three patients used concomitant low dose prednisone (5–7.5 mg daily).
Clinical and laboratory assessment of disease activity included Ritchie articular index, number of swollen joints, morning stiffness, pain by the visual analogue scale, disease activity score (DAS),13erythrocyte sedimentation rate (ESR), and C reactive protein (CRP) at entry, and at 6, 12, 24, and 36 months.
Radiographs of hands and feet were taken at entry to the study and thereafter annually during the follow up. The xrays were evaluated by the method of Larsenet al.14
LABORATORY METHODS
Blood samples for the determination of AFA and for RF were taken at entry and at 6, 12, 24, and 36 months (during 1986–91). All serum samples were stored at −20°C until analysed.
Filaggrin was purified from human epidermis as described earlier.8 Briefly, epidermis was cleaved from dermis by incubation at 56°C in 10 mM potassium phosphate buffer, pH 7.
The epidermal layer was peeled off, homogenised in a mortar, sonicated, centrifuged, and delipidated. The extracted proteins were chromatographed in reverse phase high performance liquid chromatography. Fractions containing filaggrin were identified in immunoblotting by monoclonal AFA, pooled, and subjected to gel filtration and again to reverse phase chromatography. The identity and purity of the protein were further confirmed with tryptic digestion, peptide separation, amino acid sequencing, and mass spectrometric analysis of the formed peptides. The yield of purified filaggrin was of the order of 50–100 μg from each gram of epidermis (wet weight).
ELISA for AFA was performed as described in detail elsewhere.8 Briefly, microtitre plates (Nunc, Roskilde, Denmark) were coated with filaggrin (3 μg/ml in 50 mM carbonate buffer, pH 9.6) and post-coated with 1% human serum albumin. Patient and control serum samples were diluted 1:500 in duplicate, and binding of IgG class antibodies to solid phase filaggrin was demonstrated by alkaline phosphatase conjugated, γ chain-specific antihuman IgG antibodies. Cut off levels for positivity were determined on the basis of results of serum samples from 100 middle aged (40–65 years) blood donors. Five subjects had an optical density value ⩾0.15, which was taken as the cut off point for positivity. Another control series comprised 30 healthy subjects with the same age distribution as the patients and whose serum samples had been collected and stored identically. For these controls, mean + 3SDs corresponded to 0.15 optical density units. Interassay coefficient of variation of the method was 3% for a high positive reference serum and 8% for a low positive serum.
A Kone specific automated clinical chemistry analyser (Kone Instruments, Espoo, Finland) was used for immunoturbidimetric measurement of RF and a modified assay using chemical inactivation of C1q with polyvinyl sulphonate was used as previously described.15 When this method was used, 381/403 healthy subjects (95%) had an RF <20 IU/ml,15 which was taken as the cut off point for positivity. According to the manufacturer, standards in the test kit had been calibrated against the WHO standard serum.
To eliminate possible intertest error, all specimens from each patient were always tested on the same occasion.
STATISTICAL METHODS
Differences between groups were analysed with the Wilcoxon test for paired data and the Mann-Whitney test for unpaired data. Correlations were calculated with Spearman's correlation coefficient test. The area under the curve (AUC) was used as a summary measure to integrate serial assessments of disease activity and AFA levels (at months 0, 6, 12, 24, and 36).16
The radiographic progression (delta Larsen) was measured as the absolute difference between total Larsen scores at month 0 and 36 months.
