Article Text

Abstract
Objectives: To investigate the efficacy and tolerability of allopurinol as the first-choice antihyperuricaemic treatment for gout, and compare the efficacy and tolerability of benzbromarone and probenecid as second-choice treatment.
Methods: Prospective, multicentre, open-label, two-stage randomised controlled trial in gout patients with normal renal function. Enrolled patients were given 300 mg allopurinol for 2 months (stage 1). Those patients who could not tolerate allopurinol or who did not attain the target serum urate concentration (sUr) ⩽0.30 mmol/l (5.0 mg/dl), which was defined as successful, were randomised to benzbromarone 200 mg/day or probenecid 2 g/day for another 2 months (stage 2).
Results: 96 patients were enrolled in stage 1. 82 patients (85%) were eligible for the analysis at the end of stage 1: there was a mean (SD) decrease in sUr concentration of 35 (11)% from baseline; 20 patients (24%) attained target sUr ⩽0.30 mmol/l; and 9 patients (11%) stopped allopurinol because of adverse drug reactions.
62 patients were enrolled in stage 2. 27 patients received benzbromarone (3 patients not eligible for analysis) and 35 received probenecid (4 patients not eligible for analysis). Treatment with benzbromarone was successful in 22/24 patients (92%) and with probenecid in 20/31 patients (65%) (p = 0.03 compared with benzbromarone). Compared with baseline values, there was a mean (SD) decrease of sUr concentration of 64 (9)% with benzbromarone and 50 (7)% with probenecid (p<0.001).
Conclusion: This study showed that allopurinol 300 mg/day has a poor efficacy and tolerability profile when used to attain a biochemical predefined target level of sUr ⩽0.30 mmol/l, following 2 months of treatment. In stage 2, benzbromarone 200 mg/day was more effective and better tolerated than probenecid 2 g/day.
Trial registration number: ISRCTN21473387.
Statistics from Altmetric.com
Allopurinol is the drug of choice for long-term urate-lowering therapy in the 2006 European League Against Rheumatism (EULAR) evidence-based recommendations for gout. Uricosuric agents such as probenecid and sulfinpyrazone can be used as alternatives, and benzbromarone is only recommended in patients with mild to moderate renal insufficiency. Given the scarce clinical trial data, it remains questionable whether the efficacy–safety balance of benzbromarone and probenecid is unfavourable compared with the first choice treatment, allopurinol.1
Since the introduction of benzbromarone in the early 1970s, three cases of severe hepatitis have been published.2–4 Benzbromarone, however, seems well tolerated in general use.5 In contrast, allopurinol rather frequently causes allergic skin reactions (2–5%) and in rare cases even a life-threatening hypersensitivity syndrome.6–10 In Europe, benzbromarone used to be available as a prescription drug in a limited number of countries. In the Netherlands, the only alternative in chronic gout was allopurinol. When allopurinol treatment was unsuccessful, the uricosuric drug probenecid was available for restricted use. Benzbromarone was withdrawn from the market in Europe in 2003, but was registered again in some countries in 2004.11 Its use is now restricted for patients with gout who are allergic to allopurinol or those in whom allopurinol is contraindicated.
The goal of serum urate (sUr)-lowering treatment is to reduce the sUr level below the threshold of supersaturation, to prevent any gouty attack by allowing the dissolution of existing monosodium urate (MSUr) crystals in the joints and to prevent the deposition of new crystals in cases of severe tophaceous accumulation.7–10 The solubility of urate in joint fluids is influenced by temperature, pH, concentration of cations, level of articular dehydration and the presence of nucleating agents, such as insoluble collagens, chondroitin sulphate and non-aggregated proteoglycans.7
According to the EULAR 2006 recommendations, treatment goal of sUr-lowering therapy is to reach target serum urate concentrations below 0.36 mmol/l (6.1 mg/dl).12 Recurrent gouty attacks are better prevented and tophi dissolve more quickly with target serum urate concentrations below 0.30 mmol/l (5.0 mg/dl) rather than 0.30–0.36 mmol/l.13–17 The British guideline (2007) sets the sUr treatment goal for gout patients at ⩽0.30 mmol/l.18
With the aim of collecting more evidence-based data, in the present study we:
investigated the efficacy and tolerability of allopurinol as first-choice sUr-lowering treatment for gout;
compared the above with the efficacy and tolerability of benzbromarone and probenecid as second-choice treatments.