Results
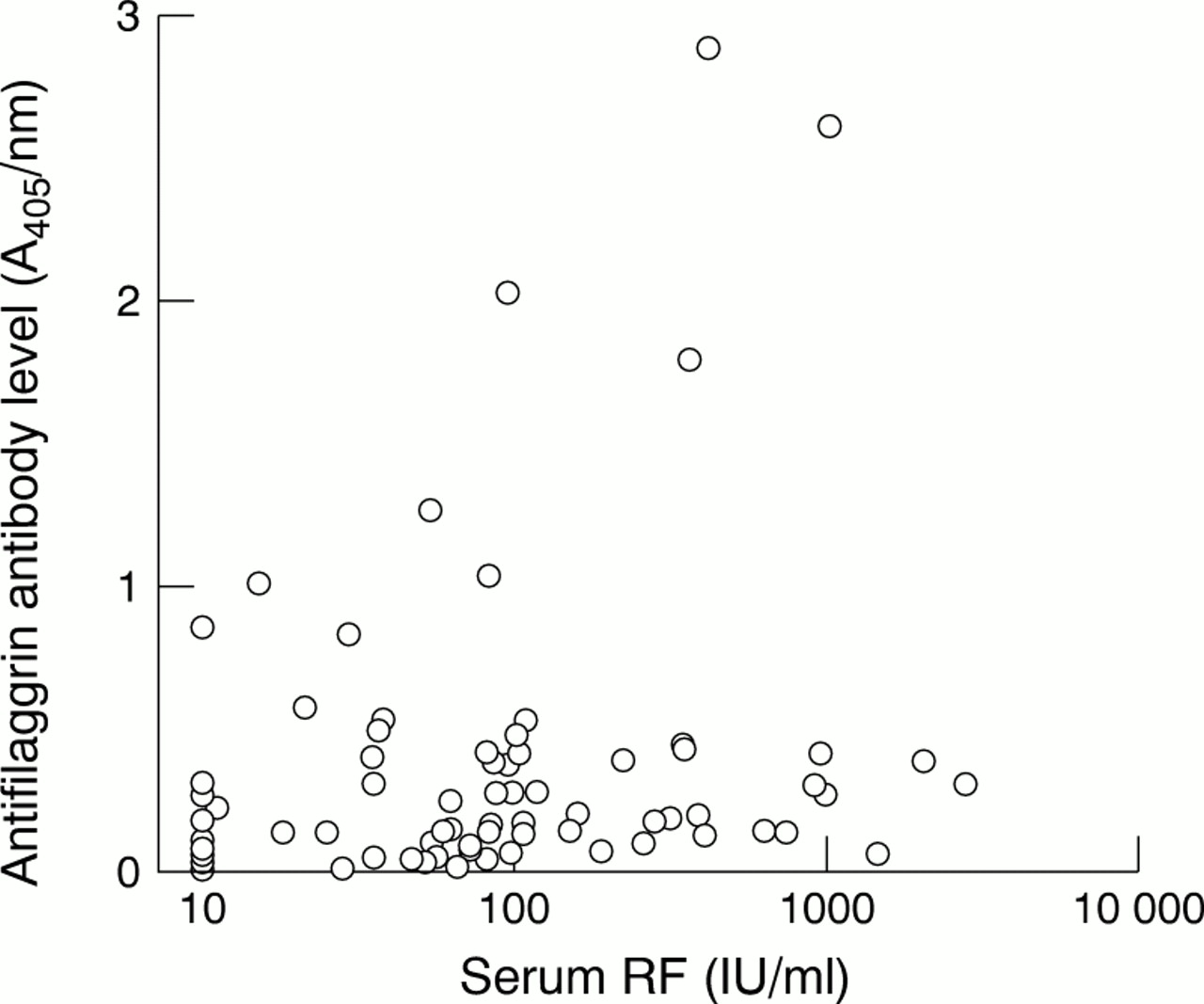
Figure 1 depicts the quantitative correlation between RF and AFA levels at entry (rs =0.30, p=0.001). Thirty six patients were positive and 13 patients were negative in both tests. Twenty three patients were positive only for RF and six patients only for AFA. Thus 58/78 (76%) of the patients were RF positive and 42/78 (54%) were AFA positive. Some patients strongly positive for RF were AFA negative and vice versa. The Spearman rank correlation between the two tests was 0.30 (p<0.01).

{kind=link}
Correlations between antifilaggrin antibody and rheumatoid factor (RF) levels at entry to the prospective study in 78 patients with early rheumatoid arthritis.
The mean AFA level was highest at study entry, followed by a significant decline at six months (p=0.001) (table 1). Some increase was noted at three years. AFA were persistently positive in 23 patients, persistently negative in 27 patients, and the results varied in 28 patients (13 from positive to negative, 5 from negative to positive, and 10 varying). In many instances the changes were borderline. Yet in 10 instances a change of ⩾0.3 optical density units was noted. In three of these patients the test reverted from negative to positive; these patients can thus be regarded as definite late seroconversions.