PATIENTS AND METHODS
This prospective, multicentre, open label, randomised controlled trial was carried out in patients recently diagnosed with gout by a rheumatologist. Eligibility criteria were19–22:
a diagnosis of gout confirmed by microscopic evidence of urate crystals or otherwise, complying with the American Rheumatism Association (ARA) criteria;
no history of use of one of the study drugs;
no relevant liver disease;
no relevant renal disease—defined as calculated creatinine clearance (cCrCl) ⩾50 ml/min, using the Cockcroft and Gault formula;
an indication for sUr-lowering therapy: presence of tophi or frequent attacks (>2/year).
Before a patient was entered the study, we measured their liver function, serum creatinine (sCr), sUr, urinary creatinine excretion (uCr) and urinary urate excretion (uUr) on unrestricted purine diet. Underexcretion of urate was defined as urate clearance (UrCl) <6.0 ml/min/1.73 m2.23 Urate clearance was calculated by urinary volume (ml/min) × urinary urate concentration/sUr and normalised for a body surface area of 1.73 m2. Overproduction of urate was defined as uUr >6.0 mmol/day. Normal excretion of urate was defined as UrCl ⩾6.0 ml/min/1.73 m2 and uUr ⩽6.0 mmol/day.
At the time of inclusion in the study, patients were assigned an inclusion number by the rheumatologist (blinded), and consequently randomised to stage 2 treatment. A computer-generated central randomisation schedule with a block size of six was used. The period of study recruitment and follow-up was from June 2005 until January 2007.
In stage 1, patients were given allopurinol 300 mg single daily dose in a step-up dosage scheme (100–200–300 mg/day, with the dose increased every week), which is a common fixed-dose regimen used in clinical practice in Europe and in other gout studies.12 24–26 When allopurinol was not tolerated or when the treatment goal of sUr ⩽0.30 mmol/l was not reached after 2 months, patients were switched to stage 2 treatment: benzbromarone 200 mg single daily dose (Desuric; OTL Pharma, Breda, The Netherlands) – step-up 100–200 mg single daily dose, dose increased after 1 week – or probenecid 1000 mg twice daily (Probenecid Weimer; Biokanol Pharma, Rastatt, Germany) – step-up 500–1000 mg twice daily, dose increased after 1 week. Defined daily doses are allopurinol 400 mg/day, benzbromarone 100 mg/day and probenecid 1000 mg/day. We used a fixed dose in the upper dosage range of benzbromarone and probenecid, because (1) adequate treatment of patients refractory to allopurinol (standard) treatment was warranted, and (2) benzbromarone 200 mg/day had not been tested in a clinical controlled trial before. Colchicine 0.5–1 mg/day was prescribed for prophylaxis of gouty episodes, until the target sUr level was reached (sUr ⩽0.30 mmol/l); when colchicine was not tolerated, a non-steroidal anti-inflammatory drug was prescribed.
Each treatment regimen was evaluated after a treatment period of 2 months by measuring sCr, sUr, uCr and uUr. To evaluate patient adherence for allopurinol, we measured the serum oxipurinol level by using a validated high-pressure liquid chromatography with ultraviolet detector (HPLC-UV) method.27 Patients with serum oxipurinol concentrations below the lower limit of quantification (<1.0 mg/l) were excluded from the analysis.
The primary end point for stages 1 and 2 was the percentage of patients tolerating the antihyperuricaemic medication and attaining an sUr concentration below 0.30 mmol/l. Our secondary end point was the relative decrease of sUr concentration attained with each treatment regimen.
The study was approved by the medical ethical committees of both centres and informed consent was obtained from all participating patients.