Antifilaggrin antibody level (A405 nm) in the follow up specimens
RF was persistently positive in 17 patients, persistently negative in 13 patients and the results varied in 48 patients. Of the 17 patients persistently positive for RF, AFA were persistently positive in 10 patients and persistently negative in one patient; the results varied in six patients. Of the 13 patients persistently negative for RF, AFA were persistently negative in 10 patients and the results varied in three patients. Owing to the more frequent reversal of RF from positive to negative, as many as 15 patients were AFA positive but RF negative at six months. At three years, there were only seven such cases.
To look for correlations of the AFA levels with the clinical parameters, AFA levels at entry were divided into three tertiles and patients belonging to the lowest tertile and the highest tertile were compared. Table 2 shows that patients belonging to the highest tertile had significantly higher CRP concentration and Larsen's score at entry to the study. After three years, significant differences were noted in the Richie index, number of swollen joints, length of morning stiffness, visual analogue scale of pain, and DAS, with patients in the highest tertile having more severe disease.
Mean (median) clinical, laboratory, and radiological data of patients with initially highest (n=25) and lowest tertile distribution (n=26) of antifilaggrin antibody (AFA)
There were weak correlations between AUC AFA and AUC ESR (rs =0.24, p=0.05), and between AUC AFA and AUC DAS (rs =0.24, p=0.05). No significant correlations were found between AUC AFA and AUC other variables of disease activity or Larsen score (data not shown).
The baseline AFA levels did not correlate with the radiographic progression (delta Larsen) (rs =0.15, p=0.17).
Discussion
We compared the behaviour of quantitative tests for AFA and RF in serial specimens from patients with early RA using assay conditions in which cut off points for positive reactions were adjusted to the same specificity level for both tests. It was found that the level of these two antibodies fluctuated considerably during the three years of follow up.
Earlier studies on serial APF and AKA measurements showed that positivity in these tests is fairly stable, though conversions from positive to negative and vice versa do occur. The present results suggest that these seroconversions are due to true changes in the antibody levels and not, for example, to technical variation or inaccuracy in the assays.4 ,17 It has been pointed out that serial measurements of APF in longitudinal studies do not give more information than a single determination.17 In our study a statistically significant decline in the AFA levels was seen after starting DMARD treatment and a number of patiens reverted from positive to negative; some of these patients became positive again at a later stage. However, fluctuation of RF levels, as shown by reversals from positive to negative and vice versa, was appreciably greater than fluctuation of AFA levels. A feature common to RF and AFA was that the prevalence of positive reactions was highest at presentation; only a few cases negative at presentation became positive at a later phase. Our data on AFA cover only the first three years of the disease. Possibly, the fluctuation in AFA levels in advanced disease is less distinct than in the early phase. Another point that has to be taken into account is that we measured (in accordance with other authors) only AFA antibodies of IgG class, whereas the immunoturbidimetric RF test measures predominantly IgM class RF.18
RF is the only immunological test for RA among the ARA 1987 classification criteria for RA. However, RF is neither uniformly present nor specific for RA. Thus there is a place for another diagnostic test for RA that is either more specific than tests for RF or is positive in a substantial proportion of RF negative patients with RA.
In the study described here the test for AFA proved to be somewhat less sensitive than that for RF. At entry to the study only a few RF negative patients were positive for AFA; after the start of DMARD treatment the proportion became larger. However, a fairly poor correlation was found even at entry between the levels of these two antibodies. Thus although both RF and AFA are markers of the same underlying immunological process of RA,19 they probably reflect different facets of the process and, hence, may complement each other.
The present series comprised patients in whom a firm diagnosis had been reached and DMARD treatment started soon after the onset of symptoms. The typical features of RA, however, may not always be present from the beginning and there can be a delay in the establishment of a firm diagnosis. Testing for AFA may provide useful information in cases initially presenting as undifferentiated arthritis.20 AFA levels also correlated with increased disease activity in these patients. However, they did not correlate with radiographic progression.
The antigen used in the AFA ELISA was prepared from human skin, thus the test is a useful reference for AFA assays that use other putative antigen substrates, such as heterologous or recombinant filaggrins or peptides corresponding to the filaggrin sequences. Recently, Schellekens et al, using synthetic peptides, provided evidence that citrulline, a post-translationally modified arginine residue, is an essential constituent of antigenic determinants recognised by antibodies reacting with filaggrin.11