Statistics
A power calculation indicated that at least 29 evaluable patients were needed in each treatment arm in stage 2 to prove a statistically significant difference between benzbromarone and probenecid (based on an estimated 90% success rate for benzbromarone versus 60% for probenecid, α = 0.05, β = 0.20).28 We expected a success rate of 20% with allopurinol and a loss to follow-up of 25%, rendering a total of 96 patients for the study. SPSS version 15.0 was used for data collection, data validation, data selection and statistical analysis. The Student two-sided t test and Fisher exact test were used to compare the effectiveness of benzbromarone and probenecid; 95% confidence intervals of proportions were calculated using binomial distribution. Normality was verified with Kolmogorov–Smirnov analysis. A p value <0.05 was considered statistically significant.
RESULTS
We enrolled 96 patients in stage 1 (fig 1). Three patients did not fulfil the inclusion criteria (estimated CrCl <50 ml/min), leaving 93 patients for analysis of baseline characteristics (table 1). Of these, 82 patients (88%) were eligible for analysis at the end stage 1; five patients were lost to follow-up and six patients were excluded because of poor adherence based on non-measurable serum oxipurinol levels.

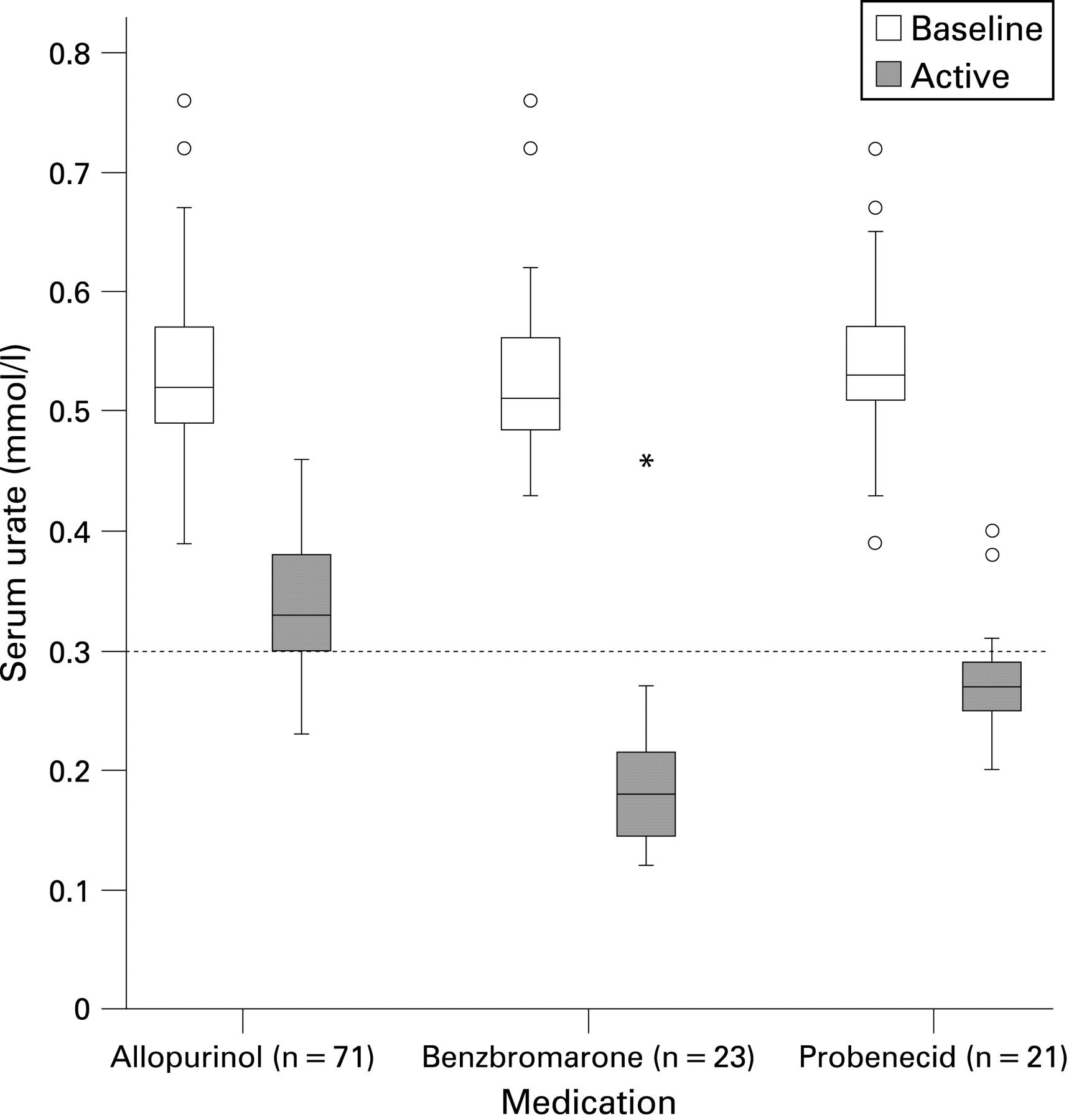
Results of stages 1 and 2 are presented in table 2 and fig 2. In 20 patients (24%) the treatment was successful, defined as tolerance of allopurinol and attainment of sUr concentrations ⩽0.30 mmol/l. Nine patients (11%) stopped taking allopurinol because of adverse drug reactions (ADRs) (table 3). In stage 1, the mean (SD) decrease in sUr concentration with allopurinol was 35 (11)%. The mean (SD) serum oxipurinol concentration measured was 13.2 (7.1) mg/l. Of patients whose sUr concentrations did not reach ⩽0.30 mmol/l, 92% had serum oxipurinol concentrations >5.0 mg/l.
{kind=link}
{kind=link}
A total of 62 patients entered stage 2 of the study: 27 patients received benzbromarone (3 patients not eligible for analysis) and 35 received probenecid (4 patients not eligible for analysis). In the benzbromarone group, 22/24 patients (92%) were treated successfully in terms of tolerance of study medication and attainment of target sUr concentrations. In the probenecid group, 20/31 patients (65%) were treated successfully, which was significantly less than the treatment success attained with benzbromarone (p = 0.026). The success ratio benzbromarone:probenecid was 1.42 (95% CI 1.07 to 1.89). With benzbromarone 200 mg/day, the sUr concentration decreased by a mean (SD) of 64 (9)% compared with a decrease of 50 (7)% with probenecid 2 g/day (p<0.001).
DISCUSSION
This study shows that allopurinol 300 mg/day has a poor efficacy and tolerability profile in patients with normal renal function at 2 months’ follow-up. With a treatment target sUr concentration of ⩽0.30 mmol/l, 24% of patients were treated successfully with allopurinol 300 mg/day. The target sUr concentration is still being debated.29 In the recent EULAR recommendations a more conservative target sUr concentration of ⩽0.36 mmol/l is proposed for gout treatment in general, whereas in patients with severe gout, the treatment target might be lower.12 If we had set a target of ⩽0.36 mmol/l in the present study, we would have achieved a treatment success rate of 56% using allopurinol 300 mg/day. A higher success rate with allopurinol 300 mg/day might be achieved in patients with less severe gout who have a lower baseline sUr, and in overproducer-type patients.
The limited efficacy and modest sUr-lowering effect of allopurinol with the recommended dose of 300 mg/day is consistent with previous findings.24–26 28 Recent guidelines recommend increasing the allopurinol dose, when necessary, until the target sUr concentration is attained, with a maximum dose of 900 mg/day.12 18 However, switching to uricosuric therapy might be preferable, because of several reasons. First, considering that steady state serum urate concentrations depend on the mass balance (difference between input and output) of urate in the body, the sUr-lowering potential of xanthine oxidase inhibitors is limited compared with uricosurics, especially in underexcretor gout patients with a mean uUr of 2.2 mmol/day. Second, uncertainty exists about the efficacy–safety balance of higher doses of allopurinol. Lastly, in routine clinical practice and in virtually all clinical research, the commonly used dose is 300 mg/day. In one case series, 19 gout patients were treated with allopurinol 600 mg/day: serum urate decreased in 44 (13)% and 52% of patients attained the target serum urate concentration ⩽0.30 mmol/l.30 In patients with normal renal function, there is no evidence for a direct relationship between allopurinol or oxipurinol concentrations and the occurrence of adverse effects.31 On the other hand, in patients with renal insufficiency, accumulation of oxipurinol is considered a crucial factor in the development of allopurinol hypersensitivity syndrome, which leads to tissue damage by toxic, immunological and/or genetic mechanisms.32–35
In our study, 11% of patients did not tolerate allopurinol (table 3). This is slightly higher than rates reported in literature (mostly 3–5%), but these differences are probably not significant.12 18 36 The ADRs leading to withdrawal in this study are well documented in the literature, except for fatigue.37
We measured the serum oxipurinol concentrations to verify adherence to allopurinol. Patients with undetectable oxipurinol concentrations (<1.0 mg/l) were excluded from the analysis. The reported reference range for allopurinol 300 mg/day is 5.0–15.0 oxipurinol mg/l.38 Most of the patients who did not attain the target treatment goal had serum oxipurinol concentration >5.0 mg/l (92%). This indicates that these patients were compliant with allopurinol treatment. For the purpose of therapeutic drug monitoring of allopurinol therapy, (re-)assessment of the therapeutic reference values of serum oxipurinol is needed.
In stage 2, we compared benzbromarone 200 mg/day and probenecid 2 g/day. The results showed that significantly more patients attain target sUr concentrations with benzbromarone. The sUr-lowering effects of benzbromarone and probenecid are consistent with previous findings.24–27 39 40 The ADRs reported with probenecid (table 3) are common side effects of this drug.41
This study was conducted in patients with an cCrCl ⩾50 ml/min. The results cannot be extrapolated to patients with renal insufficiency, because of several reasons: allopurinol dose should be adjusted; benzbromarone is considered ineffective in patients with cCrCl <25 ml/min; and probenecid is considered ineffective in patients with cCrCl <50 ml/min.36
We used sUr as a surrogate parameter for clinical success. Previous studies have shown that the attained sUr is inversely related to prevention of recurring gout flares and to velocity of size reduction of tophi.13–17 Therefore, in clinical practice sUr is a well-established parameter for evaluating success of sUr-lowering therapy for gout in the long term.
More than 90% patients in our study were underexcretors of uric acid. From a pathogenic point of view, it has been suggested that allopurinol, as an inhibitor of uric acid production, is more effective in overproducer-type gout patients. However, this view is not supported by clinical data. Previous findings indicate that even patients with apparently high uUr relatively underexcrete urate.42 When treatment goals are not achieved with allopurinol in overproducers, combination with a uricosuric drug (eg, benzbromarone, probenecid) might be useful, considering the (relative) contraindication of uricosuric drugs for patients with urinary urate excretion >4.2 mmol/day.28
Besides the drugs used in this study, there are few therapeutic options available to lower sUr to target concentrations. The uricosuric drug sulfinpyrazone is not widely used due to its adverse effect profile.36 In a recent study, 47–66% of patients taking febuxostat 80–120 mg/day reached sUr concentrations below 0.30 mmol/l compared with only 13% who were taking allopurinol 300 mg/day.24 A new treatment option for patients with severe tophaceous gout, recombinant uricase and pegylated recombinant uricase, seems promising.43–46 In short-term studies, uricase-based drugs have been potentially effective, but they are expensive drugs. The impact of gout on absence from work and productivity is substantial, so pharmacoeconomic studies are necessary, comparing the newer and older (out of patent) drugs, such as allopurinol and benzbromarone.47
It seems that benzbromarone is a highly efficacious oral sUr-lowering drug that has been excessively withdrawn from the market. It may be preferable to reintroduce benzbromarone in the market instead of using the new, costly drugs that carry a risk for unknown ADRs. Worldwide, the treatment of gout may be more successful with better (restricted) availability of benzbromarone.48 49
Acknowledgments
The authors thank the rheumatologists Dr G A W Bruyn, Dr P M Houtman, Dr J P L Spoorenberg (Medisch Centrum Leeuwarden), Dr K W Drossaers-Bakkers, Dr M W M Kruijsen and Dr H H Kuper (Medisch Spectrum Twente) for inclusion of their patients in the study. The authors thank M E J Luiken, P ten Have and M H van Dijk for collection of study data.
REFERENCES
Footnotes
Competing interests: None.
Funding: This work has not been supported by any grant from the pharmaceutical industry, or private or public institutions.
Ethics approval: Ethical approval was obtained.
Patient consent: Obtained.